
Abstract
Umbilical hernias and acute appendicitis are common general surgical problems, but an appendix incarcerated in an umbilical hernia is quite rare. We present a case of such and briefly review the available literature on the topic. We conclude that future authors should include a minimum set of information in such case reports or case series so that readers can gain as much as possible from our collective experience with this uncommon problem.
To the Editor,
S
Case Report
A 60-year-old male veteran construction worker with a body mass index (BMI) of 26 kg/m2 presented to the general surgery clinic with new onset of an umbilical bulge. Seven days before presentation, while lifting a box of cement, he felt and heard a “pop” and since then had an irreducible, mildly tender bulge at his umbilicus. He denied obstructive or constitutional symptoms. He denied any medical or surgical history. Social history revealed a remote 20 pack-year smoking history.
On physical examination the patient was afebrile with normal vital signs and in no distress. Abdominal examination revealed an irreducible umbilical hernia surrounded by nonblanching erythema up to 5 cm away from the bulge circumferentially. The patient was mildly tender at the hernia but without signs of diffuse peritonitis. No laboratory or imaging studies were obtained. Given these signs of potentially strangulated viscera we advised that the patient undergo an urgent operation that day. He declined but agreed to return as first case the next morning. In the operating room a curvilinear supraumbilical incision was made, exposing a 1 cm fascial defect, and the hernia sac was deliberately opened to reveal the contents pictured: the appendix and mesoappendix, with venous congestion of the distal 3 cm of both structures (Fig. 1) The fascial defect was widened to 2 cm and the cecum and terminal ileum were easily brought into the incision without the need for lateral dissection. An appendectomy was performed with silk suture ligation and electrocautery ablation of the exposed mucosa. The hernia defect was closed primarily with permanent suture using interrupted vertical mattress stitches; we elected not to use mesh despite the 2 cm defect for fear of a mesh infection.
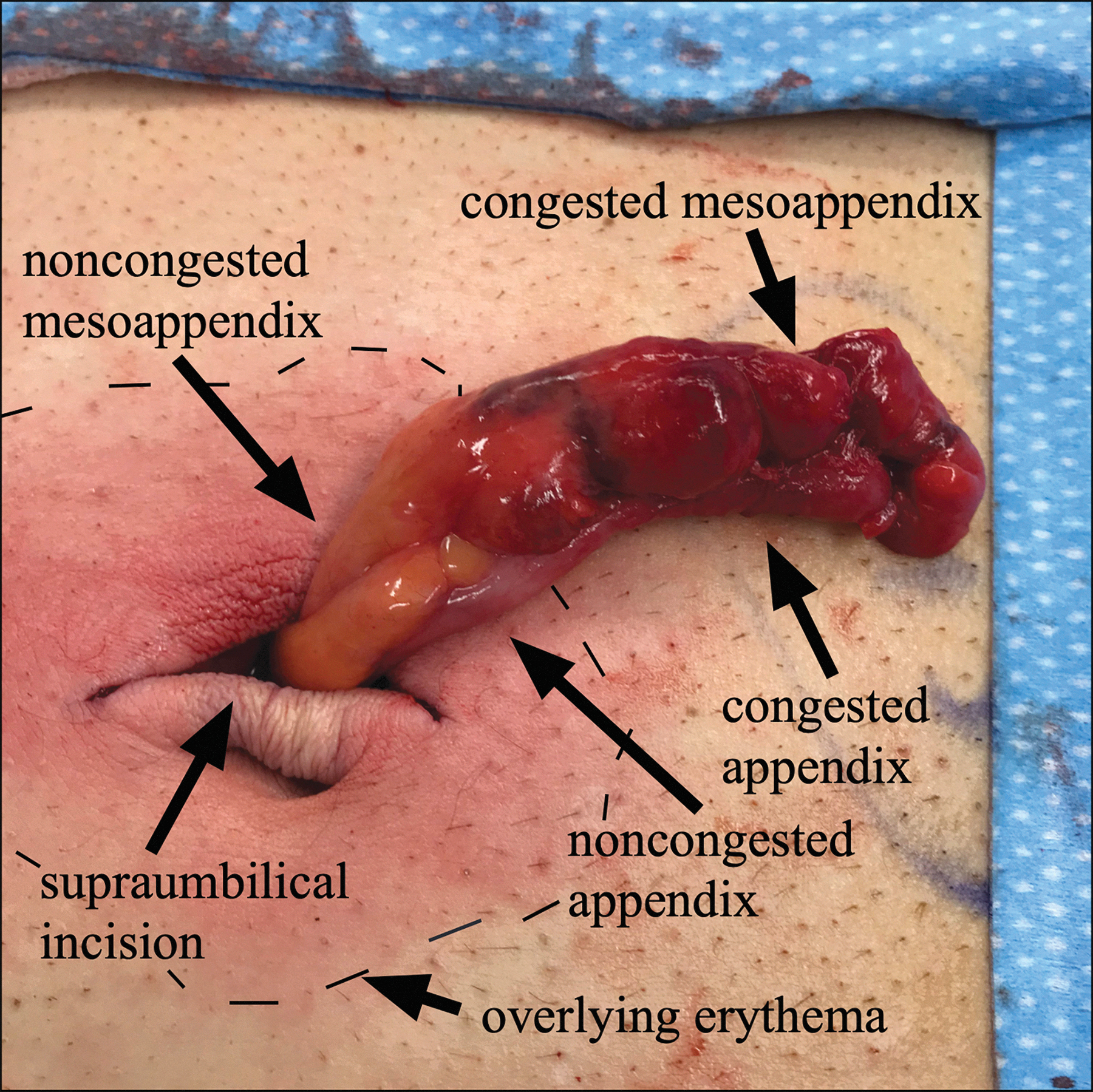
Intraoperative photograph.
The patient was discharged from the postanesthetic care unit without complications and was seen in clinic 3 weeks later without signs of infection or immediate hernia recurrence. Pathology revealed a 6 cm long and 6 mm wide appendix without pathological signs of acute appendicitis, only venous congestion of an otherwise normal vermiform appendix and mesoappendix.
Discussion
We report the case of an otherwise normal appendix strangulated within a newly discovered umbilical hernia. Searching PubMed for MESH terms “umbilical hernia” and any of “appendix,” “vermiform appendix,” or “appendix, vermiform,” and Google Scholar® (Google, Inc., Mountain View, CA) for the same, we found seven English-language case reports of umbilical hernias in adults since 1970.
As others have observed,2,4 we see two main questions about umbilical hernias containing appendixes: whether these patients' appendixes are naturally located in an umbilical hernia and they developed acute appendicitis in the same manner as other patients do, or if these are simply cases of strangulated viscera in a hernia that happen to involve the appendix due to its variable anatomic location. We suspect the latter in the majority of reported cases, and this was certainly the case here; however, three1,5,6 of the seven case reports describe their patients as having acute appendicitis rather than an appendix strangulated in an umbilical hernia sac. This question is largely academic, as most surgeons would likely agree that appendectomy should be performed in these circumstances regardless of the underlying cause of the appendix's presence in the hernia. The second question is whether or not these patients are at high-enough risk of wound infection that mesh should be avoided. Single case reports cannot answer this question; however, three1,5,7 of the seven case reports did not specify this information, and in four2–4,6 mesh was reportedly not used, as in our case.
Taking guidance from large studies of umbilical hernia repairs, 8 in future case reports on this topic we would recommend that authors include at a minimum the patient's age, gender, BMI, presenting symptoms, vital signs, whether or not the defect was previously known, whether or not the hernia was reducible, laboratory studies if they were obtained, whether the operating surgeon felt this was a case of acute appendicitis within an umbilical hernia sac or a case of an appendix strangulated within an umbilical hernia, whether or not an appendectomy was performed, whether or not mesh was used during herniorrhaphy and what type of mesh, whether or not the skin was closed, pathology findings, the patient's postoperative length of stay, and any major postoperative complications that occurred. Including this information may help surgeons seeking to learn from our limited collective experience in addressing this uncommon scenario.