
Abstract
Introduction:
Thoracic surgery in children with coronavirus disease-19 (COVID-19) pulmonary disease is rare, as very limited virus-related lung lesions require intervention. However, some patients may suffer from other pulmonary abnormalities that can be worsened by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and they may consequently require lung surgery. COVID-19 affects the indications, surgical procedure, and postsurgical care of these patients.
Background:
We present a case of a 14-year-old girl with COVID-19 pulmonary disease and persistent air leak due to right apical bullae that required resection. Clinical, surgical, and safety implications are discussed. The role of thoracic minimally invasive surgery under COVID-19 conditions is also analyzed.
Materials and Methods:
The thoracoscopic procedure was scheduled earlier than normally expected. The surgery was performed in a COVID-19 reserved theatre with neutral pressure and only the necessary personnel was allowed inside. The use of the required personal protective equipment was supervised by an expert nurse before and after the intervention.
Results:
The surgeons used a three-port technique to resect the bullae with an endostapler and no mechanical pleural abrasion was added to the procedure. Electrocautery and CO2 insufflation were avoided, and a chest drain with a closed-circuit aspiration system was installed before removing the ports. The child was discharged home 3 days later after the removal of the chest drain.
Conclusions:
COVID-19 has an impact on the standard indications, surgical strategies and postoperative care of some conditions requiring intervention. Extra safety measures are needed in the operating room to limit the chance of transmission. Minimally invasive surgery for thoracic surgery remains safe if the current safety guidelines are followed closely.
Introduction
Since the outbreak of the coronavirus disease (COVID-19) in December 2019, caused by the new severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the incidence among children aged <18 years has been estimated between 1% and 5%1,2 and the clinical course in this range of population seems to be less severe than in adults.1–10 Although less frequent, when SARS-CoV-2 does occur in children, common respiratory symptoms include dry cough and shortness of breath, and radiologic findings on CT scan normally show diffuse ground glass opacity, with or without consolidation areas, with more localized extent, lower attenuation, and less lobular involvement than in adults. 4 Alveolar pleural fistula with pneumothorax is not a typical feature and is described anecdotally only in some adult cases 11 with severe pulmonary lesions, and should, therefore, raise concern about the possibility of other diseases. 12
The first confirmed case of COVID-19 in Spain was reported on January 31, 2020. Since then, 200,210 cases have been reported with 20,852 deaths up until April 20, 2020. In the data reporting information about age and gender (80,172 cases), the pediatric population (<19 years) accounts for 0.86% of the cases with no mortalities recorded, up until April 14, 2020. The first pediatric case in our hospital appeared on February 25, 2020 and, subsequently, only 20 pediatric cases tested positive for SARS-CoV-19 up until April 20, with only one requiring thoracic surgery.
We report here the first pediatric COVID-19 thoracic surgical case to be performed on a patient with respiratory disease in our hospital. The case represented a challenge on the indications and timing for surgery, safety implications in the operating room, and recommendations for the way in which minimally invasive surgery (MIS) should be performed.
Background
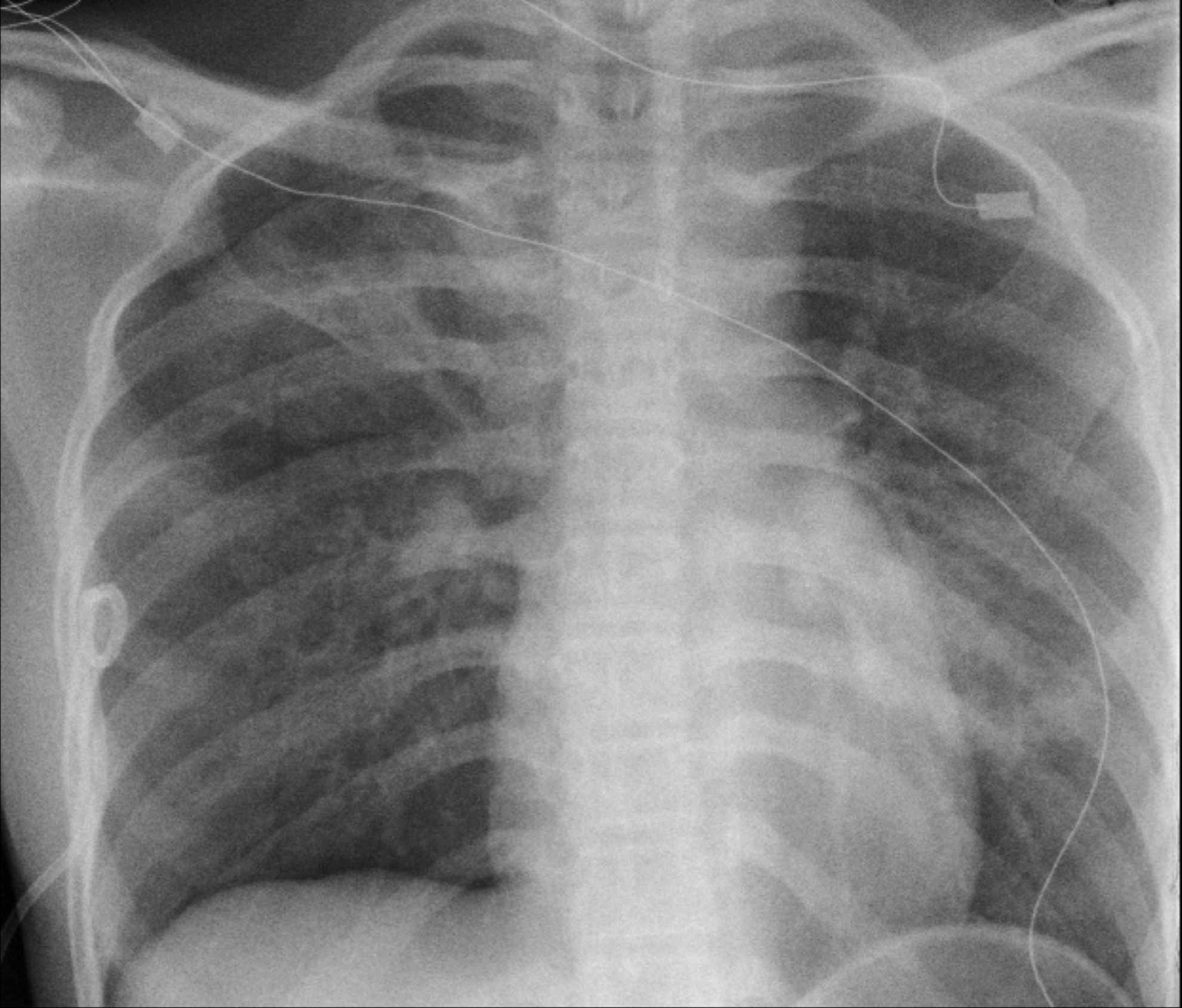
A 14-year-old girl with a clinical course of cough and thoracic pain for 11 days before admission, fever for 5 days prior, and anosmia and ageusia for 3 days prior was admitted to our hospital with a right pneumothorax and left infiltrations in the plain X-ray study (Fig. 1). The girl, of Asian origin, has been living in Barcelona since she was little and attends school in an international center with students from >40 nationalities. Two weeks before the onset of symptoms, her school had had a week's holiday, during which many pupils traveled to their home countries, including China and Italy. The patient was previously healthy but reported a history of multiple allergies and asthma during infancy. She needed punctual inhaled bronchodilator therapy during episodes but, in the previous 2 years, these episodes had been rare and she had not required regular medication or admissions to hospital. Two days before the state of emergency was declared in Spain on March 13, she manifested, during a sports activity at school, the onset of symptoms with shortness of breath and mild thoracic pain, which subsided shortly after. The following week, however, she developed a high fever, dry cough, and dyspnea, anosmia, and ageusia until, in the end, she sought medical advice.

Plain X-ray at admission with right pneumothorax (cross) and left consolidation image (arrow).
Suspicion of COVID-19 was established and she tested positive on the SARS-CoV-2 polymerase chain reaction in the nasopharyngeal sample. The patient was admitted into the intensive care unit where a chest tube was placed in accordance with safety guidelines for transmission. This improved the pneumothorax and the respiratory symptoms (Fig. 2). She was then moved to the ward the next day but persisted with a high flow air leak through the drain, on inhaling but also and, most markedly, on exhaling, meeting the criteria for a type 4,C classification of persistent air leak (PAL) according to Cerfolio. 13 Standard conservative management was initially attempted but the air leak did not improve and a CT scan was scheduled. It showed 2 bullae (24 and 17 mm in diameter) arising from the apical part of the right upper lobe along with diffuse ground-glass infiltrations in all lobes, but the right medium one, with several consolidation areas in those lobes (Fig. 3).
Plain X-ray after chest drainage. Persistent right apical pneumothorax.

Preoperative CT scan.
According to the excellent clinical status of the patient, who remained without fever or O2-support therapy despite the lesions observed in the CT scan, and the continuous nonimproving air leak, we decided to proceed with surgery on the fourth day after her admission. We brought the surgery forward before establishing the diagnosis of PAL (5–7 days of PAL)14,15 to reduce as much as possible the patient's stay in hospital and, therefore, her contact with medical personnel.
Materials and Methods
The intervention was performed in a COVID-19 reserved theater with neutral pressure (negative pressure was unavailable in our center). Professionals inside the room were limited to the 2 anesthesiologists, 2 pediatric surgeons, and 2 surgical nurses. Before the 6 professionals entered the operating theater, they got dressed in the required personal protective equipment (PPE), 16 under the supervision of an expert surgical nurse. Once all the staff were inside, the patient was admitted to the theater and no one left the room until she was dismissed to the intensive care unit after the procedure. Once again, a surgical nurse supervised while the staff removed their PPE before leaving the theater.
In an attempt to avoid insufflations of CO2 into the thorax, the anesthesiologists proceeded to a right pulmonary exclusion intubation and the patient was placed in a left lateral decubitus. A three-port thoracoscopy was performed. Incisions were limited to the size of trocars (two 5 mm and one 12 mm) and valved ballooned devices were use to avoid the leak of air through them. No CO2 was introduced into the chest and no electrocoagulation was needed during the surgery. A unique large bulla was found (Fig. 4) and resected using an endostapler. A manual reinforce suture of the parenchyma was added to the procedure. The rest of the pulmonary tissue looked perfectly normal without any other pleural lesions. Accordingly, and bearing in mind the need to shorten the procedure and the lack of knowledge about the response of the parenchyma in a COVID-19 scenario, and also acknowledging the potential coagulation abnormalities this disease may cause, we decided not to perform the mechanical abrasion pleurodesis. Before closing up the incisions, a chest drain was placed into the thorax and connected to a closed circuit aspiration system, to avoid the potential spread of the virus into the theater.
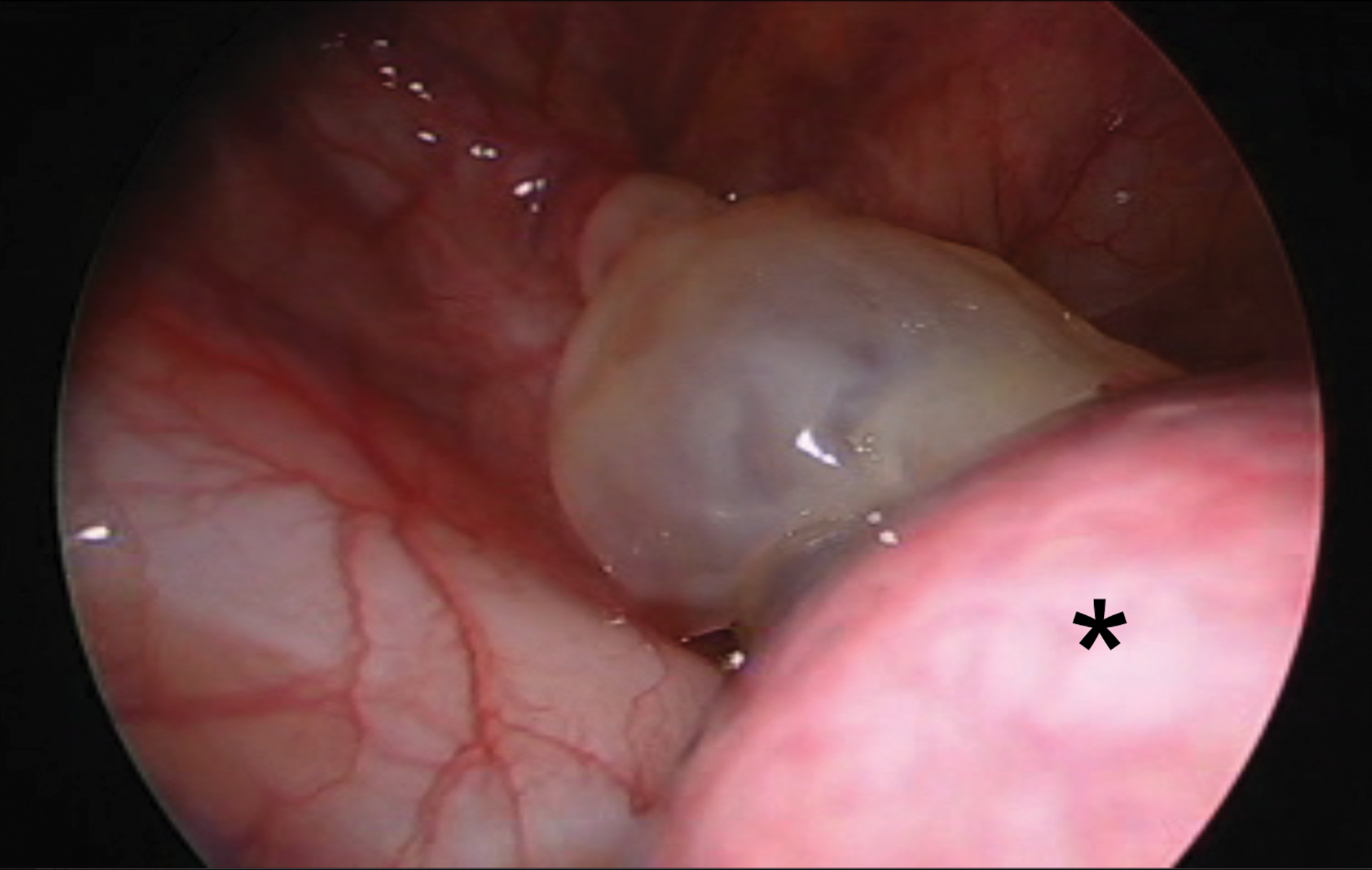
Surgical image of the bulla (*right upper lobe).
Results
The outcome was uneventful and the drain was removed 2 days later with complete resolution of the pneumothorax and the air leak. The patient was discharged home on day 3 after surgery and remains free of symptoms 1 month after. All professionals involved in the procedure also remain free of COVID-19 symptoms.
Discussion
The need for lung surgery with COVID-19 is exceptional and, as far as children are concerned, we did not find any reference in the updated literature. Pulmonary problems due to SARS-CoV-2 do not normally cause conditions requiring intervention. Pleural effusions and pneumothorax are very seldom observed and pulmonary resections are generally not indicated for virus-related lesions. 12 Likewise, bullae formation is not a typical feature of COVID-19 and has been inadequately represented in the literature and, even then, it has been only in adults with very severe radiological findings. 11 Whether or not the bulla and consequent pneumothorax in this patient is related to the virus, we cannot tell, but most likely it is not. The onset of thoracic pain and difficulties in breathing, together with the typical location of the bullae, suggest a pre-existing lesion that was aggravated by COVID-19.
COVID-19 infection introduced changes to the standard management of this PAL. The good respiratory condition of the adolescent made her a candidate for managing the infection from home, which would have been preferable to limit contact with hospital staff, but PAL forced her to remain in the hospital. Therefore, we did not opt, as we normally would, for conservative management14,15 and proceeded with the surgery to shorten the patient's stay in hospital. Another variation of the standard care was not to add a mechanical pleural abrasion to the procedure.14,15 Although the parenchyma seemed normal during surgery, we knew about the inflammatory process she had in the CT scan and we preferred not to risk more damage and bleeding, given that COVID-19 is a disease that seems to affect the inflammatory cascade and coagulation. Shortening the surgery was also important to limit the exposure of the team to the virus.
Safety in COVID-19–related procedures is mandatory. A fully dedicated room for these patients, if possible with negative pressure, and training in getting properly dressed and undressed in the PPE are key points to avoid contamination. Other factors such as limiting the staff to the minimum needed and respecting established times for entering and leaving the room also seem to have an impact in avoiding the transmission of the virus.
The use of MIS in a COVID-19 scenario is a matter of debate due to the eventual possibility of contamination of the air in the theater by the CO2 and coagulation smoke.17,18 For this reason and in the absence of strong evidence, it may be important to follow the guidelines for this option as reported by scientific societies such as the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) 19 or European Society of Paediatric Endoscopic Surgeons (ESPES). 20 In our case, the relevant pointers followed were a theater dedicated to COVID-19, reusable instrumentation, zero use of CO2, zero use of electrocautery, closed system for air aspiration, and valved and ballooned ports to avoid leaks. Besides, in the authors' opinion, MIS in thoracic surgery has a big impact on recovery, shortening the hospital stay compared with thoracotomy. This fact increases in relevance in a COVID-19 environment.
Conclusion
To summarize, COVID-19 does not normally cause lung lesions necessitating thoracic surgical resection, but some patients may have pre-existing abnormalities that force us to draw up a surgical plan. Standard care may be affected by COVID-19, forcing us to change strategies in the indication, surgical procedure, and postoperative management. Extra safety measures are needed in the operating room to limit the chance of transmission. MIS is a good option for thoracic surgery, if the recommendations already made are followed closely, at least until there is further evidence for stronger safety procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.