
Abstract
Introduction:
Laparoscopy has been used for the evaluation of impalpable testes for more than 30 years. However, its use for intra-abdominal testes has never been evaluated in a population-based approach. Neither has the share of timely orchiopexies of intra-abdominal testes according to published guidelines. We aimed to provide this information by using nationwide administrative data for hospital reimbursements.
Materials and Methods:
We obtained data for procedures for exploration and orchiopexy of intra-abdominal testes in Germany from 2005 through 2018 and analyzed them with linear regression for the use of laparoscopy and timely repair.
Results:
In 2005, laparoscopy was already used in more than 60% of explorations, which composed 76% (95% confidence interval [CI]: 72 to 79) of children operated before their first birthday and 68% (95% CI: 65 to 70) of children up to 4 years of age. Throughout the study period, laparoscopy became increasingly popular for orchiopexy of intra-abdominal testes with a yearly increase of 1.8% (95% CI: 1.2 to 2.5, P < .001) in the first year of life and 1.3% (95% CI: 0.2 to 3.4, P < .001) until the age of 4. The share of patients treated before their first birthday increased yearly by 1.9% for explorations and 1.6% for orchiopexies (P < .001 for both) but did not exceed 30% in 2018.
Conclusion:
Laparoscopy is the method of choice for exploration of intra-abdominal testes and orchiopexy. In this study, more than 70% of boys were treated after their first birthday, thus not meeting the time limit set by guidelines.
Introduction
Laparoscopy has been used for the evaluation of impalpable testes for more than 30 years, particularly because its accuracy exceeds those of imaging techniques. 1 In 1984, shortly after Semm's first laparoscopic therapeutic operation, 2 Ransley et al. described the first laparoscopic gonadal vessel ligation. 3 This cleared the way for a truly laparoscopic first-stage Fowler–Stephens orchiopexy in 1991. 1 Later, one-stage laparoscopic orchiopexy became the procedure of choice. 4 There are still controversies about the right management of impalpable testes. 5 Consequently, the epidemiology of orchiopexy has been widely investigated using population-based databases such as those from New York State 6 or Sweden. 7 While some have advocated that laparoscopy offers the possibility to simultaneously initiate treatment of intra-abdominal testes, 8 others preferred an open inguinal approach due to the a priori low risk of intra-abdominal testes. 9 In this study, we aimed to assess the use of laparoscopy for diagnosis and treatment of impalpable testes in a German nationwide hospital statistic to shed insight into recent changes in management. Inspired by reports of suboptimal compliance with guidelines for orchiopexy, in Germany 10 and in the United States, 11 we also investigated how many procedures had been conducted before the first birthday, according to guidelines that were changed in 2009. 12
Materials and Methods
Description of the data
We acquired data with encoded operations used to calculate hospital reimbursements for all nonpsychiatric hospitals in Germany from the Statistisches Bundesamt (Federal Statistics Office) for the years 2005–2018. We analyzed operations for impalpable testes, coded as “exploration for cryptorchidism” (OPS 5-625) and “orchiopexy of an intraabdominal testis” (OPS 5-626). These data do by definition not include any cases of retention testis inguinalis, which would not be included in the relevant German definition of cryptorchidism, 13 because an inguinal position of an impalpable testis needs to be excluded before proceeding to laparoscopy. 14 Consequently, an inguinal position of an impalpable testis would have been coded by a different code (OPS 5-624). Studies conducted on anonymized administrative data are exempt from ethical approval because they can never be traced back to the individual patient. 15
The German system of pediatric surgery
Contrary to many other countries, Germany has a decentralized system of pediatric surgery 16 : More than 500 board-certified pediatric surgeons 17 provide pediatric surgical care in 129 pediatric surgical units in 2017, equaling 46 pediatric surgeons per million children younger than 14 years. 16 There is a clear distinction between pediatric surgery and surgery in children: The former is exclusively part of the pediatric surgical specialty, whereas the latter comprises basic surgical operations conducted in children. 18 This clear distinction is enforced via the hospital recompensation system that denies payment by health insurances if a procedure is not part of the training curriculum of the surgeon, 19 which is not the case for exploration for cryptorchidism for both urologists and general surgeons.
Statistical analysis
Data were analyzed for differences over time using linear regression.20–22 Statistical analysis was conducted using R (version 3.5.3) with its generic stats4 package (version 3.4.3). 23 Normality of errors was checked via the Shapiro–Wilk test and homoscedasticity with the Breusch–Pagan test from the olsrr package (version 0.5.3). 24 Age groups were compared with White-adjusted analysis of variance—due to missing homoscedasticity—implemented in the car package (version 3.0-7) 25 with post hoc tests conducted via the Games–Howell test implemented in the PMCMRplus package (version 1.4.4). 26 Using these tests is recommended for missing homoscedasticity, but normally distributed errors and corrects are recommended for multiple testing. 27 For comparisons that did not meet the assumption of normally distributed errors, we used van der Waerden's test 28 followed post hoc by the Conover–Iman test as recommended by Luepsen. 29 In these cases, corrections for multiple testing were conducted according to Benjamini and Hochberg. 30 Bias-corrected accelerated bootstrap with 10,000 repetitions, as described before,31,32 was used to construct 95% confidence intervals (CIs) of point estimates via the Hmisc package (version 4.4-0). 33 Differences of mean percent of procedures conducted in the first year of life before and after the introduction of the new guideline in 2009 were evaluated the same way with an hypothesis test for nonequivalence using the wBoot package (version 1.0.3.). 34
Results
There were
The percentage of laparoscopic evaluation for impalpable testes increased by 0.8% (95% CI: 0.2 to 1.3, P = .016) yearly in the age group between 1 and 4 years (Fig. 1A). The percentage of children in the age group between 5 and 9 years increased by 1.9% (95% CI: 0.8 to 3.1, P = .004) (Fig. 1A). This was not the case in the first year of life (Δ = 0.6%, 95% CI: −0.3 to 1.5, P = .101) and in children aged 10 years and older (Δ = 1.5%, 95% CI: −0.6 to 3.6, P = .139) (Fig. 1A). The frequency of an inguinal approach in children aged 5–9 years decreased by 1.7% per year (95% CI: −2.8 to −0.6, P = .007) but remained unchanged for the other age groups (<1 year: −0.3% [95% CI: −1 to 0.4, P = .352]; 1–4 years: −0.4% [95% CI: −0.9 to 0.1, P = .102]; 10–14 years: −1.4% [95% CI: −3.1 to 0.4, P = .124]) (Fig. 1B). Open abdominal exploration was rare without change over time.
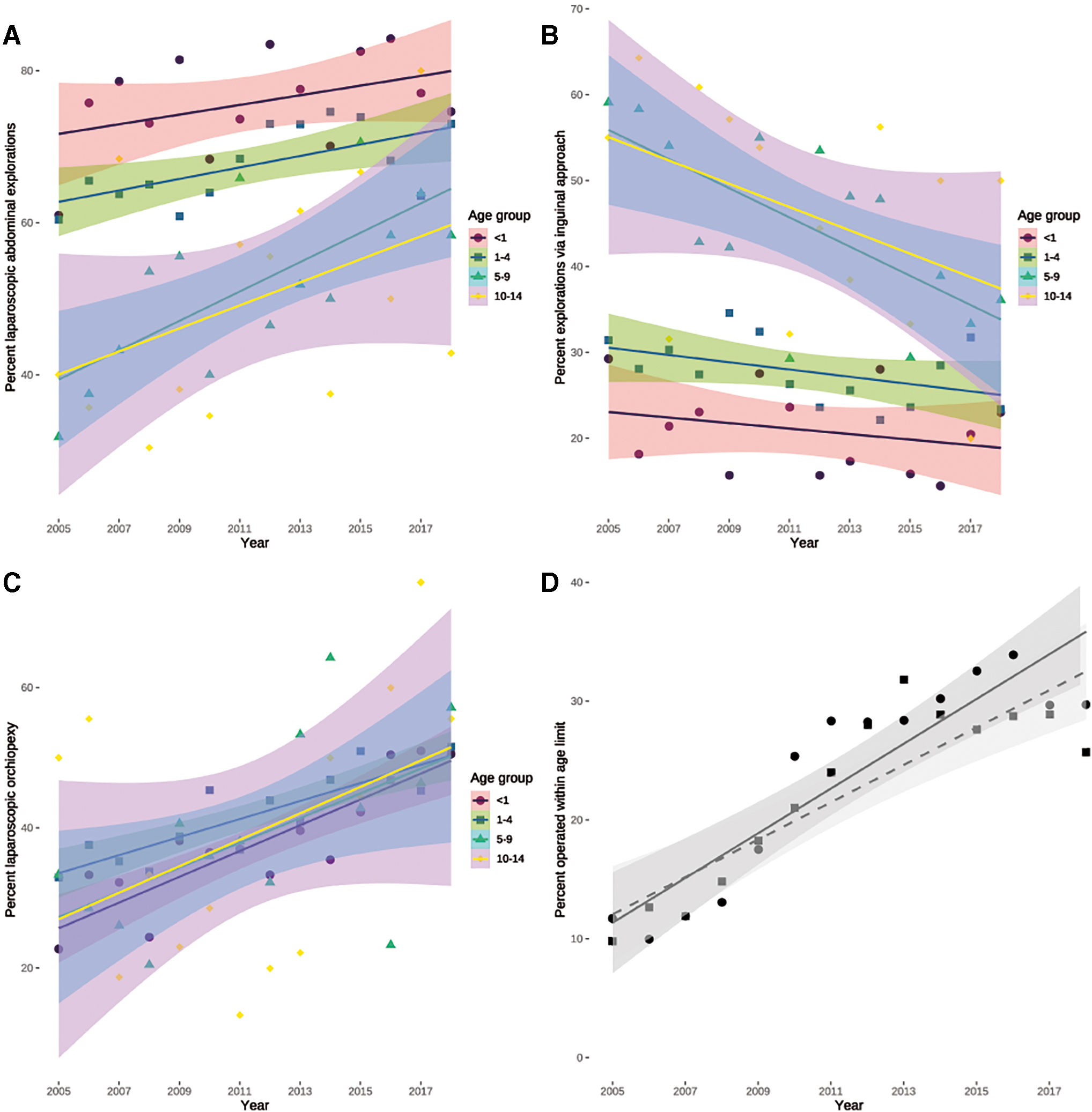
Changes in procedures over time evaluated by linear regression.
Relevant age differences were present among children explored via inguinal [F(1,3) = 28.283, P < .001] and laparoscopic [F(1,3) = 21.306, P < .001] but not via an open abdominal approach [F(1,3) = 1.331, P = .274] (Table 1). In contrast, this was not the case for patients who had a laparoscopic or open orchiopexy for impalpable testes: There was no difference between the age groups for laparoscopic [F(1,3) = 0.768, P = .517] and open abdominal orchiopexy [F(1,3) = 0.663, P = .578] (Table 2).
Distribution of Exploration Approaches Among the Age Groups
CIs were obtained via bias-corrected, accelerated bootstrap with 10,000 repetitions. The groups were compared via an analysis of variance with White-adjustment followed post hoc by the Games–Howell test.
CI, confidence interval.
Distribution of Orchiopexy Approaches Among the Age Groups
CIs were obtained via bias-corrected, accelerated bootstrap with 10,000 repetitions. The groups were compared via an analysis of variance with White-adjustment.
CI, confidence interval.
We observed an increasing use of laparoscopy for orchiopexy in the first year of life with 1.8% (95% CI: 1.2 to 2.5, P < .001) per year, in children up to the age of 4 years with 1.3% (95% CI: 0.8 to 1.7, P < .001) per year, and in children up to 9 years of age with 1.8% (95% CI: 0.2 to 3.4, P = .0343) per year, but it did not change in children who were older (Δ = 1.9%, 95% CI: −0.7 to 4.5, P = .139) (Fig. 1C).
Guidelines specify orchiopexy to be conducted before the first birthday since 2009. We therefore evaluated whether guideline adherence improved over time and found a yearly increase of 1.9% (95% CI: 1.3 to 2.4, P < .001) in explorations for impalpable testes and 1.6% (95% CI: 1 to 2.1, P < .001) for orchiopexies (Fig. 1D). Comparison of explorations before and after guideline publication revealed that the percentage of children who had an exploration for impalpable testes was 16.8% (95% CI: 13.4 to 19, P = .001) higher after the guideline was available (
Discussion
There is much debate about the right surgical approach to impalpable testes. While some prefer an inguinal approach for unilateral impalpable testes reserving laparoscopy for bilateral cases, 9 others advocate an inguinal approach as a first stage and only use laparoscopy if an inguinal exploration is negative. 35 We found an unexpectedly high use of laparoscopy for the diagnosis of impalpable testes in more than 60% of all cases as far back as 2005, even in children in their first year of life. In them, we have not seen a further increase in the use of laparoscopy for evaluation of impalpable testes. Since 2005, the use of laparoscopy has increased for diagnostic purposes, which is actively endorsed by contemporary guidelines. 36 The small group of patients treated via an open abdominal approach most likely consists of children deemed unfit for pneumoperitoneum due to cardiopulmonary disease. This interpretation is supported by their stable numbers throughout the investigative period. On the contrary, orchiopexy of intra-abdominal testes was primarily open surgery at the beginning of the study period, because more than 60% of patients were managed in this approach in 2005. The distribution between the approaches has been reversed since then, with laparoscopic orchiopexy being the preferred treatment in 2018, as demonstrated by our data. The figures in 2005 did not match the numbers provided in a survey among pediatric surgeons from 2007, 37 but since only 70% of all pediatric surgical institutions took part in that particular survey, a relevant nonresponder bias is likely. Moreover, laparoscopy has been restricted to only one surgeon in several departments in this survey, 37 which may also contribute toward the comparatively lower percentages observed in our study. The inguinal approach was much more frequent in older children, likely due to secondary testicular ascents being treated in this age group.
Fortunately, we observed an increasing number of boys treated for impalpable testis in their first year of life. This development already started in 2005, although the guideline specifying a threshold age of 1 year had not been changed until 2009. 12 However, in 2005, Rokitansky already advocated for a treatment by the first year of life, 38 a recommendation that caught on with others only 2 years later. 39 In addition, this development has also been observed in regional cohorts before.6,40 However, the vast majority of cases with undescended testes are operated after the cutoff of 1 year of age, irrespective of the investigated country 12 : This affects Germany,10,12,40 Austria, 41 Australia, 42 China, 43 Singapore, 44 Taiwan, 45 and the United States11,46 and thus represents a global problem. Despite the increase in timely operated patients in our study, more than 70% were not treated within their first year of life, which is similar to results from all over the world.
Much has been written about possibilities to improve this situation. One study reported an association between adherence to guidelines and the use of laparoscopy. 47 Timely orchiopexy has also been associated with younger surgeon age, 45 possibly indicating more recent training at a time when the guidelines had already been published. This idea is supported by a negative association of primary care provider age and the rate of timely intervention, 45 as well as referral from a nontertiary institution. 44 Interestingly, even in a country with decentralized pediatric surgical care—such as Germany 16 —the presence of a pediatric surgical service in a nearby hospital was associated with a higher proportion of timely orchiopexies. 10 This indicates that pediatric surgeons may play a role in knowledge dissemination in a community.
The most striking advantages of using routine administrative data are their number of cases due to their compulsory nature and resulting coverage of the whole population. 48 This results in sufficient numbers of rare events, which are crucial to identify smaller effects that are likely to be missed in cohort studies due to their naturally smaller sample size. 22 On the contrary, administrative data are hampered by their missing detail, which does not allow to take patient-specific factors into account when analyzing the data, such as gestational age in prematurely born children. 22 Moreover, our data are not based on patients, but on procedures, so the same patient may be included twice in the data set, if he had bilateral disease. Another aspect that requires the data to be interpreted with caution is the missing link between procedure and outcome-related measures, such as recurrences or complications. Nevertheless, administrative data may be able to shed light on aspects that would otherwise have been missed and thereby prompt further research that would not have been started. It allows a relatively simple testing of hypotheses compared with directly starting with the expensive and time-consuming data collection on multiple study sites. 49 In addition, the results from administrative data may guide sample size calculation because it provides an estimate of the effect size and may thus help to better allocate scarce research money.
In conclusion, over the past two decades, laparoscopy has become the method of choice for exploration of intra-abdominal testes and orchiopexy even in a country with decentralized pediatric surgical care. Nevertheless, a majority of boys are still not operated by their first birthday, even though some improvement in the timely repair rates has been achieved.
Footnotes
Disclosure Statement
The authors have nothing to disclose.
Funding Information
The present study was conducted without funding.