
Abstract
Background:
Obesity is a complex chronic disease, which represents a severe and growing health issue all over the world. Bariatric surgery is an option when medical treatments failed. The average of complications is low. Common bile duct stones in a patient who underwent weight loss surgery, especially Roux-en-Y gastric bypass, one anastomosis gastric bypass, or duodenal switch, is challenging due to the difficult access to the biliary duct.
Methods:
We describe the different techniques we used to perform the treatment of common bile duct stones after a gastric bypass was performed.
Results:
The highlights of the different treatments to solve this big issue that is common bile duct after gastric bypass are described, such as the endoscopic, the surgical, the percutaneous, and combined ones.
Conclusion:
There are several therapeutic options; many of them have already demonstrated excellent results. Even though there is not a gold standard technique, the total endoscopic approach performed by trained hands should be the first line of treatment. Percutaneous approach represents also a safe and effective option that can avoid reoperations in an important number of patients. However, the choice will depend on the severity of the case to face with, the availability of resources, and the experience of the team.
Background
Bariatric surgery represents a safe procedure1–4 ; however, a patient with severe obesity is predisposed to postoperative complications with a variable occurrence of morbidity and mortality. Anastomotic leaks, bleeding, marginal ulcers, obstruction, fistula, and biliary issues as common bile duct stones are some of them.5,6
Cholelithiasis is a prevalent disease; about 22% of Argentinean population would suffer from it. 7 In addition, its incidence can reach 40% after a significant weight loss, increasing the risk of choledocholithiasis. This is a serious complication of gallstones and represents nearly 15% of the cases. 8
Common bile duct stones in a patient who underwent weight loss surgery, specially Roux-en-Y gastric bypass (RYGB), one anastomosis gastric bypass, or duodenal switch, is a challenging scenario due to the difficult access to biliary ducts because it is already altered anatomy. 9
Methods
Biliary stones and RYGB
Obesity is a complex chronic disease, which represents a severe and growing health issue all over the world. RYGB is one of the most common bariatric procedures universally performed. RYGB is still considered as the gold standard technique for obesity treatment. It is a “combined” technique because it includes restrictive and disabsortive components. The technique is completed by creating a small stomach called gastric pouch, which will give the food intake restriction. In addition, an alimentary bypass is done by following the Roux-en-Y technical principles to provide a decrease in calorie absorption from the food (Fig. 1).
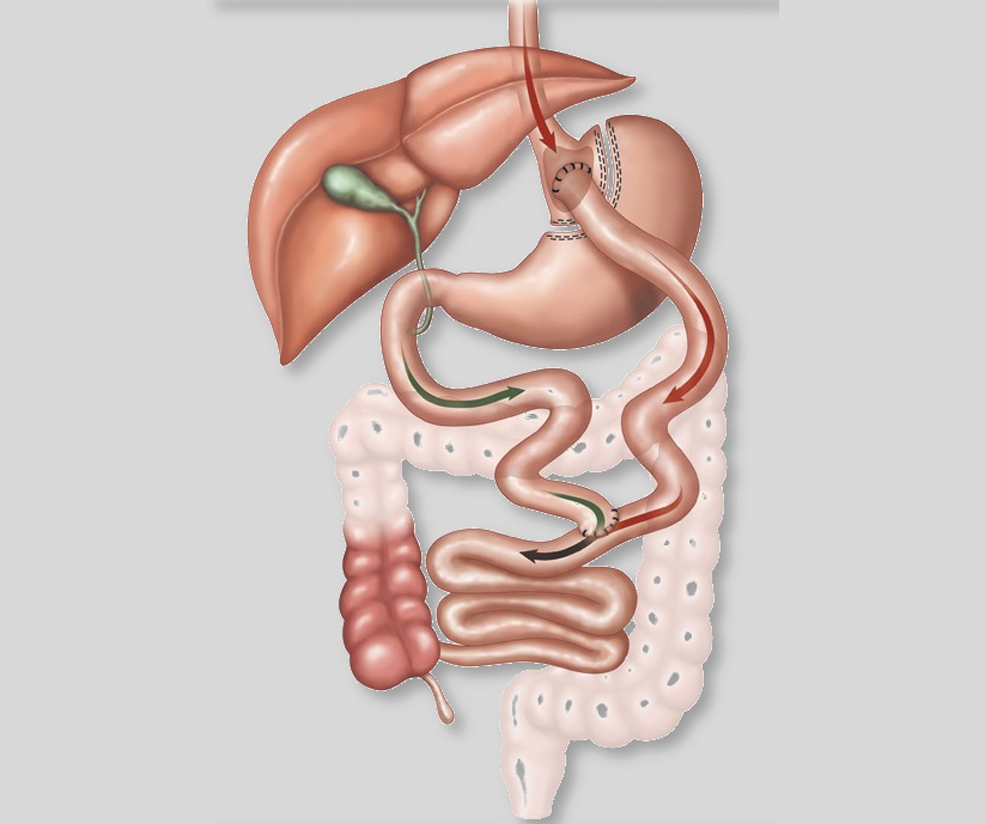
RYGB. RYGB, Roux-en-Y gastric bypass. Illustration by by Manuel García used with permission.
Rapid weight loss associated with certain changes in biliary metabolism and a relative vagal nerve injury from the gastric surgery would be the physiopathological ways to explain an increase in biliary lithiasis after bariatric surgery.10,11 In regard to choledocholithiasis, the incidence after bariatric surgery is not well reported. Lalor et al. 12 estimate around 0.7% in this case series.
The treatment of this biliary complication in patients underwent restrictive surgeries as sleeve gastrectomy or gastric band is the same as for a patient without bariatric surgery. However, in patients who are candidates to bypass surgery, it needs to be hardly evaluated and discussed both in pre- and postoperative period.
Preoperative period
This is a barely debated topic. Some authors recommend laparoscopic cholecystectomy before bariatric surgery just for those patients who have specific symptoms from gallstones; planning two alternatives for those who are asymptomatic: one, concomitant cholecystectomy during bariatric procedure, or two, differed cholecystectomy 4 to 6 months after RYGB. There were no significant differences shown in morbidity nor mortality between these two alternatives.13–15
Choledocholithiasis before gastric bypass
There is no discussion about this situation. Treatment needs to be done as soon as possible. Lap Chole with transcystic common bile duct exploration for stone removal with or without Oddi's sphincter balloon dilation or the endoscopic retrograde cholangiopancreatography (ERCP) with papillotomy, combined or not with “Rendezvous” technique, are the most preferred options; percutaneous approach being a valid alternative when endoscopic approach is not available or in high risk patients.
Choledocholithiasis after gastric bypass
Diagnostic
Diagnosis of bile duct stones or specifically common bile duct stones after RYGB is the same as in nonbariatric patients. However, as it was mentioned before, this complication after RYGB must be suspected even in asymptomatic patients due to the complexity of its treatment.
It is important to consider that bile ducts can be seen as slightly dilated after gastric bypass. 16 In this sense, ultrasonography could be an initial step, but it does not have a high sensitivity for common bile duct evaluation; hence, magnetic resonance cholangiopancreatography (MRCP) would be the choice. 17 Endoscopic ultrasonography could be useful in case MRCP is inconclusive. 18
Results
Treatment
Treatment of common bile duct stones after RYGB represents a challenging situation due to the limitation in the access to bile ducts that these patients have because of the modified anatomy; therefore, this type of patients must be treated in high volume centers in Bariatric and Endoscopic fields to give the patients the best possible results with the lowest morbidity and mortality.
There are many options already described for the treatment of this named situation, but the choice will depend on the experience of the team in charge and the circumstances (emergency or elective condition) in which the patient needs to be treated. Another important information we need to ask for is if the patient still has or not his gallbladder.
We can classify the treatment alternatives into Endoscopic, Surgical, Combined, and Percutaneous.
Endoscopic approach
Focusing in the anatomy of a patient who underwent RYGB, there are about 265 cm (40 cm of esophagus, 5 cm of gastric pouch, 150 cm of Roux limb, and around 70 cm of biliary limb) from the mouth to the second portion of the duodenum where the Oddi's sphincter is located (Fig. 2). Added to that, the vision of the papilla using this way is from the third duodenal portion; thus, the major papilla is seen in an upside-down configuration, which is completely different than a traditional ERCP view. In addition, another important factor is the length of the roux and biliopancreatic limbs; the longer the limbs the higher the failure rate. Hence, endoscopic access of this area requires a tremendous experience in the field of endoscopic treatment, is time consuming, and often necessitates specialized accessories to get it done. 19

Balloon assisted enteroscopy in RYGB. RYGB, Roux-en-Y gastric bypass. Illustration by by Manuel García used with permission.
Per-oral ERCP with duodenoscope
This technique is unused due to the shortness of the scope (120 cm) and its low rate of success.
There are some reported experiences. Hintze et al. 20 showed a failure rate of 67%. Wright et al. 21 applied a modified technique by accessing the papilla with a pediatric colonoscope and placing a guide wire and then advancing the duodenoscope over the wire, guided by fluoroscopy. They completed 45% of the ERCPs.
Push-and-pull and spirus enteroscopy
The enteroscope is a 200 cm endoscope, which allows the visualization of a greater portion of small intestine. Similar to the previously named, Push-and-pull technique (classic enteroscopy), as well as Spirus technique (assisted by a spiral at the tip of the scope to help reach more bowel), is not much used due to their low rate of success.
Single and double balloon assisted enteroscopy
Balloon assisted enteroscopy is one of the most currently used purely endoscopic procedures to perform ERCP in patients who underwent RYGB (Fig. 3). In this technique, the enteroscopy is assisted by one (single-balloon enteroscopy [SBE]) or two (double-balloon enteroscopy [DBE]) balloons. The scope is pulled until its maximal position, and an overtube (which has the balloons) is then advanced to the top of the scope. The balloon is insufflated anchoring the overtube to the intestinal mucosa. It allows a small bowel shortening by pulling back the anchored overtube and pulling forward the scope. This maneuver can be repeated as many times as needed to reach the area of interest.
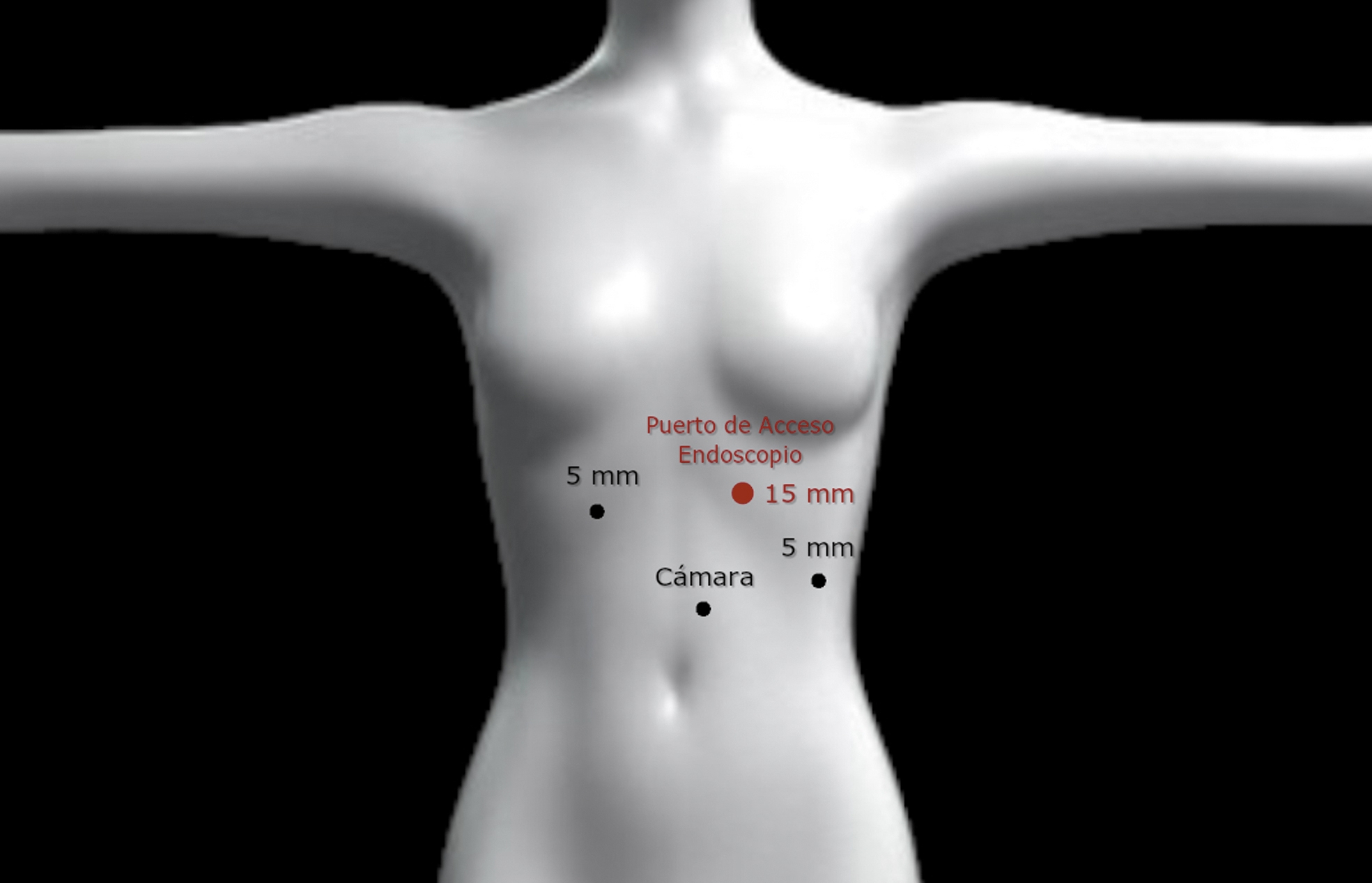
Trocar placement. Note the RED mark on the endoscopic port. Illustration by by Manuel García used with permission.
One of the latest developed SBE is the short type single balloon scope, which is a 152 cm scope with bigger working channels which allows the endoscopist to use the classic ERCP accessories with more stability for the maneuvers.
Success with this technique is reported to be about 60%–70% in the published literature.19,22–24
Endoscopic ultrasound-guided gastrogastrostomy-assisted ERCP
This is a novel technique by which using endoscopic ultrasound (EUS) a gastro-gastric stented fistula is temporarily created between the gastric pouch and the remnant stomach to give access to the classic sided-view duodenoscope to then perform a standard ERCP. After the procedure is done, the stent is removed, and the fistula closed using either single clipping or endoscopic suture such as overstitch. Majidah et al. 24 published significantly better results compared to Balloon assisted enteroscopy. They analyzed a total of 60 patients (30 on each group); the Balloon assisted group (e-ERCP group) included SBE, as well as DBE. The success rate in endoscopic ultrasound-guided gastrogastrostomy-assisted ERCP (EUS-GG-ERCP) group was 100% compared with 60% in the e-ERCP (P < .001). Total procedure time was significantly shorter in EUS-GG-ERCP (49.8 minutes versus 90.7 minutes P < .001). Length of stay also showed to be shorter in the EUS group, and the adverse events were similar, being slightly higher in EUS group.
Surgical approach
Cholecystectomy+transcystic common bile duct exploration (Fig. 4)
In case the patient has no surgical history of cholecystectomy, the gallbladder will need to be removed. Transcystic exploration during the lap chole would be the first option for common bile duct stone removal, typically using a Dormia Basket. This procedure can be associated with a balloon dilation of the Oddi's sphincter, which added a transitory decompressive effect on the bile duct. The sphincter will come back to normal approximately after 4 months from the dilation.
Choledochotomy
This approach is used in cases in which either endoscopic or transcystic ways failed or were not possible to perform. The presence of a common bile duct dilation over 10 mm facilitates a better realization of the technique. Once the stones were removed the duct is closed either in a primary manner or over the T tube based on the size of the bile duct and how the surgeon is used to.
Transduodenal sphincteroplasty and choledochoduodenostomy
These are described as valid options; however, they are not a first line of treatment due to its technical complexity and high risk of complications.
Combined
Transgastric laparoscopic-assisted ERCP
In this operation the remnant stomach is opened to give the scope access to the second portion of the duodenum. It is one of the most performed surgical options due to its low complication rate and feasibility. This allows the realization of an ERCP in a typical manner, which is less technically demanding, using the regular sided-view duodenoscope and the usual accessories.
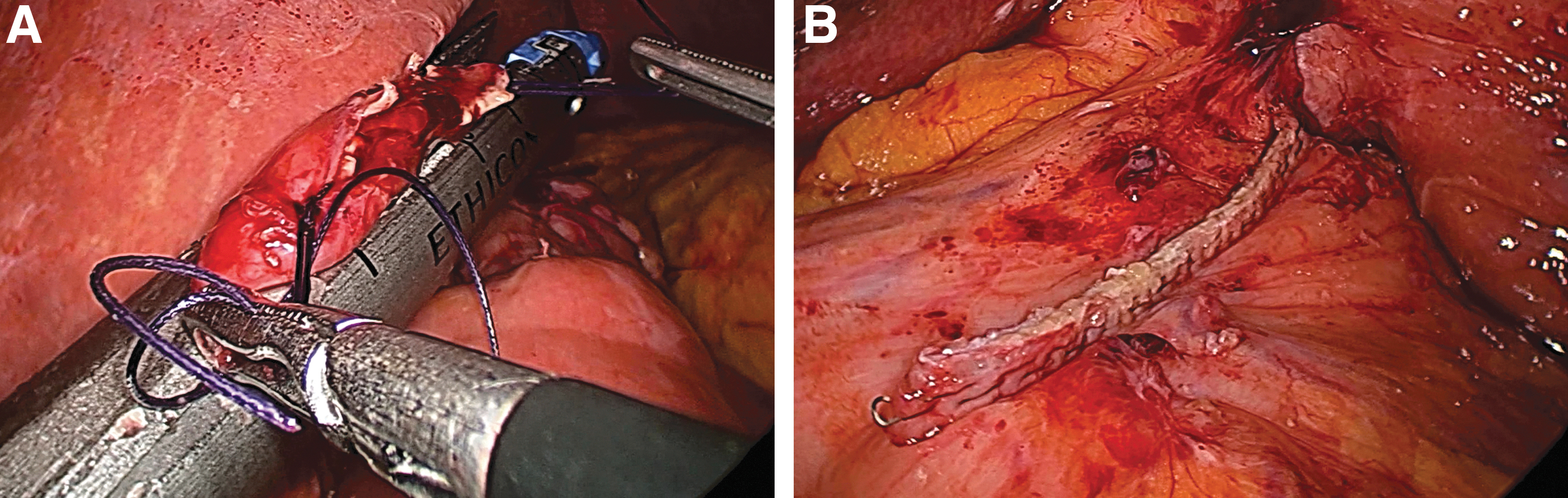
Technical considerations
Using laparoscopic approach, the remnant stomach is localized and the adhesiolysis is performed. It is important to achieve a good stomach mobilization because it allows a better handling of the scope.
Three cardinal anchor stitches are placed on the anterior gastric wall, and a gastrotomy is then made in between. There is no consensus about where the gastrotomy must be made; nevertheless, it is recommended, if possible, to make it toward the gastric corpus since it will give more stability to the scope.
Once the gastrotomy is made, the anchor stitches are exteriorized around the trocar placed at the left upper quadrant (Fig. 5) and the stomach is then pulled up toward the abdominal wall. The trocar is introduced into the stomach through the gastrotomy. An important detail here is that the scope is about 34–36 Fch wide; thus, a 15 mm trocar is needed to be able to pass the scope. In case this trocar size is not available, passing a correctly sterile dressed scope directly through the incision is an accepted alternative (Fig. 6). After the stomach access was accomplished, a classic ERCP with papillotomy is then performed. At the end of the procedure, the gastrotomy is closed either hand sewn or in a stapled manner (Fig. 7). In a prospective study conducted by Falcao et al., 25 they included 23 patients with a mean body mass index of 28.2 kg/m2 after RYGB. All patients underwent an ERCP and papillotomy without incident. Ten patients underwent simultaneous cholecystectomy. They reported an average gastrotomy duration of 92.69 minutes and an average hospital stay of 2 days. A mild acute pancreatitis was the only one complication seen and resolved clinically. No mortality was reported.26,27
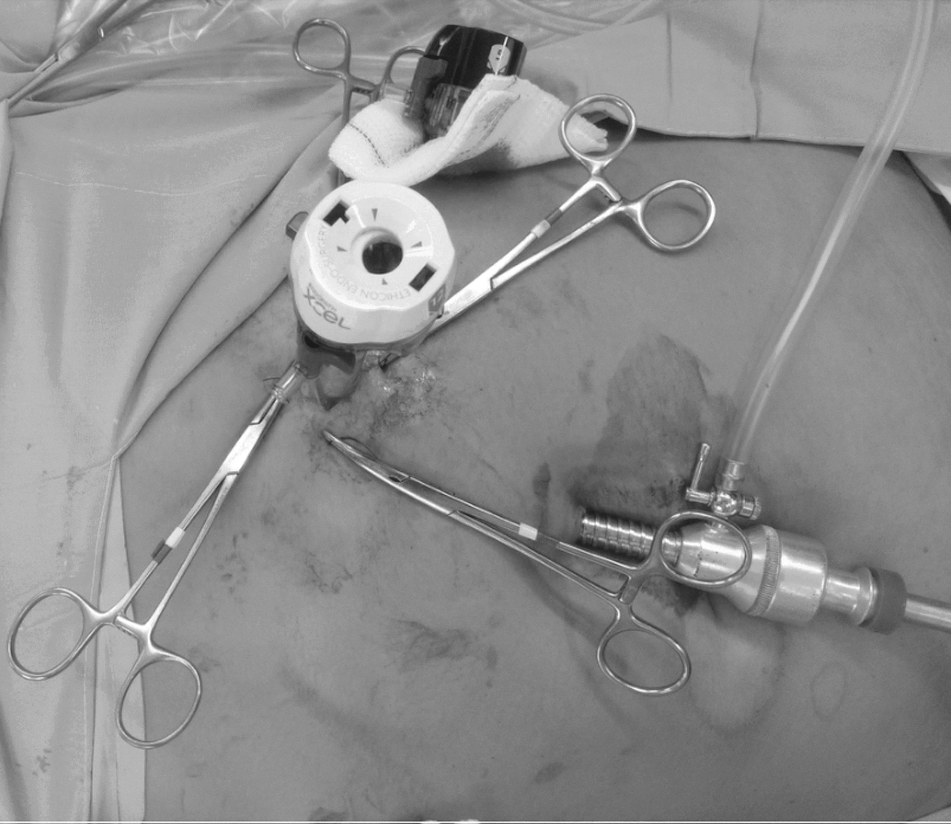
External pulling of the anchor stitches around the scope-access-port to help its entry.

Classic scope dressed by a sterile plastic sleeve.
As we mentioned before the best treatment option will depend on several factors to keep in mind.
Team experience
It is important to remark that this type of patients needs to be treated in high volume centers, specialized in bariatric and endoscopic procedures.
Clinical aspects
The clinical circumstances of diagnostic are much important. If the choledocholithiasis is a casual finding, the treatment timing and the technique will be probably different than if the patient is having a jaundice syndrome or an acute cholangitis and, in this last situation, if the patient is stable or not. For example, in an unstable patient with cholangitis the best treatment will be the one we have at hand to perform as fast as we can to stabilize the patient with the lowest possible risk.
Surgical history
Technical details of the primary surgery are important to know. For example, in patients with roux limb longer than 150 cm and biliopancreatic limb over 100 cm, a laparoscopic-assisted ERCP will be probably the best choice instead of total endoscopic approach due to the already described complexity for the endoscopic access in patients with long bypassed bowel segments.
Need for a second look
In case a second procedure is needed to complete the treatment, a gastrotomy (either surgical in case of laparoscopic-assisted ERCP or percutaneous) could be a good option to leave a rapid access already prepared. 28
Combined surgery
For those patients with a nonemergency situation, laparoscopic approach can be used to combine the treatment of common bile duct stones with another possible condition such as ventral hernias, close of mesenteric spaces, and so on.
Percutaneous approach
This approach has acquired an important role in the recent years. It showed to be less technologically demanding with good results and low complication rate.29–31
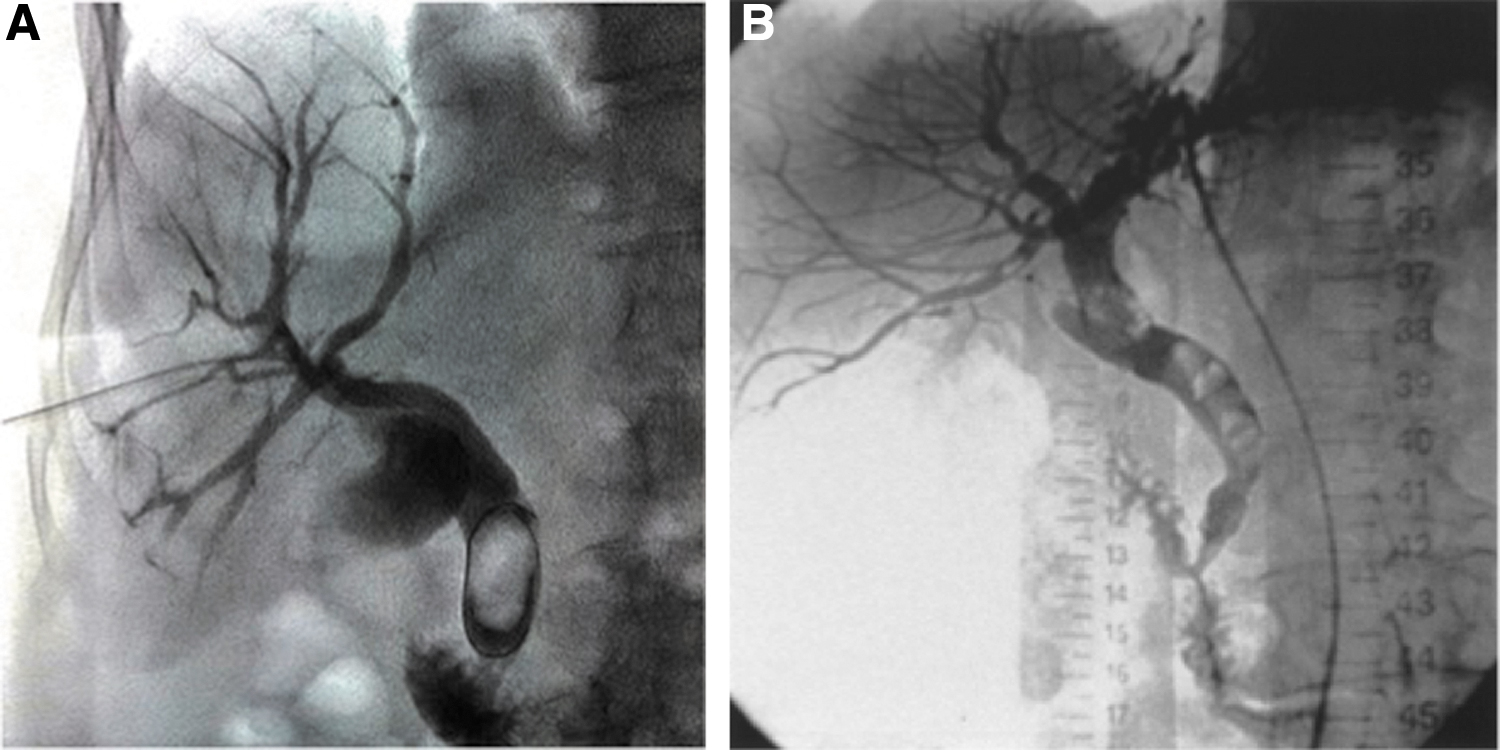
Technical considerations
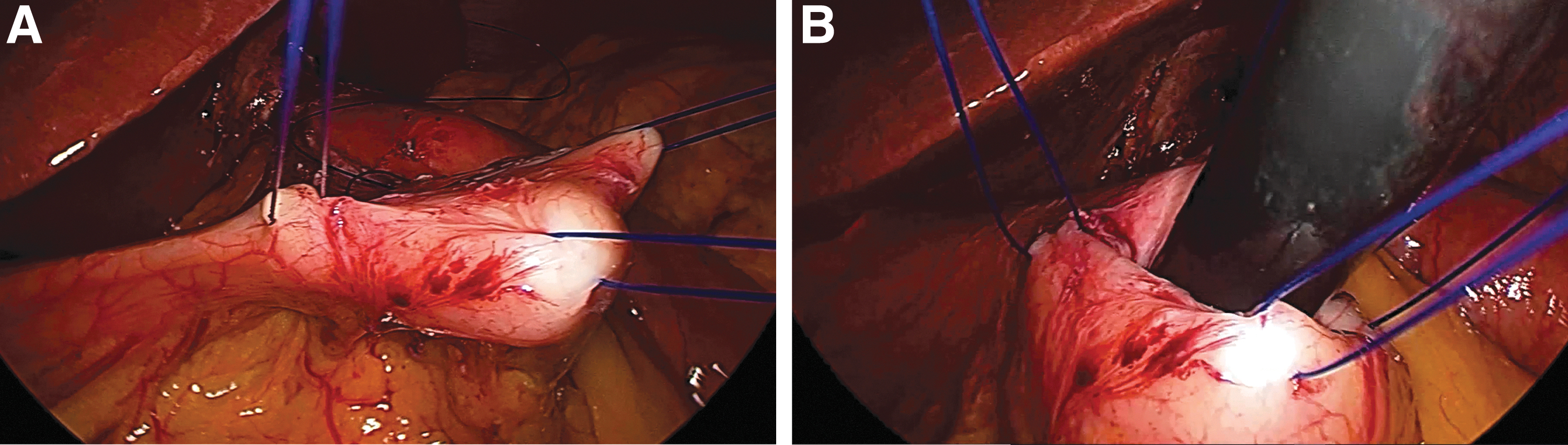
First step is to perform a percutaneous transhepatic biliary access. According to the localization of the stones on the preoperative workup, the access could be done by either right (Fig. 8A) or left (Fig. 8B) hepatic branches. Once the access is completed, a cholangiography is performed to confirm the presence of the stones.31–33 Then, an internal-external catheter is placed through the papilla (Fig. 9) to help bile tree decompressing. Overdilation of the Oddi's sphincter using a high-pressure balloon (Fig. 10) will be performed up to 20 mm Hg to help the stones to pass from the common bile duct to the duodenum. This last step would probably need a successive session as many as possible since we need to get a full clear biliary tree.31–34

Placement of internal–external transhepatic biliary drainage.

Overdilation of the papilla using high-pressure balloon.
Percutaneous approach of choledocholithiasis after RYGB is a safe and effective treatment. It is less invasive than surgical approach and it represents a simpler way than the endoscopic approach in this type of patients.26,27,34
Conclusion
Obesity is growing day by day worldwide and with it the number of bariatric surgeries. It means that this kind of complications will need to be treated sometimes by a general surgeon. Therefore, its approach in terms of diagnostic and treatment must be widespread over the general surgeon community. It has a tremendous importance mainly for those patients who are facing a life treating situation.
Rapid weight loss, as is seen after bariatric surgery, increases the incidence of cholelithiasis, thus choledocholithiasis.
Common bile duct stones in patients who underwent RYGB represent very widely debated topic in the latest years, due to its technical challenging situation because of the altered anatomy that the primary surgery implies.
There are several therapeutic options; many of them have already demonstrated excellent results. Even though there is not a gold standard technique, the total endoscopic approach performed by trained hands should be the first line of treatment. Percutaneous approach represents also a safe and effective option that can avoid reoperations in an important number of patients. However, the choice will depend on the severity of the case to face with, the availability of resources, and the experience of the team.
Whichever be the case, it is of crucial importance, if possible, that these patients be admitted in a high volume center that has the adequate resources to treat them, as well as be evaluated, treated, and followed up by a trained team in bariatric, endoscopic, and/or percutaneous fields. This way the patient will get the best possible results with the lowest possible risk.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.