
Abstract
The novel coronavirus SARS-CoV-2 (COVID-19) strain has caused a pandemic that affects everyday clinical practice. Care of patients with acute surgical problems is adjusted to minimize exposing health care providers to this highly contagious virus. Our goal is to describe a specific and reproducible perioperative protocol aiming to keep health care providers safe and, simultaneously, not compromise standard of care for surgical patients.
Introduction
The novel coronavirus SARS-C
Patient Presentation
From the first confirmed COVID-19 case in Massachusetts until the stay-at-home advisory was implemented, 2 COVID-19 PUIs required urgent surgical intervention in our institution. The first was an elderly man with multiple comorbidities who presented with fever, severe upper abdominal pain, dyspnea, and significant leukocytosis. Imaging demonstrated acute gangrenous cholecystitis but no acute cardiopulmonary processes. The second was an older woman presenting with right-sided chest and abdominal discomfort, dyspnea, and fever with leukocytosis. Chest X-ray was negative and imaging confirmed acute cholecystitis with an impacted gallstone. Fever and dyspnea prompted COVID-19 reverse transcription (RT)-polymerase chain reaction (PCR) testing and both patients were scheduled for urgent cholecystectomy given the severity of their symptoms. At that time, final RT-PCR testing results took up to 5 days to finalize and thus full precautions were taken perioperatively. Both patients were discharged within 24 hours and final COVID-19 RT-PCR tests were negative.
Perioperative Protocol
A multidisciplinary team from the departments of surgery, anesthesia, infectious diseases and nursing developed and implemented a protocol for PUIs or confirmed COVID-19 patients requiring urgent or emergent surgical procedures (Fig. 1). This protocol consisted of the following key phases:
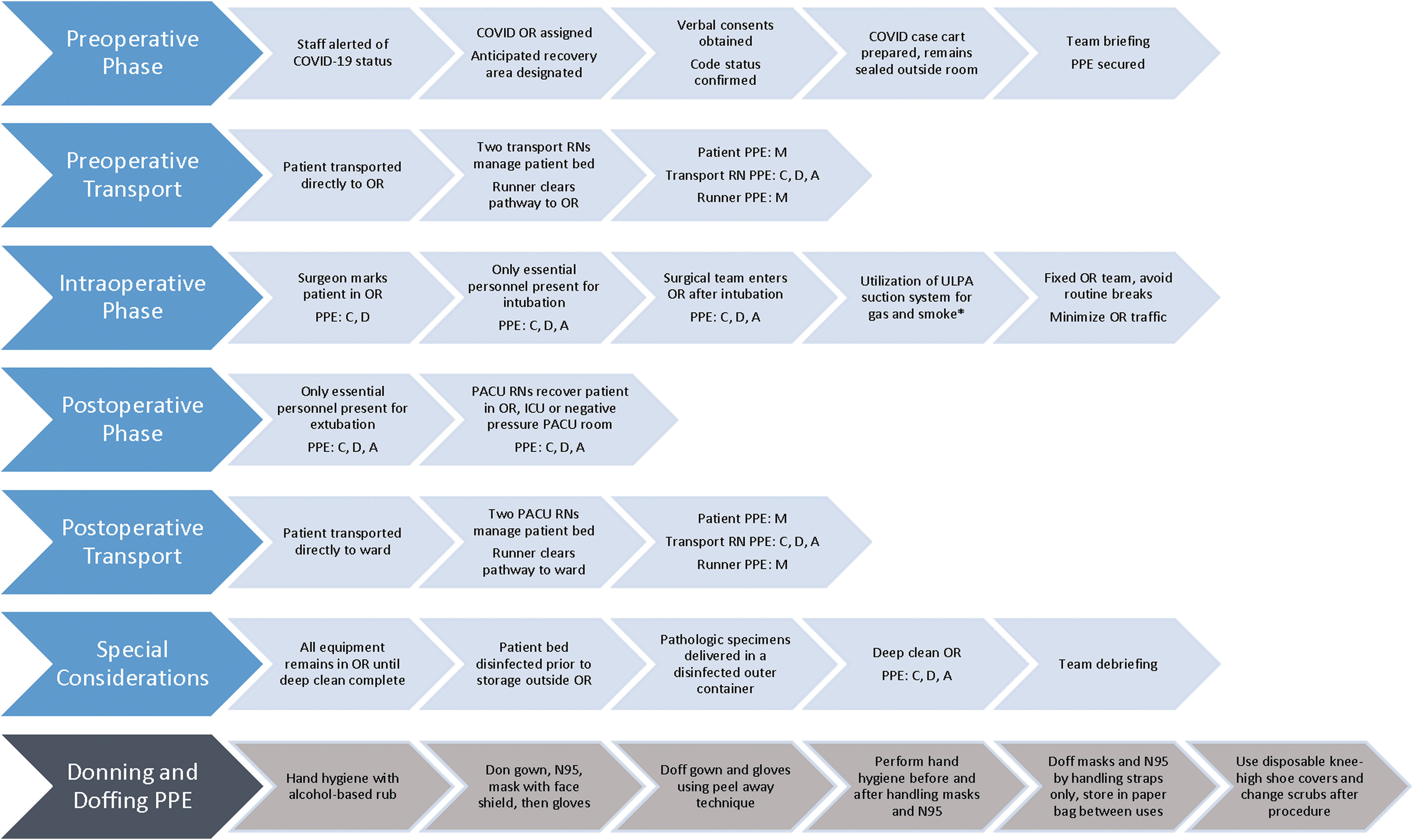
Perioperative protocol phases. *If laparoscopic, ULPA. A, aerosol precautions (N95 mask or PAPR); C, contact precautions (gown, gloves); D, droplet precautions (mask with face shield); M, simple face mask; PPE, personal protective equipment; ULPA, ultra low particulate air suction system.
1. Preoperative phase
Involved staff alerted of COVID-19 PUIs or positive status.
Verbal consents obtained with appropriate witnessed attestation. Code status discussed in advance with the health care proxy/primary care team.
Operating room (OR) case carts, patient care kits, devices not immediately essential to the procedure, and stationary OR cabinets remain sealed outside the OR.
Patient transport was initiated only after OR staff and room were prepared.
2. Preoperative transport phase
Designated transport team (2 OR staff members plus 1 runner to ensure unobstructed entrance to the OR) with appropriate personal protective equipment (PPE).
Immediate passage into OR without stopping at preoperative holding areas or main desk.
Patient ward bed stripped of all linens and bed sterilization were performed.
3. Intraoperative phase
Surgeon signs patient in OR.
Intubation performed with designated disposable GlideScope per anesthesia guidelines.
Surgical team enters the room after intubation. Judicious use of high-speed energy or high-amplitude large-plume generating smoke devices, which may generate aerosolized particles during laparoscopic, thoracoscopic, and open procedures.
Single fixed OR team to minimize exposures and room entry/exit.
4. Postoperative transport phase
Similar to preoperative transport phase.
Patient dons new face mask, clean linens applied to bed before transport.
5. Special considerations
Pathologic specimens to be placed in a disinfected outer container labeled appropriately and delivered directly to the laboratory.
OR deep clean to be performed per institutional protocol for contact/droplet precautions.
All equipment remains in the room until OR deep clean was completed.
Discussion
The algorithm we used to define management of patients requiring urgent or emergent surgical intervention is similar to that previously described. 6 In many cases, COVID-19 RT-PCR testing is submitted before surgical consultation due to presence of symptoms potentially attributable to infection by the novel coronavirus SARS-CoV-2. PUIs for COVID-19 with acute surgical issues should be treated promptly with the appropriate PPE and level of protection. To date we have performed 8 cases following the mentioned protocol. Testing resulted negative for all of them. Special considerations for each phase of perioperative care include the following.
Preoperative phase
Thorough briefing and coordination between patient care teams (emergency room, intensive care unit (ICU), ward) and OR staff are essential for safe and efficient patient transfer. Dedicated transport teams, utilization of negative pressure rooms, when available, and restricting use to only essential surgical instruments for respective procedures can conserve resources and minimize potentially harmful exposures.
Intraoperative phase
The safety of all OR team members (anesthesia, surgery, and nursing) is essential, especially during aerosol generating procedures. Thus utilization of appropriate PPE, maintenance of a fixed OR team, and minimizing OR traffic are vital in preserving PPE and limiting health care worker exposure. If a laparoscopic approach is elected, reduction of the artificial pneumoperitoneum effect on lung function can be achieved by decreasing intra-abdominal pressure when feasible. Given the concern for high viral concentration in surgical smoke after use of electrical or ultrasonic instruments, 7 appropriate smoke and gas evacuation systems should be utilized for filtration of the viral particles and safe completion of the procedure. 8
Postoperative phase
Based on patient stability and available resources, recovery should preferentially be performed in the OR, followed by an established ICU room or lastly, a negative pressure Post Anesthesia Care Unit room. Timely and inclusive team debriefing is essential to identify successful processes and potential challenges.
Health care providers are at an increased risk of exposure to the novel SARS-CoV-2, thus adherence to similar protocols, an essential component of delivering exceptional care to surgical patients, and maintaining a safe working environment.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.