
Abstract
Introduction:
Xanthogranulomatous cholecystitis (XGC) is a rare inflammatory disease of the gallbladder (GB). XGC surgery is a difficult process due to its clinical, radiological, and intraoperative findings. In this study, our aim is to show the difficulties of XGC surgery and to find out if laparoscopic surgery is a sufficient procedure.
Materials and Methods:
Histological findings of 3339 cholecystectomy patients, who were operated between January 2015 and January 2020, were retrospectively reviewed. Age, gender, radiological results, clinical features, intraoperative findings, and surgical management of the patients with XGC were recorded.
Results:
XGC was observed in 70 patients (2.09%). The average age was 53.75. M:F ratio was 1.2. In radiological examinations, gallstones were found in 94.2% of the patients and GB wall thickness (≥3 mm) was increased in 58.5% of the patients. Around 45.7% of the patients came to the clinic with chronic cholecystitis and 32.9% with acute cholecystitis. In the intraoperative period, adhesions were observed in 80% and increase in GB wall thickness was observed in 77.1% of the patients. The operation started laparoscopically in 66 patients. In 14 patients (21.2%), it was converted to open surgery usually due to insufficient dissection of Calot's triangle. Gallbladder carcinoma (GBC) was suspected in 6 patients, but none of them had malignancy in frozen sections or histology.
Conclusions:
XGC surgery is difficult due to its radiological, clinical, and intraoperative features and mimicking GBC. It can be converted to open cholecystectomy due to difficulties in laparoscopic dissection. However, since conversion cholecystectomy rates are reasonable, laparoscopic surgery is recommended in patients with suspected XGC.
Introduction
Xanthogranulomatosis refers to the condition caused by the accumulation of lipid-laden histiocytes in different parts of the body. Xanthogranulomatous inflammation occurs in various organs such as skin, kidney, retroperitoneum, intracranium, gastrointestinal system, and genital organs. 1 Xanthogranulomatous cholecystitis (XGC) is a rare chronic inflammatory disease characterized by macrophage and foamy cell infiltration and diffuse fibrosis in the gallbladder (GB) wall. 2 Inflammatory reaction and fibrosis cause asymmetric wall thickening in the GB wall and multiple yellowish brown-colored intramural nodules.3,4
It is clinically seen as acute or chronic cholecystitis. Diagnosis is generally difficult in the preoperative and intraoperative period. Surgery is often difficult due to intense fibrosis and adhesions to neighboring organs. Therefore, laparoscopic cholecystectomy (LC), which is the gold standard in the treatment of GB disease, results in a high rate of failure.5,6
The aim of our study is to show the difficulties of XGC surgery and to find out if laparoscopic surgery is sufficient.
Materials and Methods
In this study, the histological findings of 3339 patients who underwent cholecystectomy between January 2015 and January 2019 at Istanbul Health Sciences University Şişli Hamidiye Etfal Training and Research Hospital General Surgery Clinic were reviewed retrospectively. The diagnosis of XGC was made histologically in 70 patients and its details were analyzed.
Demographic information, radiological findings, diseases related to gallstones in the preoperative period, and intraoperative findings were collected.
Age and gender were recorded in demographic information.
In radiological findings, gallstones, GB wall thickness (those with wall thickness ≥3 mm were evaluated as increased wall thickness), and pericholecystic fluid in the upper abdomen in ultrasonography (USG) or magnetic resonance imaging (MRI) before surgery were recorded.
In the preoperative period, choledocholithiasis, hyperbilirubinemia, endoscopic retrograde cholangiopancreatography (ERCP) history, and acute biliary pancreatitis history were recorded.
In the intraoperative period, the size of the GB, GB wall thickness, edema, adhesions, abscess, fistula, Mirizzi's syndrome, suspicion of malignancy, duration of surgery, and type of surgery (LC, open cholecystectomy [OC], and conversion cholecystectomy [CC]) were recorded.
Statistical Package for the Social Sciences (SPSS, version 22) was used to analyze the data. The data were defined using percentages and averages.
Results
Seventy of 3339 patients were diagnosed as XGC histologically. Thus, XGC constitutes 2.09% of cholecystectomies in our study. The ratio of the male patients is 54.28%. The patients in our study are between 19 and 82 years old and the average age is 53.75 ± 15.2 (Table 1).
Demographic Information, Radiological Findings and Clinical Presentation, of 70 Patients with Xanthogranulomatous Cholecystitis
ERCP, endoscopic retrograde cholangiopancreatography; GB, gallbladder; SD, standard deviation.
Gallstones were detected in 66 patients (94.2%) in USG or MRI. In 41 patients (58.5%), GB wall thickness was increased (≥3 mm). Only 4 patients had pericholecystic fluid (5.7%). Two patients were operated with the diagnosis of porcelain GB. Intramural hypoechoic nodules were not described in preoperative imaging studies in any of the 70 XGC cases (Table 1).
Chronic cholecystitis was the most common clinical presentation (45.7%) at the admission to hospital in our study. Acute presentation during admission was seen at the remainder. This was in the form of acute cholecystitis, obstructive jaundice, and acute biliary pancreatitis. Acute cholecystitis was the second most common clinical presentation. Approximately 32.9% of the patients came to the clinic with acute cholecystitis. Obstructive jaundice was diagnosed in 9 patients (12.9%) as the third most common presentation. Six patients (8.5%) had acute biliary pancreatitis. Fourteen of 15 patients with obstructive jaundice and acute pancreatitis preoperatively performed ERCP (Table 1).
In the intraoperative period, 80% of patients had adhesions in the GB. Omental adhesions (61.4%) were the most common; duodenal adhesions and colonic were observed in 14.2% and 10% of the patients, respectively. In 77.1% of the patients, the thickness of the GB wall increased. Edema was seen in the GB wall in 22.8% of the patients. GB hydrops were observed in 14.2% of the patients and fibrosis in 11.4% of patients. There were liver abscesses in 3 patients, Mirizzi's syndrome in 1 patient, and cholecystoduodenal fistula in 1 patient. In 6 patients, gallbladder carcinoma (GBC) was suspected, but no cancer cells were seen in intraoperative frozen sections and histology (Table 2).
Intraoperative Findings of 70 Patients with Xanthogranulomatous Cholecystitis
GB, gallbladder.
OC was performed in 4 patients. Two patients had liver abscess and 1 patient had a diagnosis of porcelain GB preoperatively. One patient underwent OC due to a history of coronary bypass. The operation was started laparoscopically in 66 patients. However, it was converted to OC in 14 patients (20%). The rate of conversion to OC was 21.2%. In 10 patients, the operation was converted to OC due to insufficient Calot's triangle dissection. In 4 patients, the operation was converted to OC as a result of insufficient exploration due to intra-abdominal adhesions caused by previous operations. The operation of 52 patients (74.3%) resulted laparoscopically. While the average operation time was 123.28 minutes, it was 122.01 minutes in LCs and 126.78 minutes in CCs (Tables 2 and 3).
Operative Approach and Operation Times of 70 Patients with Xanthogranulomatous Cholecystitis
CC, conversion cholecystectomy; LC, laparoscopic cholecystectomy; OC, open cholecystectomy.
Discussion
XGC was first described in the literature by Christensen and Ishak in 1970. 7 Surgery is difficult for this rare inflammatory and it is hard to distinguish it from GBC. 8 The incidence of XGC is reported as 0.7–13.2 of all cholecystectomies in the literature.1,9 In the meta-analysis, which included 29 studies by Hale et al., the incidence of XGC was 1.3%–1.9%, excluding India, whereas it was found 8.8% in India. 10 In our study, it was found 2.09%.
XGC is mostly seen in men1–3,6,8,9,11–16 and in the sixth decade.4,10,13,14 In some studies, it was found more frequently in women.17–19 There are studies in which the female-male ratio is equal. 4 In the meta-analysis published by Hale et al., the mean age was found as 53.7. 10 Our results were similar to the literature. In our study, the mean age was 53.7 and it was seen more in men.
Although XGC is well-defined histologically, it is difficult to diagnose it radiologically. Although gallstones and thickened and echogenic GB walls are frequent radiological findings, they are not specific.18,20 Gallstones are defined in 72%–100% in different studies.2,4,5,8,9,14,18,19 The GB wall thickness increase varies between 59% and 100% in different studies.3,5,6,8,19 Hypoechoic nodules and hypoechoic bands in the thickened wall are occasionally seen and considered characteristic findings. 20 Hypoechoic nodules were found 15% in the study by Parra et al., 16.7% in the study by Qasaimeh et al., and 73% in the study by Kim et al.5,17,18 In the study performed by Parra et al., the rate of hypoechoic band was 19%. 18 Pericholecystic fluid was found 28.6% in the study by Qasaimeh et al. and in 29% in the study Deng et al.3,5 In our study, gallstones were found in 94.2% of the patients, GB wall thickness was increased in 58.5%, and only 5.7% of patients had pericholecystic fluid in USG or MRI. Intramural hypoechoic nodules were not described in preoperative imaging studies in any of the 70 XGC cases. Increase in GB wall thickness was lower than other studies and existence of gallstones results was similar with the literature in our study.
Any signs or symptoms for XGC are not specific. The signs and symptoms are similar to acute and chronic cholecystitis. Patients with XGC often present with an acute complication of cholelithiasis, such as obstructive jaundice, acute biliary pancreatitis, or empyema of the GB. It can also be seen as the right upper quadrant mass mimicking GBC.5,8 Clinical presentations during the admission to the hospital are acute conditions in some studies.5,18,19 However, there are studies in the literature that show chronic conditions are higher.6,8,9 In Qasaimeh et al's publication, patients who underwent cholecystectomy for XGC were compared with patients who underwent cholecystectomy for benign GB disease. 5 While acute cholecystitis and obstructive jaundice were significantly higher in the XGC group, there was no difference in acute pancreatitis. In the same study, acute conditions were higher (59.5%). The most common clinical presentation is biliary colic (40.5%), the second is acute cholecystitis (26.2%), the third is obstructive jaundice (21.4%), and the forth is acute pancreatitis (4.8%). In two other studies that acute conditions were high, acute cholecystitis rate was found to be close to the half of XGC patients (Parra et al. 54%, Srinivas et al. 48%).18,19 In our study, clinical presentation during the admission is frequently acute conditions (54.3%). Chronic cholecystitis was the first with a rate of 45.7%. Acute cholecystitis was the second with 32.8%. Obstructive jaundice was observed in 12.8% and acute pancreatitis in 8.5% of the patients.
XGC is confused with GBC in the clinical, radiological, and intraoperative period. Irregularities in the GB wall, adhesions and fistula to neighboring organs, which are noticed by the surgeon during the intraoperative period, both make surgery difficult and create suspicion for malignancy, and in these cases, intraoperative frozen section is recommended (Fig. 1).8,10,21,22 XGC is more frequently associated with GBC than other forms of cholecystitis. Co-occurrence rate of XGC and GBC varies between 2% and 15%. For this reason, the rate of performing inappropriate surgery in the form of open surgery or bed resection with a false prediagnosis of GBC during LC is 3%. Due to the adhesions caused by local inflammation and GB wall thickness, the conversion rates from laparoscopic surgery to open surgery are high (Fig. 2). 10 In the study published by Deng et al., while all patients were found to have increased thickness in the GB wall during the intraoperative period, adhesions were seen in 95.2% of the patients. The most common adhesion was found omental and the anatomy of the Calot's triangle was found to be uncertain in 26% of patients. 3 In another study, 82% of patients had increased GB wall thickness, omental adhesions were observed in 79% of patients. 19 In the meta-analysis published by Hale et al., co-occurrence rate of XGC and GBC has been reported between 0% and 20%. Intraoperative GBC was suspected in 10.1% of all XGC patients, but in 1.3%, GBC was diagnosed. 10 In the study published by Yucel et al., 33.3% of patients who were operated laparoscopically had a frozen section due to suspicion of malignancy and only 2 patients had malignancy. 9 In our study, 77.1% of patients showed increased GB wall thickness. Adhesions were observed in 80% and the anatomy of Calot's triangle was found to be uncertain in 14.2%. In 6 patients (8.5%), GBC was suspected in the intraoperative period, frozen sections were studied in 4 patients. None of the frozen sections and histological results showed malignancy. Our results were similar to the literature.
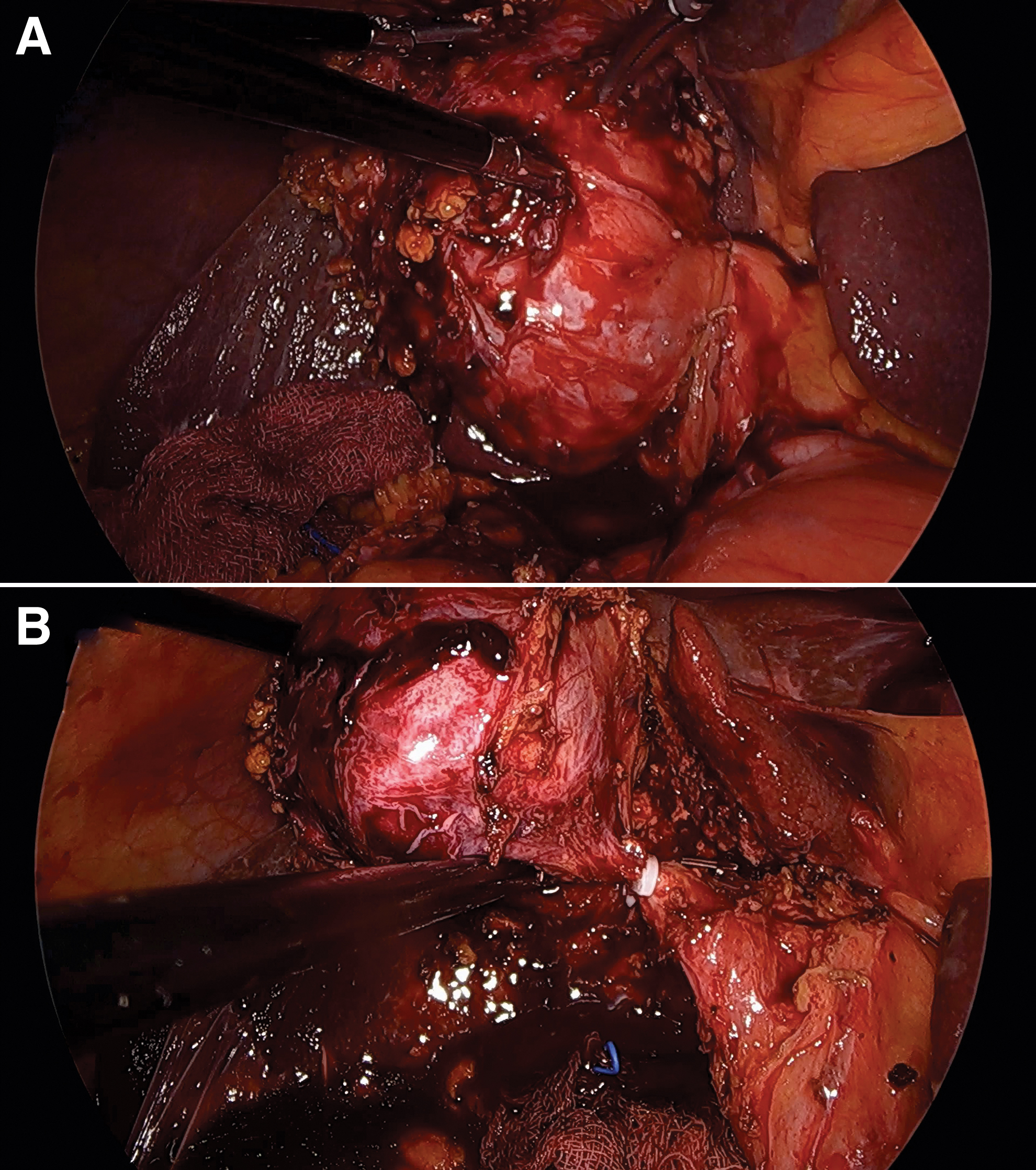
Cholecystectomy that is started laparoscopically and completed laparoscopically.
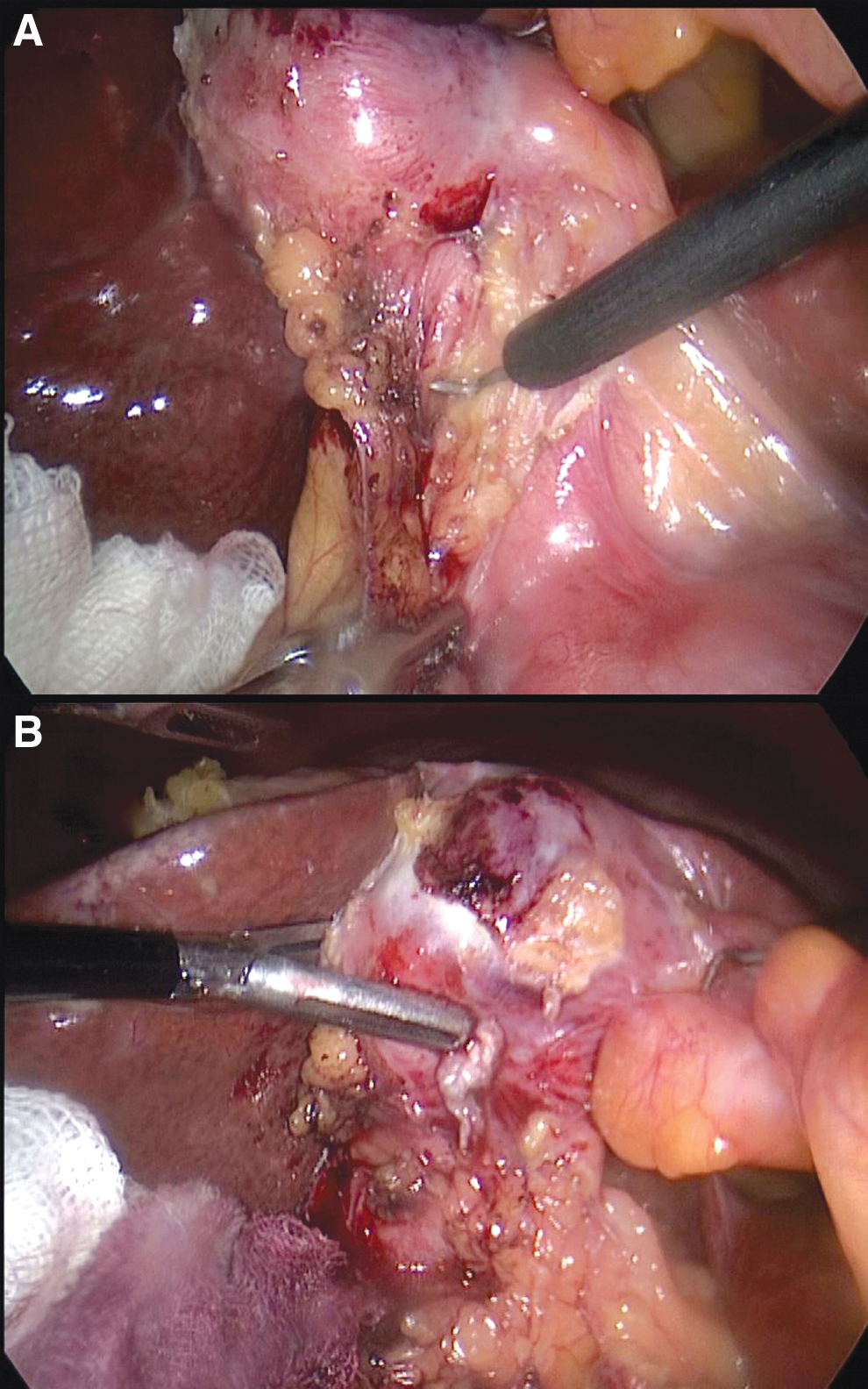
Cholecystectomy that is started laparoscopically and converted to OC.
LC is the gold standard in GB surgery. The conversion rate from laparoscopic surgery to OC for any reason in the literature is 1.1%. 23 Since it is difficult to diagnose XGC patients in the preoperative period, the operation starts laparoscopically if the patient does not have a hindrance to laparoscopic surgery.4,5,8,13,19 However, in some publications, an open approach has been adopted because of the suspicion of cancer or high expectation of conversion to open surgery.1,3,6,14,15 Also, the rate of conversion from laparoscopic surgery to open surgery has been reported to be 10%–80%.2,4,5,6,8,9,13,16,18 In the literature, the lowest CC rate was seen in Wang et al. with 10.6%, whereas the most CC rate was seen in Guzman-Valdivia with 80%. In our study, the rate of conversion to open surgery is 20%.
Conclusions
XGC surgery is difficult due to high clinical presentation of acute conditions, increased thickness in the GB wall radiologically, increased GB wall and adhesions in the intraoperative period, and confusion with GBC. For this reason, it may be necessary to switch to open surgery in laparoscopic surgeries due to the insufficient dissection of Calot's triangle or probability of malignancy occurrence in frozen sections. However, cholecystectomies were completed laparoscopically in most of the patients in our study. Therefore, in patients with suspected XGC, it is recommended to start the surgery laparoscopically, although XGC surgery is difficult and to study frozen sections in case of suspected malignancy.
Footnotes
Authors' Contributions
M.B. designed the study and offered final approval on the version for publication. Y.G. and Ö.B. conducted data analysis and wrote the article. R.İ.T. contributed to data acquisition and analysis. All authors read and approved the final article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.