
Abstract
Background:
An accurate and reliable localization of endoluminal gastrointestinal (GI) lesions is crucial, particularly during minimally invasive surgery. As an extreme consequence, a misdetected GI lesion can lead to the resection of the wrong segment, especially in colorectal surgery. A preoperative endoscopic marking is recommended in case of GI lesions, which are expected to be difficult to detect from the serosal side. In clinical practice, three preoperative endoscopic marking methods are currently used: India ink, SPOT™, and endoclips with intraoperative fluoroscopy. All of them have substantial limitations. This has encouraged research on alternative solutions.
Methods:
In the current systematic review, animal and clinical studies about alternative preoperative endoscopic marking methods of GI lesions were analyzed using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Results:
Thirty studies were found using PubMed/MEDLINE, EMBASE/Ovid, and the Cochrane Library for the qualitative analysis.
Conclusion:
Although several smart solutions have been proposed and tested successfully, all of them seem to have a substantial drawback related either to scarce stability on the marking site or potential spreading on the bowel wall or diffusion into the surgical planes.
Introduction
An accurate and reliable localization of endoluminal gastrointestinal (GI) lesions is crucial, particularly during minimally invasive surgery, given the lack of tactile sensation.
Intraoperative endoscopy is logistically demanding and time-consuming. Additionally, it may induce bowel distension and reduced visibility. 1
A preoperative endoscopic marking is recommended in case of GI lesions, which are expected to be difficult to detect from the serosal side. And yet, clear guidelines are still lacking.2,3 An ideal endoscopic preoperative tattooing/marking method should be safe and stable. Additionally, it should allow for the precise intraoperative detection of the tumor-bearing segment with minimal impact on the operation workflow and should not impair surgical planes visualization.
The most commonly used methods include the submucosal injection of various substances (tattooing) or the application of endoscopic clips in the peritumoral area. India ink is a carbon-based dye largely used since 19754 as an endoscopic tattooing agent. India ink tattooing is long-lasting (up to several years), 5 but it induces tissue inflammation, due to the presence of stabilizing additive substances, 6 which may lead to complications such as abscess formation,7,8 idiopathic inflammatory bowel disease, 9 adhesion-related ileus, 10 inflammatory tumor, 11 or focal peritonitis.7,12 Subsequently, a sterile suspension of dye based on smaller carbon particles without the proinflammatory additives, the SPOT™, has been introduced and its efficacy and safety have been proven in large series of patients. 6 Nonetheless, a common problem of India ink and SPOT tattooing is the occurrence of intraperitoneal spillage, reported in 2.4%–13% of cases. 13 Not only does this issue seem to be accountable for most of the tattooing-related complications, 3 but it also consistently reduces the visibility of cleavage planes during surgery. 2
Preoperative marking can also be achieved by applying endoluminal metal clips. 14 However, the intraoperative clip identification requires a C-arm fluoroscopy, which implies X-ray exposure for both patient and staff and increases operative time. Additionally, the clips tend to detach spontaneously from the mucosa after 10 days on average. 15
Consequently, India ink, SPOT, and endoclips, which are the most commonly used methods in clinical practice, suffer from several limitations. The aim of the present study was to systematically review the literature on preoperative endoscopic tattooing/marking methods of the GI tract, in search for promising alternatives.
Methods
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Prisma Checklist in the Supplementary Data). 16
A literature search performed on December 30, 2019, was conducted using relevant databases (PubMed/MEDLINE, EMBASE/Ovid, and Cochrane Library). The following search strategy was constructed: “endoscopic AND (tumor OR cancer) AND (tattooing OR marking OR localisation) AND (gastrointestinal OR stomach OR colorectal OR colonic OR colon).” Clinical, experimental trials, systematic/Cochrane reviews, and meta-analysis were included. Exclusion criteria were as follows: conventional methods (India ink, SPOT, fluoroscopy-based clip detection), case reports, ex vivo studies, experimental studies with only one experimental subject, clinical studies in which endoscopy was performed on the same day of surgery, and non-English articles. No date limits for the included studies were set. The primary outcome was represented by the successful intraoperative detection of the GI tract's portion previously targeted, using the alternative endoscopic tattooing/marking method. The secondary outcome was the lack of complications and safety of the method employed.
Two authors (M.B. and M.P.) independently examined the titles and abstracts retrieved from the search, obtaining full texts of potentially eligible studies. Controversies were solved by discussion until consensus was reached. The bibliography of all retrieved articles was additionally evaluated for supplementary amenable publications.
Results
After removal of duplicates, 806 records were obtained, of which 697 studies were excluded after screening titles and abstracts. The remaining 109 articles were fully screened and only 23 articles were selected. Seven additional inherent records were retrieved from the reference lists of the selected articles, and as a result, the number of articles included in the qualitative analysis was 30
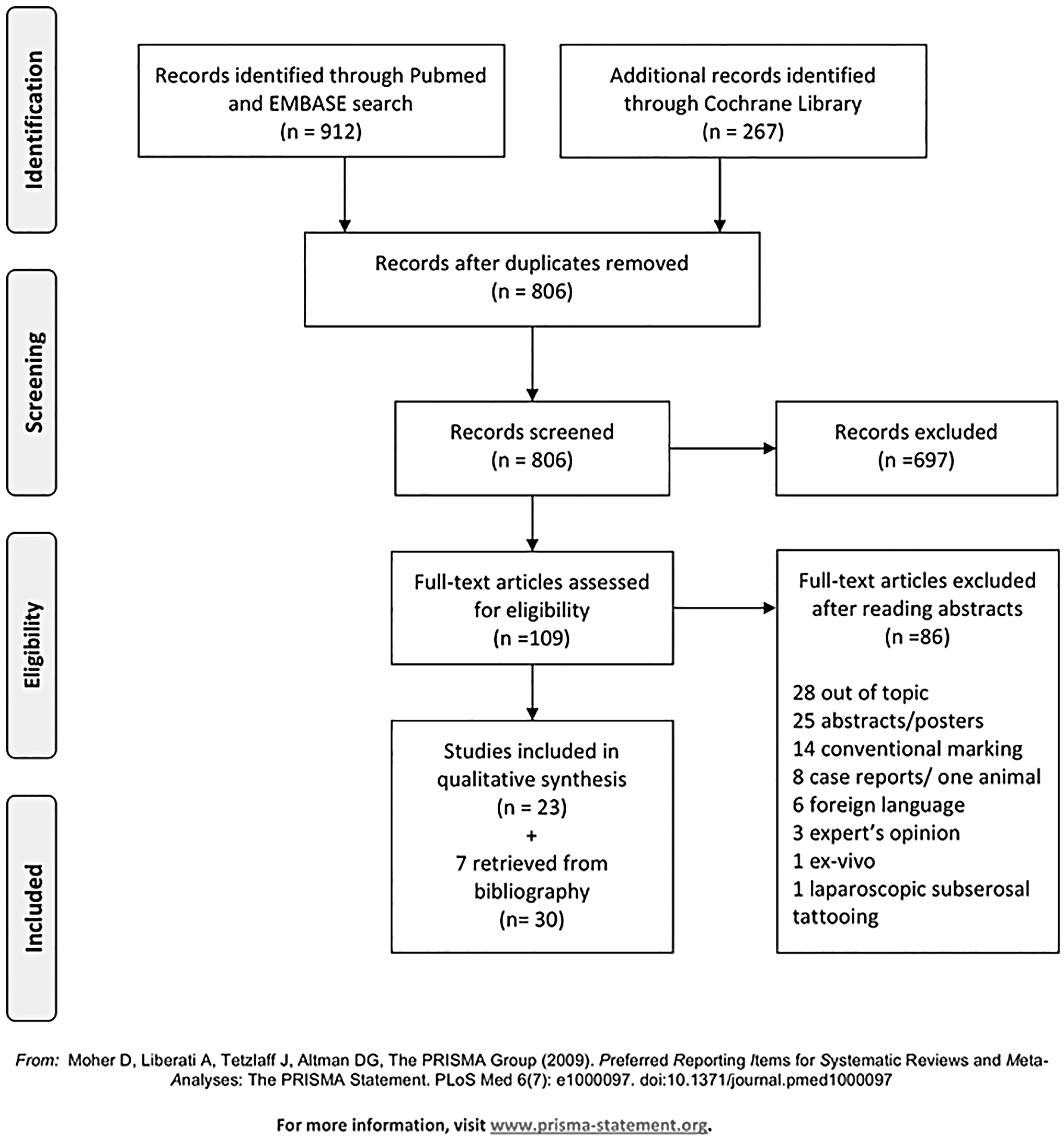
PRISMA flowchart showing the studies analyzed and included in this systematic review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
A schematic representation of the results is reported in detail in Table 1.
All the Works Analyzed in This Systematic Review Are Reported in the Table Together with the Main Outcomes
EUS, endoscopic ultrasound; ICG, indocyanine green; IUS, intraoperative ultrasound; LED, light-emitting diode; NIR, near-infrared.
Indocyanine green under white light
Indocyanine green (ICG) is an inert water-soluble, tricarbocyanine dye, containing 5%–9.5% of sodium iodine. It has been originally used as a contrast agent during ophthalmic angiography or to determine cardiac output or to test the hepatic function. Injected into the tissue at a high concentration, ICG appears to be a brilliant green dye; at lower concentration, it is invisible under white light, but it fluoresces when exited within the near-infrared (NIR) electromagnetic spectral range.
In 1989, Hammond et al. 17 tested several dyes as colonic tattooing agents in a canine model and concluded that ICG remained visible up to 7 days after its submucosal injection, causing a considerably lower inflammatory reaction when compared with India ink. Subsequently, the same authors tested ICG as an endoscopic marking agent for colonic lesions in a series of 12 patients. 18 They demonstrated that ICG submucosal injection is safe and still visible 36 hours after its endoscopic application in 100% of cases.
A few years later, Lee et al. 19 tested the efficacy of ICG and India ink in an experimental comparative survival study in the pig model. The authors observed that after a 14-day survival period, both dyes caused a mild inflammatory reaction at the injection site and that ICG was visible only in 59% of cases, whereas India ink was visible in 92% of all cases.
Miyoshi et al. 20 reported their experience with multiple cases of India ink spillage, including migration of the dye in the peritoneal cavity and subsequent difficult visualization of the dissection planes during surgery. Due to this issue, the authors started to use ICG as a colonic tumor marking agent and described their experience in 39 patients. The dye was visible within 9 days in 100% of the patients, but after 9 days in only 10% of cases. Additionally, they experienced dye spillage in one case without any consequences for the patient nor any impairment during the surgical procedure. Lee et al. 21 had an overall 93.5% detection rate of ICG-marked lesions during laparoscopic colorectal resection. However, in most cases, the dye was applied within 2 days before surgery (95% success rate, 170 of 179 lesions). When visualization was attempted 2 days after endoscopic dye application, the detection rate dropped to 40% (2 of 5 cases). In a retrospective clinical study of 114 patients with colonic lesions endoscopically tattooed with ICG, Park et al. 22 described a 100% detection rate, although the time interval between tattooing and laparoscopic detection was not specified in the article.
ICG under NIR light
The first author to describe ICG coupled to a NIR camera, as a preoperative endoscopic marking agent, was Watanabe in 2009. 23 First, during unpublished animal experiments, the authors found that the best dye concentration was 2.5 mg/mL. Second, in a case series of 10 patients, ICG was injected 1–5 days (mean 3) before surgery in the submucosal space, and it was visualized using an open surgery NIR camera system. The success rate was 100%, whereas the authors reported that only 20% of the tattoos were visible under white light. Similarly, in 2016, Ozawa et al. 24 reported a case series of 3 patients undergoing ICG submucosal injection, in proximity to colonic lesions, at the same concentration used by Watanabe et al., 1–2 days preoperatively and visualized it using an NIR system. In this study, the authors performed surgical resection laparoscopically and used a minimally invasive NIR camera system, achieving a 100% visualization rate. Nagata et al. 25 reported similar results in a clinical study with 24 patients having colonic lesions. Interestingly, in this study, the authors injected ICG and India ink simultaneously at each lesion site and could visualize India ink in only 41% of the cases, whereas ICG was visible under NIR light in 100% of cases.
Subsequently, Watanabe et al. injected one submucosal spot of 0.5 ICG (2.5 mg/mL) endoscopically 1–17 days before surgery, 26 in 80 patients undergoing laparoscopic colonic resections. For intraoperative visualization, an NIR laparoscopic camera was used, and the overall success rate was 93.8%. Interestingly, the visualization rate increased to 98.7% if the interval between tattooing and operation was <7 days.
In 2019, Ushimaru et al. applied four spots of low-dose ICG (0.05 mg/mL) endoscopically in patients undergoing laparoscopic gastrectomies 1 day before surgery. 27 In this study, 84 patients who received ICG were compared through a propensity match score with 174 historical patients who did not undergo any preoperative tattooing of the lesion. The intraoperative tattoo detection rate was 100%, and partial gastrectomy resection lines were always negative in the ICG group. Interestingly, since ICG is a rather small molecule and tends to diffuse into the interstitial tissue, the authors measured the ICG expansion rate and found it to be 2.5 cm on average in all four directions, with maximal peaks of 7 cm.
During the same period, another group 28 published a study of 18 patients undergoing laparoscopic partial gastrectomy. The authors applied one to three spots of 0.1 mL of ICG at a concentration of 1 mg/mL in the submucosal space before laparoscopic gastric resection. The intraoperative detection rate was also 100%.
Carbon nanoparticles
In the last few years, nanosized carbon particles, with an average diameter of 150 nm, have been used for the tattooing of several tumors and for lymph node tracking.29,30 Given the ability of these nanoparticles to enter the lymphatics rather than the blood vessels and the few side effects, Wang et al. described, for the first time, preoperative endoscopic colonic tattooing with submucosal injection of nanosized charcoal particles in a series of 26 patients in 2013. The authors demonstrated an intraoperative identification rate of 100% of the marked lesion, up to 14 days following endoscopic tattooing. 31 Subsequently, the same authors conducted a retrospective study on colonic tumor marking, comparing 27 patients preoperatively tattooed with carbon nanoparticles and 27 patients not tattooed. They observed that carbon nanoparticles were always well visible during laparoscopy with a significantly shorter time to detect the tumor-bearing bowel segment (2.71 ± 2.13 min vs. 6.91 ± 5.16 min, P < .001) in the tattooed group. Additionally, a shorter operation time (151.22 ± 30.66 min vs. 170.26 ± 33.13 min, P = .033) and less intraoperative blood loss (125.04 ± 29.48 mL vs. 147.52 ± 34.35 mL, P = .013) were reported in the tattooed group. 32 Recently, Lin et al. reported 3 cases of endoscopic ultrasound-guided submucosal injection of carbon nanoparticles for tattooing tumors at the level of the esophagogastric junction 1 week before surgery. The tattoo was quickly visible in 100% of patients and the operations were laparoscopically completed within 3 hours. 33
Autologous blood injection
In 2012, Jeong et al. described a preoperative endoscopic tattooing technique in patients with early gastric cancer using the patient's own blood. 34 The authors performed a gastroscopy 1 day before surgery in 23 patients and injected 2–3 mL of venous blood, simultaneously sampled from the patient, in the submucosal space. An intraoperative visualization success rate of 100% without any complication has been reported.
A few years later, another group described their experience using the patient's autologous blood for preoperative endoscopic tattooing of colonic lesions. 35 The retrospective study was conducted in 25 patients, and preoperative marking was performed injecting 5 mL of blood submucosally proximal and 5 mL distal to the lesion. The reported intraoperative success rate was 92% and no complication occurred.
Endoclips identified using intraoperative ultrasound
In 1999, Montorsi et al. 36 first described the preoperative marking (1–9 days before surgery) of small colonic lesions using regular endoclips, which were identified intraoperatively using laparoscopic intraoperative ultrasound (IUS), in a series of 8 patients. The identification rate was 100%, and the time required for IUS ranged from 5 to 17 minutes.
Hyung et al. 37 described a similar technique in 17 patients undergoing laparoscopic gastric resections: the clips were applied endoscopically 1–2 days before the surgical procedure and detected using laparoscopic IUS. The success rate was 100%, and the mean IUS time ranged from 2 to 8 minutes.
Subsequently, Nagata et al. 38 performed a study in 17 patients undergoing laparoscopic colonic resections, in which endoclips were applied preoperatively close to the lesion. In one group, the clips were intraoperatively colocalized using a standard C-arm fluoroscopy, and in another group, a laparoscopic IUS was performed. They achieved a 100% success rate in both groups. However, they reported that the time used to find the clip with IUS (7.0 minutes, range: 4–12 minutes) was significantly shorter than the time required for fluoroscopic search (15.8 minutes, range: 10–28 minutes).
Recently, the same preoperative endoscopic marking method has been used in 11 patients undergoing minimally invasive esophageal resection. The average laparoscopic IUS time was 6.5 minutes (range: 5.2–9 minutes), with a 100% success rate. 39
Endoclips identified using a metal detector
A Japanese group performed two studies involving patients who underwent laparoscopic colonic resections 40 and laparoscopic gastric resections 41 and who received an endoscopic tumor marking using regular endoclips preoperatively. Interestingly, the authors used a marking clip detector system (MCDS), a modified laparoscopic version of a metal detector system, to identify the tumor-bearing segments intraoperatively. With this device, they reported a 100% success rate and a short intraoperative localization time.
Subsequently, the same authors used modified magnetic endoclips to mark neoplastic lesions in patients undergoing laparoscopic colonic 42 and gastric 43 resections preoperatively. A small round magnetic body with a maximum magnetic flux density of 320 mT was attached with a nylon thread to commercially available endoclips.
The MCDS was used to detect the magnetic clips intraoperatively and a 100% detection rate was reported.
Marked endoclips
Kojima et al. described his experience using a specially designed endoclip with a radiofrequency identification tag in an experimental study in 11 dogs. 44 The clip was applied endoscopically on the gastric mucosa and then detected laparoscopically in ∼30 seconds, using a custom-made laparoscopic radiofrequency probe. The identification rate was 100%.
In the preoperative period, a Korean group applied a modified endoclip, attached through a nylon thread to a small magnetic ring, in 25 patients with either small gastric or colonic lesions. 45 The intraoperative detection, which occurred in <1.30 minutes, was performed using a magnetic ring connected to a laparoscopic probe. Once the intraluminal and the intra-abdominal magnets were mated, the detection was completed. The authors described a 100% success rate with this technique.
Recently, Wada et al. 46 described their remarkable experience in detecting colorectal lesions in 3 patients using a newly developed endoclip. The device is composed of a small light-emitting diode (LED) attached to a standard endoclip with the addition of a laparoscopic power source, which is capable of electromagnetic power transfer. When the laparoscopic power source probe is in proximity to the novel clip, the LED is activated, and the tumor-bearing segment can be easily detected. The reported detection rate was 100%.
Devices
A German group 47 developed an over-the-scope magnetic ring device, which could be attached to the mucosa using standard endoclips and could be detected laparoscopically using any ordinary ferromagnetic laparoscopic instrument. The authors used this system successfully in 28 patients undergoing laparoscopic colorectal resections. They reported device migration in one patient, in whom the magnetic device was applied 2 days before surgery. In the rest of the patients, the endoscopic marking was performed at most 1 day preoperatively.
Another research group 48 reported their experience using an engineered ICG-embedded rubber band. In an experimental study in pigs, the authors applied the devices on the gastric and colonic mucosa of the animals endoscopically. They were then able to visualize the marked sites by means of fluorescence imaging, using a laparoscopic NIR camera system. The reported visualization rate was 100%.
Discussion
When performing minimally invasive procedures, the haptic feedback is reduced. As a result, it is sometimes difficult to detect GI intraluminal lesions from the serosal side. As an extreme consequence, this can lead to the resection of the wrong segment, especially in colorectal surgery, 49 with dramatic consequences for the patient, including conversion to open surgery or further resection. 50 For this reason, a reliable preoperative marking of the lesion-bearing portion is crucial.
The ideal endoscopic marking method should offer long-lasting, safe, and straightforward intraoperative detectability. Although India ink and SPOT provide efficient and durable tattoos, the first one can produce severe complications,7–12 whereas the second one is safer. Both dyes are visible under white light. Consequently, in case of intraperitoneal spillage, they might conceal the surgical planes, 20 substantially complicating the procedure. The marking with endoclips is safe. However, intraoperative detection using fluoroscopy has a high impact on the surgical workflow. As a result, the drawbacks of the existing preoperative marking agents have triggered research on alternative solutions.
ICG, injected into the submucosal space and then intraoperatively detected under white light, presents, similarly to carbon-nanoparticle-based dyes, a reduced risk of complications. Nevertheless, both dyes could still interfere with surgical plane visualization. On the contrary, the use of ICG coupled to an NIR camera system allows to prevent this issue since the dye at a smaller dose is invisible under normal light. The surgeon needs to actively switch the camera system in the NIR mode to detect the tattooing and, since the dissection phase is generally performed under white light, the ICG staining does not impair this part of the procedure. The main drawback of ICG is its scarce longevity, with a visualization window of 8 days maximum.20,26 In addition, since ICG is a small hydrophilic molecule, it diffuses largely within the tissue. In fact, a fluorescence spreading up to 7 cm from the injection site has been reported, 27 and this could theoretically lead to lesion misdetection. Although tattooing using autologous blood is a cheap and smart solution, its intraoperative detection has to occur within 2 days maximum.34,35 In many of the analyzed studies, either standard25,36,37,39–41 or modified42–46 endoclips were used as alternative marking techniques. In these cases, the authors suggested different remarkable intraoperative detection solutions including IUS,36–39 modified metal detectors,40–43 magnetic interaction, 45 electromagnetic probes, 44 and LED activation using radiofrequency power transfer. 46 Nevertheless, since all endoclips have an unpredictable spontaneous detachment rate (10 days on average), poor longevity of endoclips is a clear limitation to all those alternative techniques. 15 Likewise, a poorer durability might also be an issue for the noteworthy fluorescent rubber band engineered by Hyun et al. 48 This device was tested solely within an acute experimental setting, and it is notorious that elastic esophageal varices bandings are associated with high spontaneous release rates. 15
The interval between diagnosis and surgical removal of colorectal and gastric cancer is in average of 4–6 weeks. 51 An ideal preoperative GI lesion marking agent should be placed during the diagnostic endoscopy and stay in place until surgery. This would avoid performing additional preoperative endoscopic procedures exclusively to mark the lesion, which result in patients' discomfort and increase of the overall care costs. The only existing durable agents are the carbon-based tattooing India Ink and SPOT, which are far from being the ideal preoperative marking agents, since they might provoke concealment of the correct surgical dissection plane, increasing substantially the operation difficulty degree. For this reason, there is an opportunity window for new research on this topic.
Hereinafter, inspired by the findings of this review, our group recently engineered a fluorescently coated over-the-scope clip, using a biocompatible polymer.52,53 Over-the-scope clips do not dislodge even 2 months after their application. 54 As a result, they might be long-lasting as endoluminal marking agents. The efficacy of this clip as an endoscopic marking agent, coupled to a laparoscopic NIR system, is currently explored in an ongoing survival experimental study at our research facility.
Conclusion
In conclusion, the analyzed studies included in this systematic review still present substantial drawbacks, which are summarized either as scarce stability on the marking site or as potential spreading on the bowel wall or diffusion into the surgical planes, although a number of authors proposed several creative and smart solutions. Consequently, ideal preoperative tattooing means have yet to be found.
Footnotes
Acknowledgment
The authors are grateful to Guy Temporal and Christopher Burel, professionals in medical English proofreading, for their valuable help in revising the article.
Disclosure Statement
Jacques Marescaux is the President of IRCAD, which is partly funded by KARL STORZ, Siemens, and Medtronic. Michele Diana is member of the board of Diagnostic Green (travel fees) and is the recipient of the ELIOS grant. Manuel Barberio, Margherita Pizzicannella, Giovanni Guglielmo Laracca, Mahdi Al-Taher, Andrea Spota, and Eric Felli have no conflicts of interest or financial ties to disclose.
Funding Information
This work was funded by the ARC Foundation through the ELIOS (Endoscopic Luminescent Imaging for precision Oncologic Surgery) grant.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.