
Abstract
The COVID-19 outbreak has dramatically impacted our activities of pediatric surgeons and urologists over the past 3 months, especially in the field of minimally invasive surgery (MIS) and robotics. Analyzing the available literature, there is very scarce evidence regarding the use of MIS and robotics for treatment of pediatric surgical and urological pathologies during this pandemic. However, we found some useful information that we would like to share with other pediatric surgeons and urologists through this journal.
Based upon the available data, we believe that surgery should only be performed in pediatric patients with emergent/urgent and oncological indications until resolution of the COVID-19 outbreak. Robotics and MIS may be safely performed in such selected children by adopting specific technical precautions such as prevention of aerosol dispersion using filters/suction or adapted systems and appropriate use of electrocautery and other sealing devices for reduction of surgical smoke, as reported in our recent experience. Another key point to manage this pandemic emergency is that all hospitals should provide health care professionals with adequate individual protections and perform universal screening in all patients undergoing surgery. Considering that this pandemic is a rapidly evolving situation with new information available daily, these data resulting from the analysis of literature focused on pediatric robotics and MIS may be further revised and updated.
The COVID-19
Analyzing the available literature, there was very scarce evidence about this subject. However, we found some useful information that we would like to share with the readers of Journal of Laparoendoscopic & Advanced Surgical Techniques.
There are two critical points: (1) protection of surgeons and all health care professionals, who may be exposed to COVID-19+ patients and also nondiagnosed, asymptomatic, but contagious COVID-19+ patients who may become potential vectors during anesthesiologic maneuvers, surgical procedure, and postoperative care and (2) protection of patients. Several guidelines have been published until now in different surgical specialties in an effort to help surgeons in the management of their patients.1–8 First, it has been recommended to limit surgery to urgent/emergent or oncological indications and postpone the surgical treatment of nonemergent conditions after resolution of the COVID-19 outbreak. 9
However, considering that the duration of this pandemic cannot be reliably predicted and different pediatric pathologies, such as obstructive uropathies with high risk of urosepsis and kidney damage, progressive cancers, or various malformations, may require an emergent/urgent surgery, as surgeons, we must be able to manage them while preserving the safety of ourselves, our team, and our patients. Second, some reports described an increased risk of virus spreading associated with laparoscopy and robotics. 10 This risk has been mainly attributed to the “aerosolization” of viral particles during the induction and maintenance of the pneumoperitoneum and the generation of surgical smoke with use of electrocautery devices and sealing devices.11,12
In fact, it has been demonstrated that the size of particles produced by electrocautery (0.007–0.42 μm) and sealing devices (0.35–6.5 μm) allows them to easily reach the lower respiratory tract. 13 As reported in a recent study by Zheng et al., 10 after using electrical or ultrasonic equipment for 10 minutes, the particle concentration of the smoke during laparoscopic surgery was significantly higher than that during open surgery. In addition, in both laparoscopy and robotics, the risk of exposure to the pneumoperitoneum aerosol may be increased by different factors such as sudden release of port valves, nonair-tight instrument exchange, port displacement, or specimen extraction. 10 To date, there is no certain proof that infection of surgical personnel occurs through laparoscopy any more so than open surgery. 14
In their clinical practice, pediatric surgeons must interact with the child and the parents; as a consequence, a higher protection level is needed to avoid large-scale infection among health care professionals due to undiagnosed cases. After analysis of the international literature, we aimed to provide to the pediatric surgery community useful information and specific control strategies to apply in robotics and MIS.
Patient selection: All elective surgeries that can be delayed without any risk for the patient should be postponed to after resolution of the COVID-19 outbreak.6,15 As performed in our divisions, surgery should be reserved to emergent/urgent and oncological indications.
Admission screening: All patients admitted to pediatric surgery service should receive adequate anamnestic interview (the patient and family) about presence of recent symptoms such as fever, cough, or respiratory distress and recent social interaction with a COVID-19+ subject. Before admission, they should also receive body temperature measurement and COVID-19 screening test.6,10 In our hospital, we adopt the (COVID-19) IgG/IgM rapid diagnostic test (RDT) that assays patient antibodies (IgM and IgG) to SARS-CoV-2 or viral antigen from blood samples from a finger prick, saliva samples, or nasal swab fluids. The sensitivity of the RDT ranges between 57% and 81%. 16 The same screening should also be extended to the parent accompanying the patient. Furthermore, only 1 parent should be allowed to assist the child during hospital stay and no visitors should be admitted. 6
General protection of health care professionals: Based upon our current practice, all the rooms in the ward should be set with a single bed during the pandemic to avoid crossing infection between admitted children or their accompanying parents. Considering the possibility of false negative results of COVID-19 RDT, 16 all health care professionals should always wear all appropriate protective disposals, including surgical mask, goggles, face shield, disposable caps, and gloves, before performing routine medical work and especially procedures such as dressing change, drainage removal, or other maneuvers directly exposing to contact with patient's blood, body fluids, or excretions.6,17 Adequate hands cleaning and disinfection using bactericidal alcohol gel should be performed before and after each contact with the patient.6,10
General protection of patients: Patients and accompanying parents should reduce their permanence and wear a mask in the ward public area. 6 The body temperature of patients and accompanying parents should be measured at least twice a day and any symptoms such as fever, cough, or other, appearing during hospitalization, should be referred to the clinicians. 6
General protection of surgical team: Surgical team, including surgeons, anesthesiologists, nurses, and all transiting persons in the operating room (OR), should always wear surgical masks, protective glasses or masks, isolation gown, protective suits, and shoe gloves to protect work clothes, face, and eyes from contamination by spatter of blood, body fluids, or secretions, irrespectively, of known or suspected COVID status of the patient. In case of a suspected or diagnosed COVID-19+ patient, the three-level protection measures must be applied, including FFP2/3 masks with face shield and body protective garb. 18 During robotic procedures, the console surgeon should also wear a sealed visor mask to avoid any contact with droplets, and the head support of the console should be adequately cleaned between surgical cases. 8 Special attention must be paid to prevent sharp wounds or damage of the protective equipment, especially gloves and body protection. 6
OR setting: COVID-19+ patients who need to perform urgent surgery should be operated in a dedicated OR with limited surgical staff following the general recommendations for OR staff protection. 10 If not possible, greater OR turnover time and increased ventilation and air purification should be applied for OR sanitation between surgical procedures. 6
Intraoperative management: Different technical aspects should be carefully managed during robotic and MIS procedures to reduce the risk of viral contamination:
Management of aerosol dispersal: the use of a suction-assisted smoke evacuation device may reduce the risk of gas leakage through trocars during the insertion, manipulation, and instrument change. 10 Surgeons should verify that trocar stopcocks or luer connectors are closed before insertion to avoid unnecessary gas leakage. Skin incisions for ports should be as small as possible to avoid gas leakage around ports. In both robotic and laparoscopic procedures, use of integrated flow system can be advantageous. This must be configured in the smoke evacuation mode that, using a 0.01 μm Ultra Low Penetrating Air (ULPA) Filter according to the guidelines established by the Association of Perioperative Registered Nurses (AORN), 19 allows capturing of particles >0.01 μm and the COVID-19 particle size has been reported in the range of 0.06–0.14 μm. 20 As a consequence, use of such devices with smoke evacuation filters may be helpful to reduce the diffusion of COVID-19 during robotic and MIS procedures.
Management of pneumoperitoneum: after trocars placement, the pneumoperitoneum pressure and CO2 ventilation should be kept as low as possible without compromising the surgical field exposure or patient's safety. 10 The Trendelenburg position's time should be lowered as much as possible to minimize the effect of pneumoperitoneum on lung function and circulation and reduce susceptibility to infection. 10 In our practice, we perform controlled desufflation of CO2 using an adapted suction system consisting of a disposable filter, an endotracheal tube, and a luer connector to attach to one of the working ports before closure, trocar removal, or any extraperitoneal maneuver (Fig. 1). Specimen extraction should be performed after complete CO2 desufflation. The use of a locking grasper to secure the specimen before desufflation may be helpful. Specimen retrieval bags may also be useful to limit the release of fluids during specimen extraction.
Management of surgical devices: use of monopolar coagulation, advanced bipolar devices, or any other sealing devices should be minimized or avoided to prevent the production of excessive surgical smoke and particle aerosolization. If needed, the electrocautery should be adopted using the lowest possible power for the desired effect.10,21
Recommendations for surgery: all robotic and MIS procedures should be performed by experienced surgeons and with the minimum number of surgical team members, to reduce the operating time, the risk of postoperative complications, and viral contamination.6,10 Presence of SARS-CoV-2 nucleic acid has been demonstrated in urine and stools of COVID-19+ patients. 22 Although no evidence of virus transmission through the urines and stools has been reported yet,22,23 certain maneuvers such as bowel handling and opening or urethral and ureteral catheterization during robotic and laparoscopic procedures should be minimized or performed using extreme caution, if pneumoperitoneum is already induced.
Based upon the available evidence, we believe that robotics and MIS may be safely performed in selected pediatric patients during COVID-19 pandemic by adopting specific technical precautions such as prevention of aerosol dispersion using filters/suction or adapted systems and appropriate use of electrocautery and other sealing devices for reduction of surgical smoke, as reported in our recent experience. Another key point to manage this pandemic emergency is that all hospitals should provide health care professionals with adequate individual protections and perform universal screening in all patients undergoing surgery. Considering that this pandemic is a rapidly evolving situation with new information available daily, these data resulting from the analysis of the literature focused on pediatric robotics and MIS may be further revised and updated.
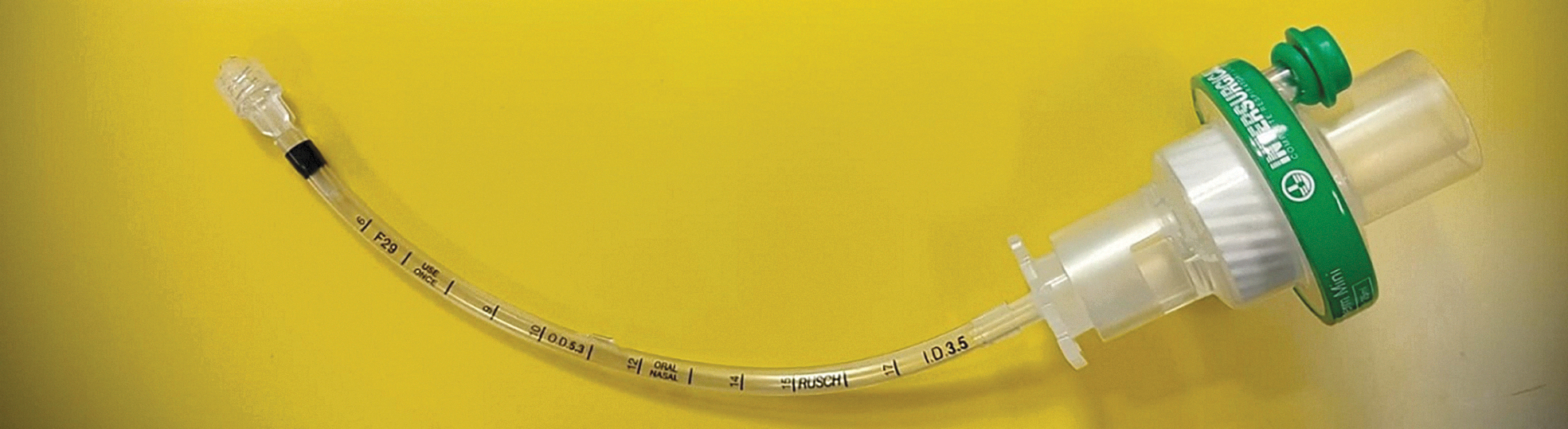
Our adapted suction system consisting of a disposable filter, an endotracheal tube, and a luer connector to attach to one of the working ports for pneumoperitoneum desufflation.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.