
Abstract
Background:
The current global COVID-19 pandemic is caused by the novel coronavirus Severe Acute Respiratory Syndrome coronavirus 2 (SARS-CoV-2). Given that SARS-CoV-2 is highly transmissible, surgical societies have recommended that procedures with a high risk of aerosolization be avoided or delayed. However, some high-risk procedures, such as those related to head and neck malignancies, cannot always be delayed. Care must be taken during aerosol-generating procedures to minimize viral transmission as much as possible. Preoperative testing for COVID-19, limited operating room personnel, adequate personal protective equipment, and surgical technique are factors to consider for high-risk procedures.
Methods:
This article presents the case of an awake tracheotomy performed for a transglottic mass causing airway obstruction.
Results:
With detailed planning and specific techniques, the amount of aerosolization was reduced, and the procedure was performed as safely as possible.
Conclusion:
This case provides a template for future aerosol-generating procedures during respiratory pandemics.
Introduction
The novel coronavirus disease 2019 (COVID-19), caused by Severe Acute Respiratory Syndrome coronavirus 2 (SARS-CoV-2), was first described in Wuhan, China, in December 2019. Since that time, the COVID-19 outbreak has rapidly spread throughout the world and has been declared a public health emergency of international concern by the World Health Organization.1–3 Currently, more than 1,400,000 cases of COVID-19 have been documented globally with more than 80,000 deaths. 4 The majority of deaths are associated with acute respiratory distress syndrome, severe pneumonia, and subsequent shock and organ failure. 3 Asymptomatic patients have also tested positive for COVID-19, although the exact number of asymptomatic carriers is unknown due to the lack of testing and the prolonged incubation period.2,3,5
SARS-CoV-2 remains viable in aerosols for at least 3 hours,6,7 leading to the recommendation by the American Academy of Otolaryngology—Head and Neck Surgery (AAO-HNS) to avoid aerosol-generating procedures (AGPs), such as tracheotomy, in patients with COVID-19 when possible. 8 Furthermore, delaying or avoiding tracheotomy reduces the risk of viral transmission to health-care providers and conserves necessary personal protective equipment (PPE). However, in patients with head and neck cancers that cause airway obstruction, tracheotomy may be necessary to protect the airway, diagnose, and treat these patients. Accordingly, the aims of the present study were to review important perioperative considerations for airway management and to discuss an approach to an awake tracheotomy in a patient with a large transglottic mass causing airway obstruction.
Methods
A 64-year-old male with multiple medical comorbidities presented to the Washington DC Veterans Affairs Emergency Department with dyspnea, cough, and stridor for which the otolaryngology service was consulted. He endorsed a 3-month history of dysphonia and globus sensation, and reported a 20 pack-year smoking history with heavy alcohol consumption.
Physical examination was remarkable for stridor, hoarseness, and mild increased work of breathing, and his lab work was notable for a troponin of 0.11 ng/mL (reference range: 0.0–0.7 ng/mL). Flexible fiber-optic laryngoscopic exam demonstrated a transglottic mass emanating from the left true vocal fold (TVF) with subglottic extension. His left TVF was immobile and fixed in the paramedian position, and the right TVF was hypomobile. A computed tomography (CT) scan of the neck with contrast demonstrated a 2.3 cm × 1.6 cm × 1.1 cm lesion along the left TVF, with narrowing of the airway and no cervical metastases (Fig. 1). The patient was subsequently admitted to the hospital, at which time a COVID-19 polymerase chain reaction (PCR) test was negative. Given his tenuous airway, the decision was made to perform an awake tracheotomy with pan-endoscopy and biopsy.

Computed tomography scan of the neck with contrast demonstrating a 2.3 cm × 1.6 cm × 1.1 cm lesion along the left true vocal fold (TVF) with narrowing of the airway, subglottic extension, and no cervical lymph node metastases.
Surgical procedure
Within 24 hours prior to the procedure, a repeat COVID-19 PCR test was performed, and again the results were negative. However, given the risk of a false-negative test, the procedure was performed in a negative pressure operating room as if the patient were infected with COVID-19. PPE was utilized by the surgical team, anesthesia providers, and nursing staff. This included either a powered air purifying respirator (PAPR) or an N95 respirator mask, head cover, face shield, double gloves, surgical gown, and shoe covers.
The patient was positioned in the supine position with a shoulder roll in place. The anesthesiologist administered midazolam, and the patient remained awake and breathing spontaneously throughout the procedure. The anesthesia mask was tightly fastened around the face to prevent a leak, with a high efficiency particulate air (HEPA) filter attached directly to the face mask (Fig. 2). Four milliliters of 1% lidocaine with 1:100,000 epinephrine was administered into the subcutaneous tissues of the neck overlying the cricoid cartilage. The incision was made with a 15-blade, and dissection was carried down to the strap muscles, which were retracted laterally to reveal the thyroid isthmus. The isthmus was transected, and another 2 cc of 1% lidocaine was injected into the tissues overlying the trachea and into the trachea itself to anesthetize the airway. Typically, this aspect of the procedure causes significant coughing and aerosolization of particles. However, using the mask affixed to the face as opposed to a nasal cannula, the amount of aerosolization was diminished. The tracheotomy was made between the second and third tracheal rings, and a 6.0 cuffed Shiley tracheostomy tube was inserted and secured in place. Suctioning the airway was minimal, and stay sutures were not utilized to reduce the duration of this portion of the procedure.

The anesthesia mask was tightly fastened around the face to prevent an air leak. The high efficiency particulate air (HEPA) filter was attached directly to the face mask. This is in contrast to the typical nasal cannula utilized during awake tracheotomy.
The patient was then sedated and paralyzed, and the direct laryngoscopy with esophagoscopy was performed. The procedure revealed an exophytic transglottic mass emanating from the left TVF, crossing the anterior commissure, and extending to the right TVF and into the subglottis (Fig. 3). The cervical esophagus and hypopharynx were clear without masses or lesions. Following the procedure, the PAPRs were cleaned with the proper technique, and the patient was transported back to his room with the HEPA filter in place. Final pathology revealed invasive squamous-cell carcinoma.
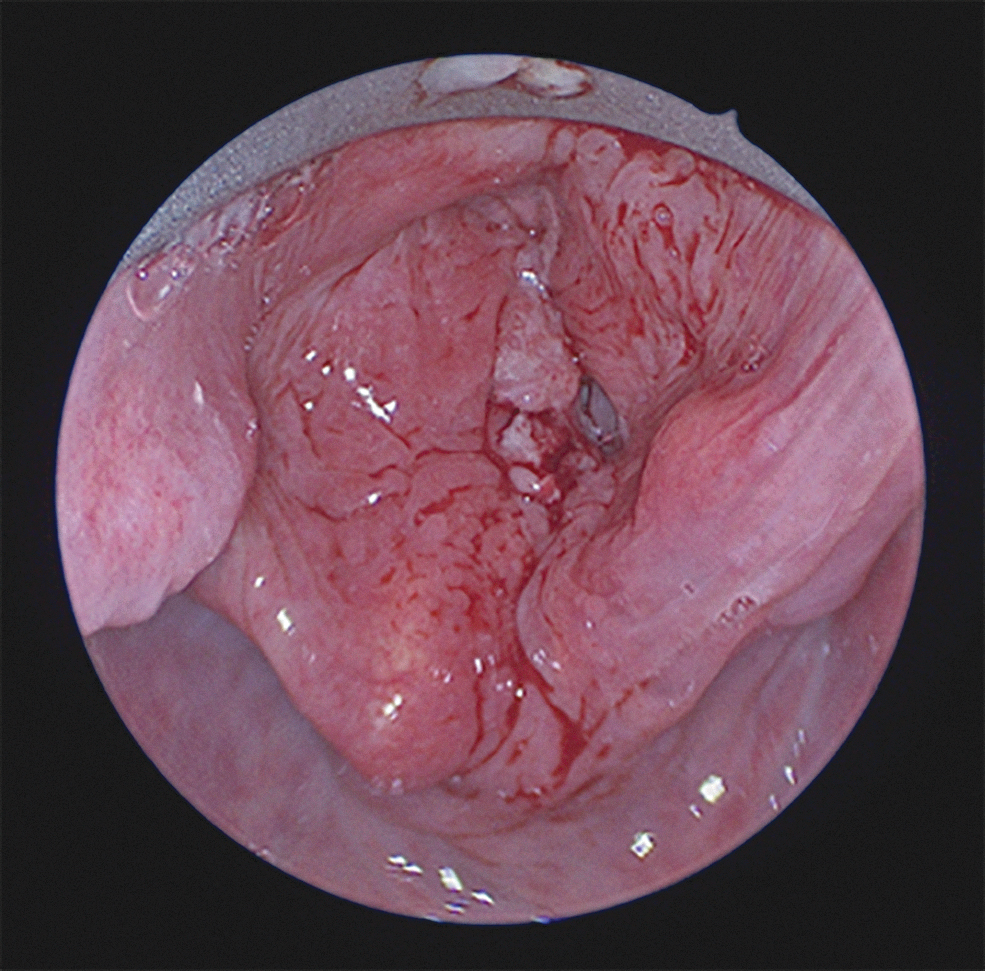
Direct laryngoscopy revealed an exophytic transglottic mass emanating from the left TVF, crossing the anterior commissure, and extending to the right TVF.
Discussion
AGPs, particularly those that cause mucosal disruption, likely have the highest risk for SARS-CoV-2 transmission. 9 Urgent and emergent AGPs pose significant management challenges, in large part due to the current paucity of available literature. Awake tracheotomies are particularly high-risk procedures due to the potential for coughing and airway distress by the nature of the procedure. Therefore, this case demonstrates a conservative approach to performing high-risk procedures during the COVID-19 pandemic.
Guidelines from AAO-HNS recommend waiting to perform tracheotomy in COVID-19-positive patients at least 2–3 weeks from intubation, and preferably with a subsequent negative test. 8 However, there are instances when tracheotomy is necessary and best if performed in a controlled environment as opposed to an emergent scenario. Wei et al. described a case of tracheotomy after failed oral intubation in a patient with SARS from 2003. 10 The authors provided recommendations for emergent tracheotomy during SARS, including limiting personnel, preoxygenation for 5 minutes with 100% FiO2, and use of appropriate PPE similar to that worn in our present case. They recommended paralyzing the patient prior to rapid cricothyroidotomy with subsequent mechanical ventilation via a cuffed tracheostomy tube inserted through the cricothyroid membrane. Similarly, our present case highlights important factors that must be considered for surgical procedures during the current COVID-19 pandemic. These factors include timing of the operation, preoperative viral testing, personnel involved, appropriate PPE, and operative technique.
Recently, Werner et al. suggested that low-grade cancers of the head and neck could potentially be delayed by 1–3 months, as the benefit of minimizing SARS-Cov-2 transmission and preserving PPE may outweigh delay in diagnosis and treatment. 11 The authors also suggested consideration of alternatives to surgery, such as chemoradiation for human papillomavirus-positive oropharyngeal cancers, to prevent aerosolization. In our case, the patient had imminent airway compromise and did not yet have tissue diagnosis of his transglottic mass. As such, delaying the procedure would have compromised his airway and therefore was not an option. Furthermore, the size and location of the mass precluded standard orotracheal or awake fiber-optic nasotracheal intubation, thus necessitating awake tracheotomy.
The role of preoperative viral testing remains under debate. Some suggest that full PPE for all operating room staff, including N95 masks, should still be considered for mucosal operations, despite a negative test, because the true prevalence of community disease is likely higher than reported.9,12 The number and timing of negative tests required to proceed with non-urgent cases has yet to be determined. We believe that multiple recent negative SARS-Cov-2 tests in this patient allowed us to proceed at normal pace safely during this operation. However, if the test had been positive, the primary modification to our current technique would have been to minimize staff to only essential and senior personnel.
Recently, Tay et al. reviewed cases of open tracheotomies performed during the SARS epidemic with attention to techniques that could be employed during the current pandemic. 13 Strategies included full PPE with either N95 masks or PAPRs, negative pressure operating environments, patient paralysis, limiting or avoiding suction and diathermy, and minimizing the number of exposed personnel. None of these cases, however, was performed urgently on a patient who was awake.
Our technique to minimize aerosolization included securing a face mask tightly to the nose and mouth as opposed to the typical use of nasal cannula. The face mask remained in place until the tracheostomy tube was secured and connected to the anesthetic circuit. We believe this modification could have utility for future awake tracheotomies during the current pandemic to reduce the risk of viral transmission. Implementing recommendations for elective tracheotomies, such as minimizing suctioning and using in-line suctioning if needed, further reduces transmission risk.12,14
Conclusion
We describe the first reported case of an awake tracheotomy during the COVID-19 pandemic. A secured face mask was used for secretion management prior to insertion of the tracheostomy tube. This technique, when combined with previously published recommendations for elective tracheotomies, may assist in minimizing risk of viral transmission for awake tracheotomies performed during the current pandemic.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.