
Abstract
Background:
Peripheral arterial disease has high incidence and complication rates. Vessel recanalization represents the main therapy. However, it induces reperfusion injury. Preconditioning with sildenafil has been advocated to protect against this injury. In this study, we show a real-time noninvasive quantitative assessment using hyperspectral imaging (HSI) of ischemia/reperfusion (IR) and analyzing the sildenafil effect.
Materials and Methods:
A one-sided hindlimb ischemia (120 minutes) followed by reperfusion (30 minutes) was created. Five mice received Sildenafil (1 mg/kg, i.p. twice before ischemia) and 5 mice served as control. The StO2 at T0, 5, 30, 60, 120 minutes after ischemia (T5, 30, 60, 120) and 5, 15, and 30 minutes after reperfusion (T125, 135, 150) were measured through HSI.
Results:
The control group showed a significantly lower StO2 at T120 (24.8% ± 17%) as compared with T0 (53.3% ± 7.04%) (P = .013) and T150 (76.8 ± 3.77; P = .0008). T150 showed a statistically significantly higher StO2 than T0 (P = .0134). In the sildenafil group, T120 StO2 (28.6% ± 20%) was lower than T0 (63.3% ± 8.46%; P = .0312) and T150 (73.3% ± 19.1%, P = .0075). The StO2 values did not differ statistically between sildenafil and control groups.
Conclusions:
HSI is a feasible tool to quantify both ischemia and reperfusion phases during lower limb IR. Preconditioning with sildenafil did not modify IR-related StO2 changes.
Introduction
Lower limb ischemia–reperfusion (IR) cycles characterize peripheral arterial disease (PAD), which is accountable for severe complications. Those include limb loss. PAD is often associated with cognitive dysfunction and death.1,2 Overall PAD prevalence ranges from 3% to 10%, and it increases to 15%–20% in the older population (>70 years of age). 3 Surgical or angiographic revascularization interventions possibly associated with thrombolysis represent the main therapeutic option. Revascularization of a large vessel, which might be unfeasible in some instances, is not always followed by complete reperfusion at microcirculation or cellular levels. 2 Additionally, vessel recanalization triggers a massive reactive oxygen species (ROS) production, causing ischemia–reperfusion injury (IRI). Several strategies have been investigated to limit IRI damage, and one of those is the pharmacological preconditioning using a cyclic nucleotide phosphodiesterase (PDE) inhibitor. In particular, the PDE5 inhibitor, sildenafil, has shown promising protective effects against IRI on several organs,4–6 although it has recently failed to show any improvement in terms of mitochondrial respiration of the skeletal muscle. 7 However, it tended to reduce ROS production, which might be linked to a change in the degree of reperfusion. Accordingly, despite recent advances in the knowledge of PAD pathophysiology,8,9 the development of more effective therapeutic approaches still represents a strategic target of basic and clinical research.
Currently, the hindlimb ischemia (HLI) murine model is widely used in preclinical studies and the efficacy of the tested experimental therapies is usually assessed combining intravital (laser Doppler perfusion imaging [LDPI] or magnetic resonance imaging [MRI] angiography) with postmortem techniques (histology, microcomputed tomography [micro-CT]). 10 Those methods are expensive, time consuming, and provide meaningful information if they are merely used in combination, since none of them alone can simultaneously provide noninvasiveness, quantification, and adequate spatial resolution. In this view, there is the need for a noninvasive real-time diagnostic tool, which can provide a precise quantitative perfusion analysis. Hyperspectral imaging (HSI) acquires spatial images along the electromagnetic spectrum, consequently providing a tridimensional dataset called hypercube (x, y as spatial coordinates, and λ as the spectral coordinate). This technology couples a spectrometer to a photo camera, and the tissue–light interactions at the analyzed area mirror its specific biochemical features. HSI has been largely exploited in the industrial and agricultural field, and since approximately two decades it has been progressively used in medicine. 11 Given its ability to quantitatively discriminate the chemical composition of the analyzed surface in a contactless and nondestructive fashion, it is rather attractive for the medical field. Recently, HSI found multiple medical applications, 11 for cancer detection, 11 for monitoring the efficacy of laser thermoablations,12,13 or for the intraoperative detection of target structures, which need to be selectively preserved intraoperatively, such as the common bile duct 14 or parathyroid glands. 15 In particular, given its capability in quantifying the amount of oxygenated tissue hemoglobin within the tissue microcirculation, it has been successfully used to detect endothelial dysfunction in healthy individuals, 16 to successively screen patients for PAD17,18 and to detect 19 or quantify20,21 intestinal ischemia. Recently, considering its ability to discriminate ischemic tissue, HSI has been used as a surgical navigation tool to achieve experimental HSI-guided anatomical hepatic resection. 22
The aim of this study was to explore the capabilities of HSI to quantify the microcirculation perfusion in a murine hindlimb IRI model and to determine the potential effect of pharmacological preconditioning with sildenafil on limb perfusion.
Materials and Methods
Animals characteristics
Ten male Swiss mice (12–16 weeks old), provided by JANVIER Laboratories (Saint Berthevin, France), were housed in a thermo-neutral environment at 22°C ± 2°C on a 12-hour day–12-hour night cycle and were given food and water ad libitum. The protocol was approved by the Regional Committee of Ethics in Animal Experimentation of Strasbourg (CREMEAS) and the Ministry of Higher Education and Research (CREMEAS No. 2018060718457300).
HSI system
A complementary metal–oxide–semiconductor (CMOS) push-broom hyperspectral camera (TIVITA®; Diaspective Vision GmbH, Germany), with a 640 × 480 pixel spatial resolution and a 5 nm spectral resolution, within a 500 to 1000 nm spectral range, was used. The camera built-in software provides datasets in about 6 seconds, both as hypercubes and as pseudo-color images, containing information about tissue perfusion. The superficial tissue perfusion metric quantified as false-color images was tissue oxygen saturation (StO2%). StO2 is extrapolated using an algorithm integrated within the camera software, based on two known oxygenated hemoglobin (HbO2) spectral peaks (500–650 and 700–815 nm). 23
Experimental design
A tourniquet-induced 2-hour ischemia was followed by a 30-minute reperfusion period (Fig. 1). The contralateral nonischemic limb served as a control, as supported by previous experiments.7,24 Thirty minutes before ischemia and 5 minutes before reperfusion, sham mice (n = 5) received intraperitoneal NaCl 9‰ (5 μL/g), and sildenafil mice (n = 5) received intraperitoneal sildenafil/NaCl 9‰ (1 mg/kg). The animals were then placed in a hermetic anesthetic induction cage, ventilated with a gas mixture of 4% isoflurane (AERRANE®; BAXTER S.A.S.) and oxygen, and placed on heating blankets (MINERVE®, Esternay, France) at 37°C. Spontaneous ventilation was allowed through an oxygen-delivering mask, with different concentrations of isoflurane depending on the surgical stage (2% during painful stimuli and 1% during latent periods). Both hind limbs were imaged with HSI before commencing ischemia (T0), 5, 30, 60, 120 minutes after ischemia (T5, 30, 60, 120) and 5, 15, and 30 minutes after reperfusion (T125, 135, 150). To avoid interferences from environmental light sources, HSI measurements were performed surrounding the animal with a custom-made removable black chamber. The StO2 quantification was performed at circular region of interest (ROIs) placed at the center of the midfoot of each hindlimb, using the camera-integrated software.

Experimental set-up diagram.
Statistical analysis
All results were expressed as mean ± standard deviation. Data were analyzed using Prism software (GraphPad Prism 8; GraphPad Software, Inc., San Diego, CA), and differences between groups were assessed using one-way analysis of variance (ANOVA) or two-way ANOVA, as appropriate. A P value <.05 was considered significant.
Results
The ischemia, not visible in the RGB pictures, could be easily visualized using HSI in both control and sildenafil group (Fig. 2).
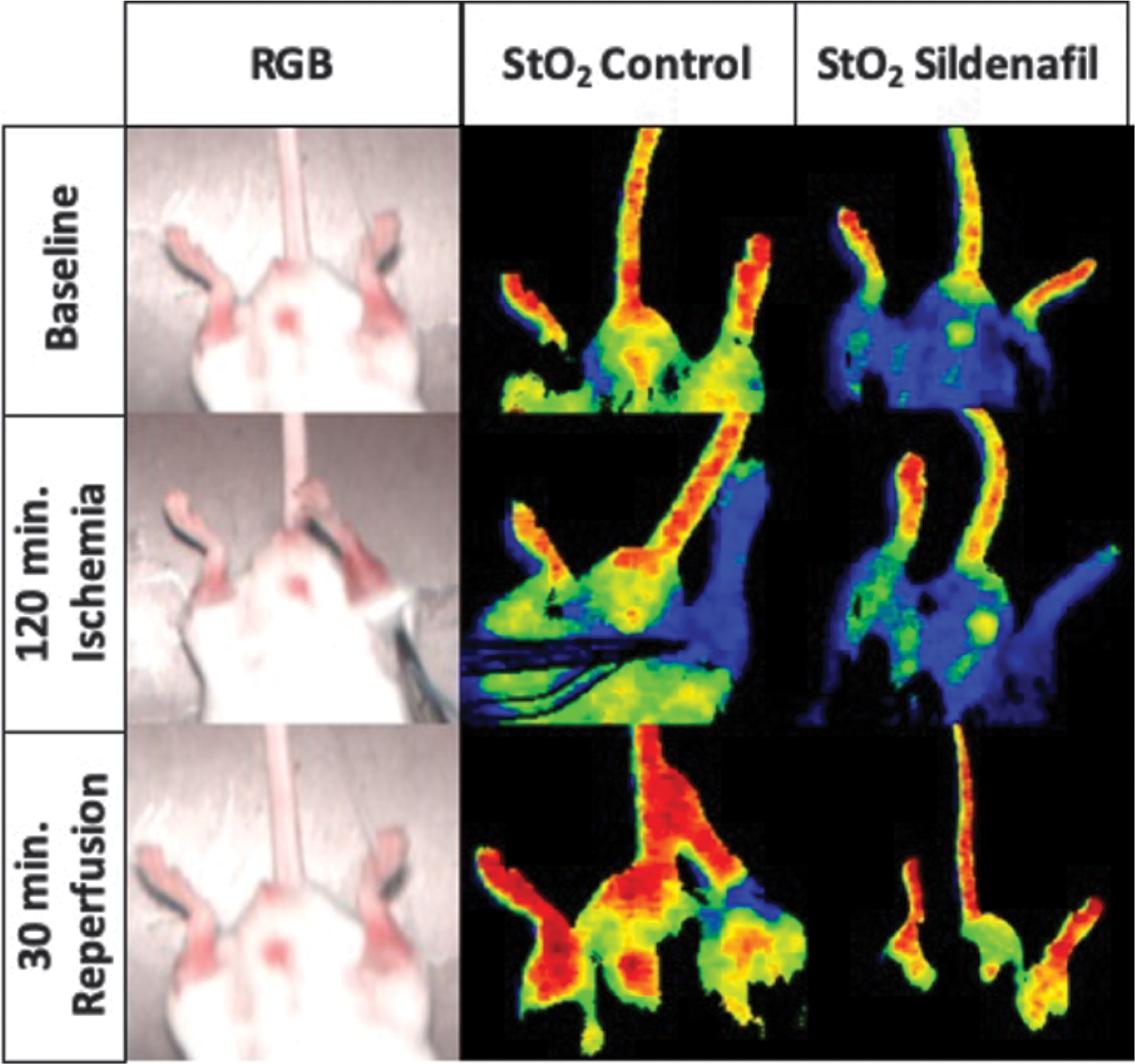
RGB pictures captured with the HSI camera before ischemia, after 120 minutes of ischemia and after 30 minutes of reperfusion are shown in the RGB column. The pseudo-color images generated by means of the HSI system quantify the StO2 content at the different time points, in the control group (central column) and in the sildenafil group (right column) group, respectively. Red areas display the highest StO2 amount, whereas green, yellow, and blue colors incrementally lower perfused areas. HSI, hyperspectral imaging.
The control group showed that StO2 was significantly lower (T120, 24.8% ± 17%, P = .0113) during ischemia and was significantly higher during reperfusion (T150, 76.8 ± 3.77, P = .0008), as compared with the baseline T0 value (53.3% ± 7.04%) (Fig. 3).
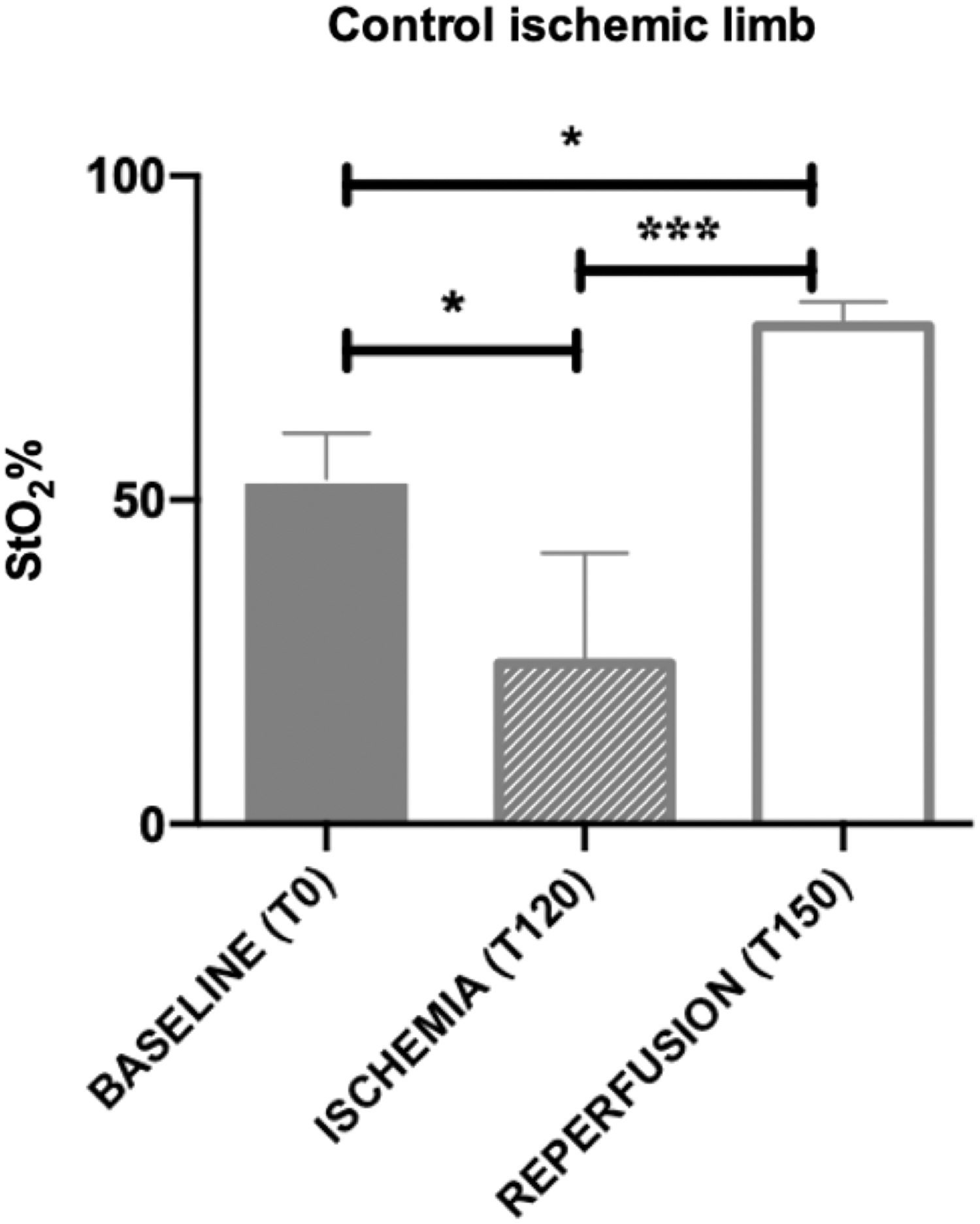
StO2% in the control group at different time points, before ischemia (T0), during ischemia (T120), and during reperfusion (T150) (one-way ANOVA: *P < .05, ***P < .001). ANOVA, analysis of variance.
Similarly, in the sildenafil group, StO2 during ischemia (T120, 28.6% ± 20%, P = .0312) was significantly lower as compared with the T0 value (63.3% ± 8.46%) and reperfusion (T150, 73.3% ± 19.1%, P = .075). However, no difference was found between baseline and reperfusion StO2 (Fig. 4).
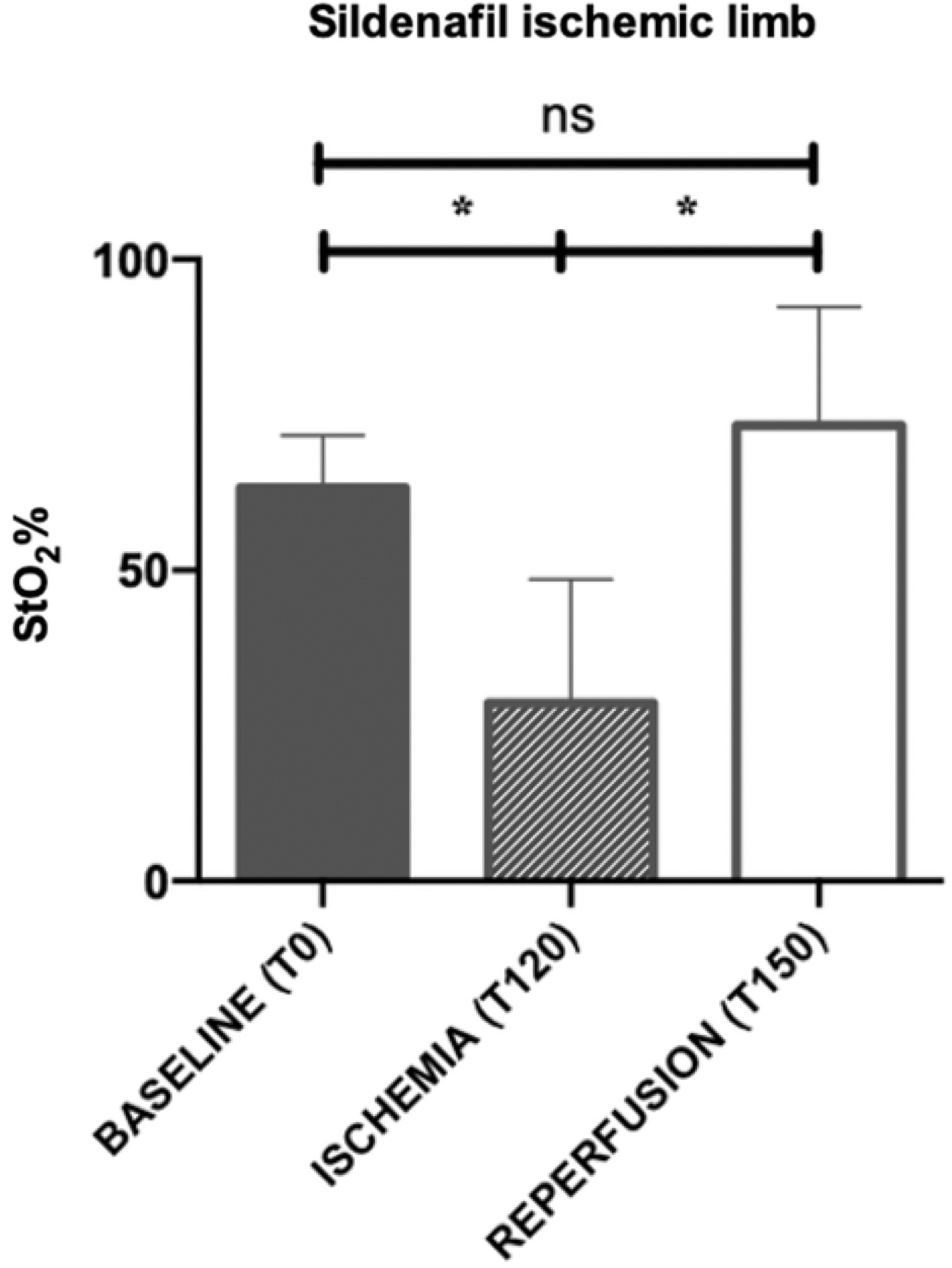
StO2% in the sildenafil group at different time points, before ischemia (T0), during ischemia (T120), and during reperfusion (T150) (one-way ANOVA: ns = P ≥ .05, *P < .05). ANOVA, analysis of variance; ns, non significant.
The comparison of StO2 values at T0, T120, and T150 between the sildenafil and the control group did not show any statistical difference (Fig. 5).
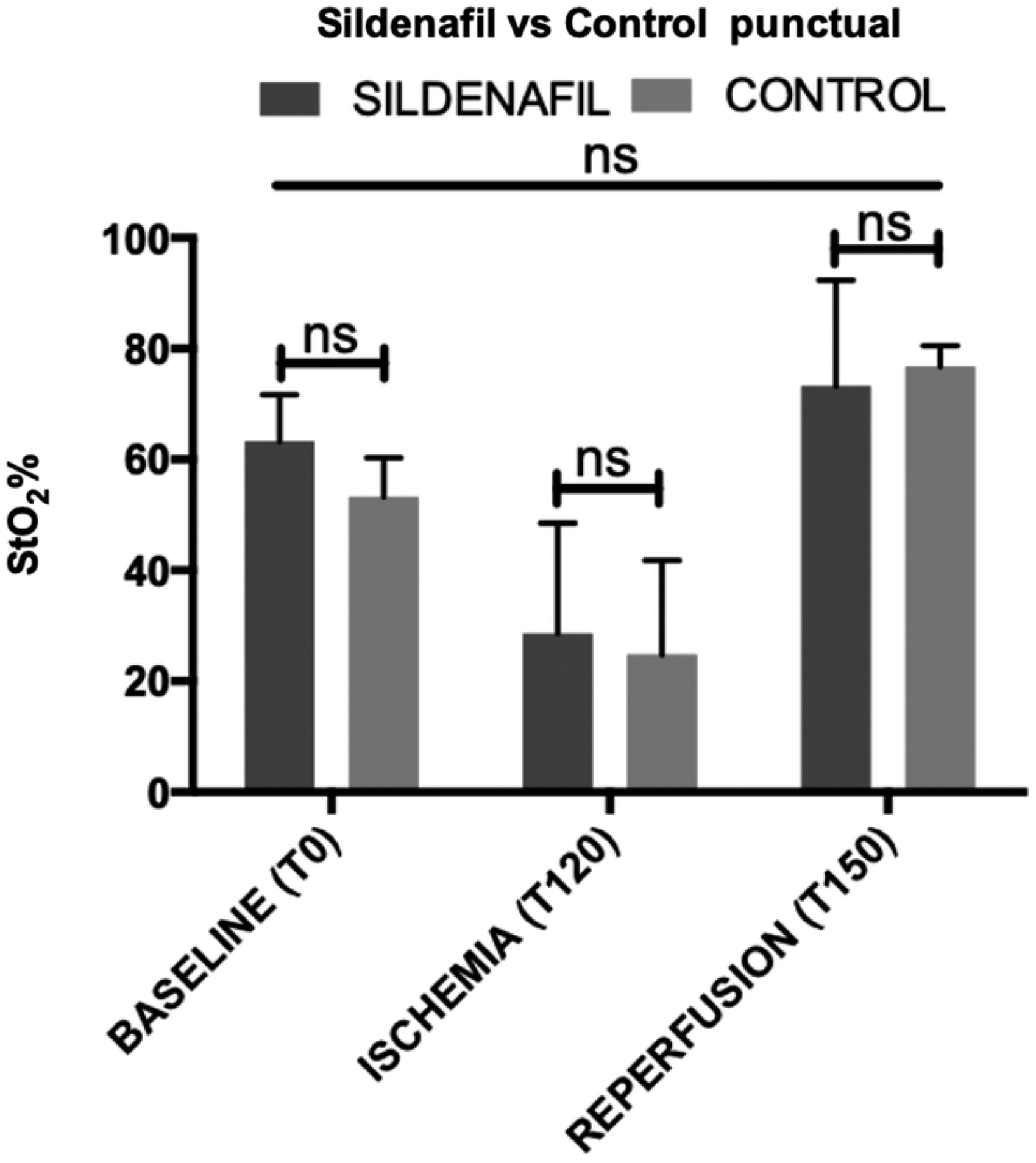
Comparison of StO2% in the control group and in the sildenafil group before ischemia, during ischemia, and during perfusion (two-way ANOVA, ns = P ≥ .05). ANOVA, analysis of variance; ns, non significant.
During the overall ischemic phase, the StO2 mean value of the ischemic limb in the control and in the sildenafil group measured 30.2% ± 13.4% and 30.5% ± 18.9%, respectively. Both had significantly lower values than the mean of the nonischemic limb in both groups (control: 64.0% ± 8.34%; sildenafil: 66.2% ± 5.08%; P < .0001).
During the whole reperfusion phase, StO2 amounts of the ischemic limb were 73.8% ± 0.48% in the sildenafil group and 77.1% ± 1.04% in the control group, whereas StO2 amounts in the nonischemic limb were 74.8% ± 2.59% for the sildenafil group and 75.6% ± 3.45% for the control group, respectively (Fig. 6).
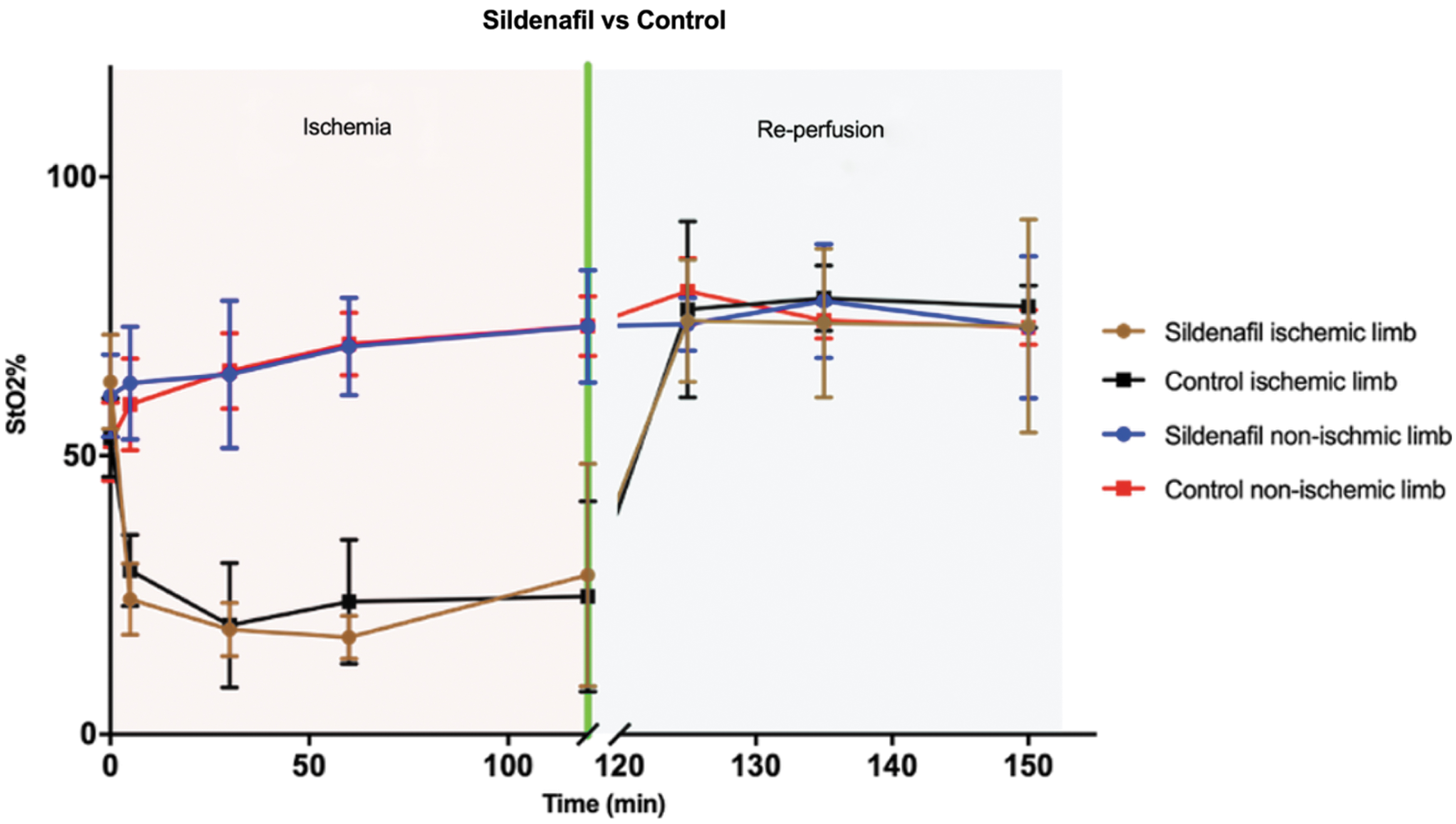
StO2% in both groups: control and sildenafil. The graph shows all the values recorded during the ischemia and reperfusion. Each point is the mean of the five samples with SD. SD, standard deviation.
Discussion
The main results of this study demonstrate that HSI was effective in discriminating nonischemic from ischemic limbs. Additionally, pharmacological preconditioning using the PDE5 inhibitor, sildenafil, did not show any improvement of StO2 over the control group. Previously, several authors reported the use of HSI to evaluate the outcomes of HLI models. Poole et al. 10 used a combination of HSI and optical coherence tomography to assess disease severity and to quantify collateral microcirculation formation in a chronical PAD model, obtained through the ligation and transection of the hindlimb femoral artery in mice. They found that HSI significantly correlated to well-established imaging modalities, such as LDPI and pulse oximetry. Additionally, Grambow et al. used HSI to successfully monitor the outcome of microsurgical anastomoses performed on the rat hindlimb. They utilized the same system that we used in our study and they were able to quantify hindlimb ischemia after clamping of the femoral artery. 25 Our results show a significant StO2 drop after 2 hours of ischemia in comparison to the preischemia baseline and reperfusion phase. Interestingly, in the control group, StO2 after 30 minutes of reperfusion was significantly higher than baseline levels. This result is in line with previous studies on healthy human subjects, in which StO2 was measured using near-infrared spectroscopy (NIRS). 26 NIRS clearly differentiated ischemic from nonischemic phases, and StO2 increases above the baseline were reported during the reperfusion phase. The downsides of NIRS are the necessity to attach several sensors onto the skin surface and the lack of spatial coordinates. In this regard, HSI offers clear advantages over NIRS, as it is contactless and provides an appropriate spatial resolution. This is especially convenient under an experimental setting, since StO2 can be exactly quantified repeatedly during the procedure, thereby providing a kinetic information, and the measurement can be performed exactly at the chosen site of a possible biopsy.
The StO2 values did not show any significant difference in the sildenafil group as compared with the control group at baseline, after 120 minutes of ischemia and after 30 minutes of reperfusion. Accordingly, in a previous study with a similar set-up, in which the protective effect of sildenafil preconditioning against IRI was explored, we could not find any improvement in mitochondrial oxidative and calcium retention capacities within the skeletal muscle in the preconditioning group. 7 A more chronic sildenafil administration may be required to elicit the beneficial perfusion effects of the preconditioning. 7
In conclusion, although sildenafil did not improve StO2, HSI appears to be a promising technology to assess treatment efficacy in murine PAD models, since it is fast, contactless, and nondestructive, and provides an objective and spatially resolved StO2 quantification. As a result, HSI deserves to be further used to assess lower limb IR and to investigate the potential beneficial effects of pharmacologic and/or ischemic conditioning.
Footnotes
Acknowledgment
Authors are grateful to Guy Temporal, professional in medical English proofreading, for his valuable help in revising the article.
Disclosure Statement
J.M. is the President of both IRCAD, which is partly funded by KARL STORZ, Siemens, and Medtronic. M.D. is member of the Board of Diagnostic Green (travel fees). The remaining authors have nothing to disclose.
Funding Information
No funding was received for this article.