
Abstract
Introduction:
Cholecystectomy is the most frequently performed procedure in general surgery. The consent procedure for cholecystectomy needs to inform patients about the possibility of subtotal cholecystectomy (STC) as an alternative procedure used for “difficult gallbladders” as it is associated with increased postoperative morbidity. We sought to determine the quality of informed consent for patients who were scheduled for cholecystectomy but underwent STC, and evaluate whether patient or procedural factors influenced the information discussed in consenting.
Materials and Methods:
We classified 57 components of information necessary for a patient to give informed consent for cholecystectomy. We retrospectively reviewed the consent forms of patients scheduled for conventional cholecystecomy but instead undergoing STC between 2011 and 2017. Consent quality was measured as the percentage of components completed. Subgroup analyses were conducted to determine whether age, gender, American Society of Anesthesiologists grade, setting (elective/nonelective), operation mode (open/laparoscopic), or the responsible surgeon affected consent quality.
Results:
Across 174 patients, just 9 (5.2%) had been informed about the possibility of undergoing STC, whereas the overall quality of consent was 37.5%. Patient and setting-specific factors affected the completion of specific consent components. Patients were more likely to receive a patient information leaflet if they were female (relative risk [RR] 2.76; 95% confidence interval [CI] 1.09–7.00), <60 years (RR 3.32; 95% CI 1.39–7.90) or undergoing laparoscopic surgery (RR 8.04; 95% CI 2.50–25.88).
Conclusion:
The suboptimal quality of consent and multiple inconsistencies in the information disclosed to different patient cohorts emphasize the need for a more transparent and consistent consenting process.
Introduction
A
Cholecystectomy is one of the most common procedures performed by general surgeons. About 70,000 cholecystectomies are performed every year in the United Kingdom, with 92% of them performed laparoscopically. 3 In recent years, multiple studies have demonstrated a considerable degree of variation in the quality of consenting for cholecystectomy. One study found that the information presented to patients was inconsistent and inadequate for making an informed choice. 4 Unsatisfactory patient comprehension of cholecystectomy and its key risks has also been described. 5 Recordings of doctor–patient consultations, in which doctors were utilizing standardized consent forms, have revealed that an average of just 37% of the information components found on the form were actually discussed with cholecystectomy patients. 6 Patient comprehension of cholecystectomy is frequently low, but their level of understanding has been shown to be affected by the grade of their consenting physician 4 or patient factors such as age 5 and education level. 7 The consistency and quality of consenting for surgical procedures has been improved with the use of procedure-specific consent forms, 8 including those specific to cholecystectomy. 9 However, cholecystectomy-specific consent forms have not been widely adopted in the United Kingdom and significant variation in their use has been reported across 121 National Health Service Trusts. 10
In the event of conversion from conventional cholecystectomy to subtotal cholecystectomy (STC), perioperative morbidity rate increases to 32%. 11 The primary endpoint for this study was to provide real-world evidence of the overall quality of informed consenting for patients who were listed for conventional cholecystectomy but instead underwent STC. The analysis of such patients, representing a higher-risk cholecystectomy patient subpopulation, can emphasize the importance of transparency and detail in informed consenting for cholecystectomy. A secondary endpoint was to further explore whether the quality of informed consent was influenced by factors such as the responsible consultant, the patients' age, gender or fitness grade, or procedural factors such as the surgical setting and operation mode.
Materials and Methods
Patient selection
The retrospective audit project was carried out at Aintree University Hospital, Liverpool, United Kingdom; a tertiary hepatobiliary surgery center for the region. Business Intelligence Service of the Trust provided the total number of cholecystectomies performed between 2011 and 2017 and the unit numbers of the patients who underwent STC for benign symptomatic gallbladder disease. We included all adult patients (≥18 years) who were consented for conventional cholecystecomy but instead underwent STC.
Indicators of quality of consent
To assess the quality of consent, we first identified the components of information that we deemed necessary to be discussed with a patient in order for them to provide informed consent for conventional cholecystectomy. Overall, 57 components of information were identified. These were divided into administrative and generic surgical components—including entry details, patient information, end documentation, intended benefits of the procedure, anesthetic information, and materials to be used during surgery—and cholecystectomy-specific components, which included the intraoperative risks, postoperative risks, other procedures that may be required, and alternative options to conventional surgery. The cholecystectomy-specific risks were selected based on a combination of expert opinion and the results of a literature search.
Data extraction
The hospital management software (SIGMA) was used to retrieve the included patients' informed consent forms, the name of the responsible surgeon, the patient's gender, age, American Society of Anesthesiologists (ASA) fitness grade, surgery setting (elective/nonelective), and operation mode (open or laparoscopic). Cholecystectomies that converted to open STCs were categorized as open. The consent forms for each of the included patients were retrospectively studied to identify the components that had been adequately covered during the consenting process. Several of the required components, such as entry details, anesthetics and patient information were present as tick box prompts on the hospital's generic surgical consent forms. If these prompts were ticked, it was assumed that the component had been discussed. Other components of information, including intended benefits, intra- and postoperative risks, materials to be used during surgery, and alternative options to conventional cholecystectomy, were not present as prompts on the consent form and so were discussed at the discretion of the consenting surgeon. We identified these components as “discussed” if information was found to suggest that the component had been discussed, or ‘not discussed’ if no information was found.
Management of data and statistical analysis
Initial data were inserted into Excel (Version 2011 for Mac®) database and scrutinized for completeness and plausibility before statistical analyses were performed. The overall quality of consent was calculated as the percentage proportion of the 57 components of information that were discussed with the patient during the consenting procedure. The mean percentage of components covered per patient was compared between different consultant surgeons to determine whether there was any variation in consenting quality. All conventional summary descriptive statistics from the categorical variables included 95% confidence intervals (CIs) for an individual sample proportion, calculating following the Wilson procedure.12,13
We divided the included patients into five subgroups based on their demographics, fitness, and other clinical factors. They were categorized as follows: gender, age (whether they were <60 or ≥60 years), ASA grade (1–2 or 3–5), surgical setting (elective or nonelective), and mode of operation (open or laparoscopic). Chi-square analyses were conducted using IBM SPSS Statistics (Version 23 for Windows) to check for overlapping distribution between the different patient cohorts. For each comparison, the mean quality of consent was compared between the two contrasting subgroups of patients. To determine whether any of the patient or setting-specific factors affected the probability of any of the individual consent components being discussed, we used the relative risk (RR) model. The calculations of RRs and associated 95% CIs were performed using Review Manager 5.
Results
Characterization of included patients
Overall, 2321 conventional cholecystectomies and 180 STCs (7.2% of all cholecystectomies) were performed for benign gallbladder disease. Of the 180 STC patients, 6 were excluded from the audit as they were initially consented for other procedures or were not consented formally due to a loss of consciousness or lack of capacity to consent. The average age of the 174 included patients was 58.2 years (range 24–82) with 89 patients (51.1%) aged <60 years and 85 patients (48.9%) aged ≥60 years. There were 103 female (59.2%) and 71 male patients (40.8%). Categorized by fitness grade, 29 patients were identified as in ASA class 1 (16.7%), 106 were in class 2 (60.9%), 35 in class 3 (20.1%), 3 in class 4 (1.7%), and 1 patient in class 5 (0.6%). The surgery setting was elective for 116 patients (65.9%) and nonelective for 58 patients (33.1%). Cholecystectomy was performed laparoscopically in 83 cases (47.7%), whereas there were 91 cases of open surgery (52.3%). Chi-square analysis revealed statistically significant correlation between the subgroup of female patients and the laparoscopic subgroup (p = .006). There was no significant overlap between any other combination of subgroups.
Overall completion of consent components
On average, just 37.5% of the 57 consent components (95% CI 36.5–38.5) were discussed with patients before gallbladder surgery. Figure 1 shows the percentage proportions of patients for which each administrative or generic surgical component was discussed. Administrative components, such as entry details (79.5% overall, 95% CI 76.3–82.3), end documentation (69.4% overall, 95% CI 66.6–72.2), and patient information (84.9% overall, 95% CI 81.5–87.7) were completed frequently. However, only 25 patients (14.4%, 95% CI 9.9–20.4) were provided with cholecystectomy-specific patient information leaflets. None of the materials to be used during surgery were discussed with a single patient (0.0%, 95% CI 0.00–0.02).
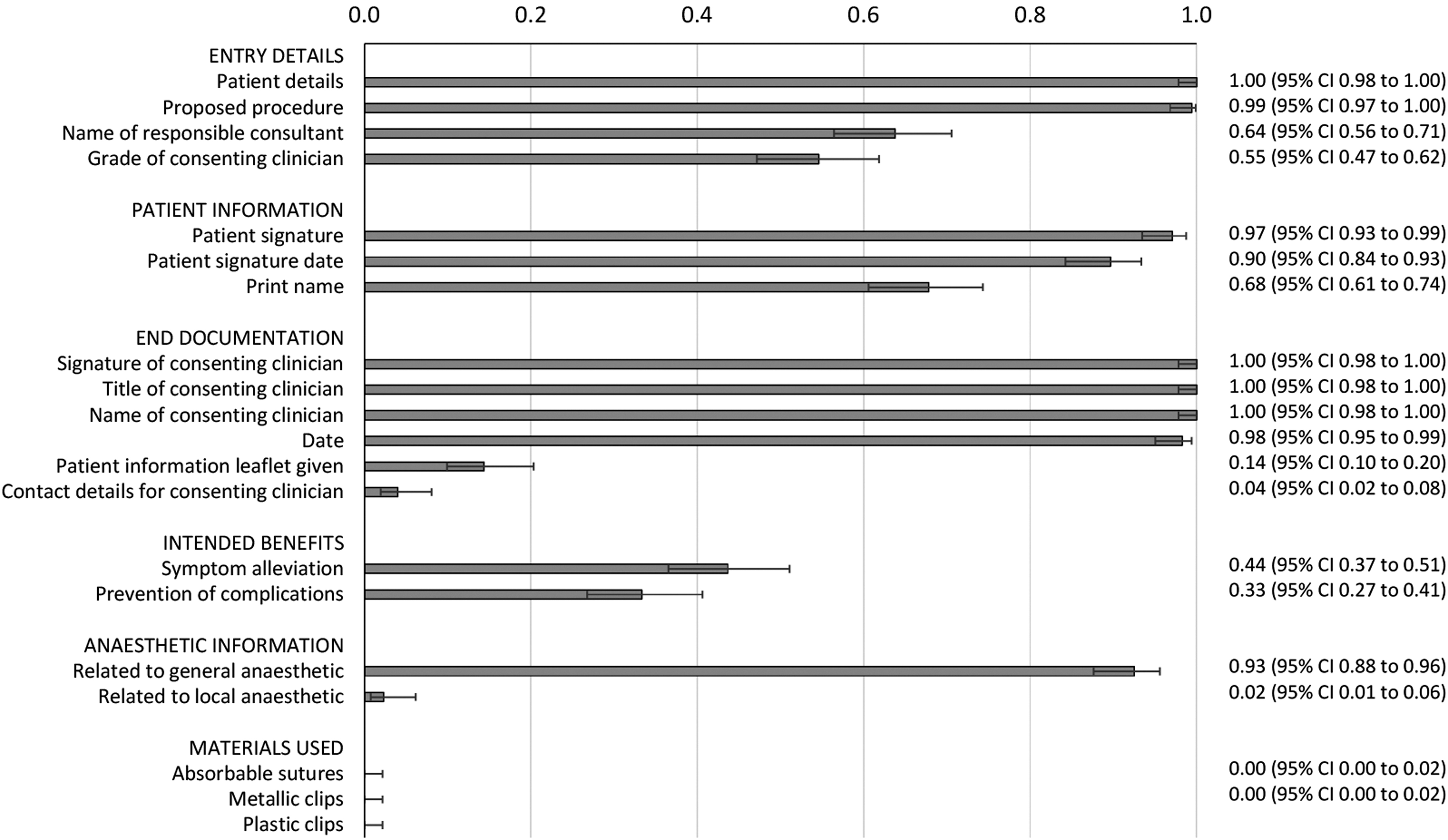
Twenty administrative and general surgical consent components were identified as necessary for patients to give informed consent for cholecystectomy. The percentage of STC patients with whom each component was discussed are shown with 95% CIs. CI, confidence interval; STC, subtotal cholecystectomy.
Figure 2 shows the percentage proportions of patients for which each cholecystectomy-specific component was discussed. Several potential risks were discussed frequently with patients; postoperative bleeding was discussed with 167 (96.0%; 95% CI 91.9–98.0), gastrointestinal injury with 105 (60.3%; 95% CI 52.9–67.3), damage to bile ducts with 162 (93.1%; 95% CI 88.3–96.0), postoperative infection with 154 (88.5%; 95% CI 82.9–92.4), pulmonary embolism with 126 (72.4%; 95% CI 65.3–78.5), and deep vein thrombosis with 137 (78.7%; 95% CI 72.1–84.2). However, the risks of cardiac disorders (n = 11, 6.3%; 95% CI 3.6–11.0), bile spillage (n = 7, 4.0%; 95% CI 2.0–8.1), gallstone spillage (n = 4, 2.3%; 95% CI 0.7–6.2), and diathermy-induced injuries (n = 0) were very rarely discussed with patients. Unscheduled procedures that may potentially have been required (11.6% overall, 95% CI 10.2–13.2) and alternative treatment options (3.2% overall, 95% CI 2.2–4.6) were also discussed infrequently. Alarmingly, just 9 of the 174 patients receiving STC (5.2%, 95% CI 2.7–9.5) had been notified about the possibility of STC as an alternative surgical management.
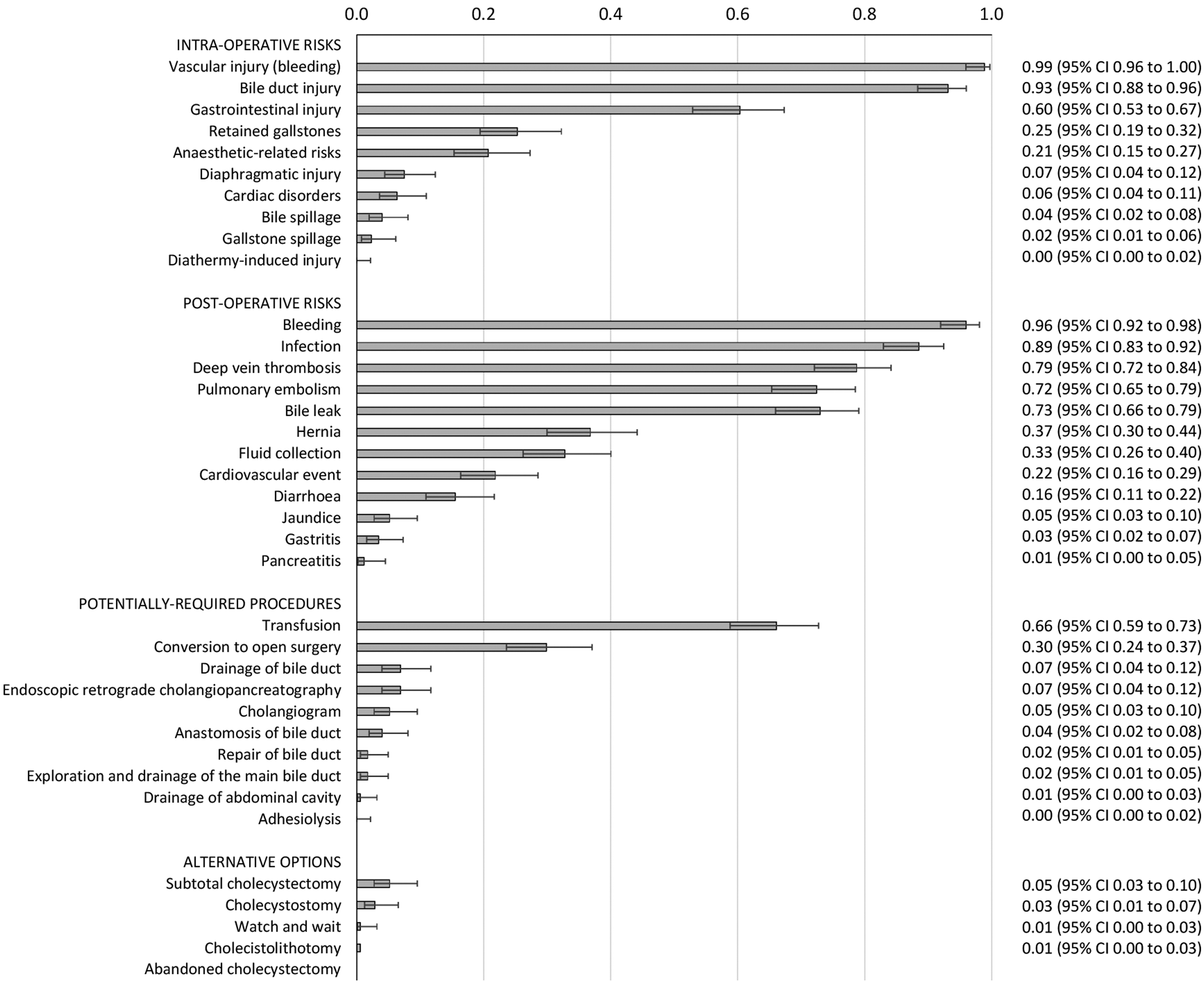
Thirty-seven cholecystectomy-specific consent components were identified as necessary for patients to give informed consent for cholecystectomy. The percentage of STC patients with whom each component was discussed are shown with 95% CIs.
Influence of variables on the likelihood of completion of consent components
The overall quality of consent varied significantly between the 17 individual consultant surgeons included in the study, ranging from 42.1% of consent components covered (95% CI 39.9–44.4) to 28.1% (95% CI 18.1–40.8). No differences in the overall quality of consent were seen across the comparisons of gender, age, ASA grade, surgery setting, or operation mode. However, when considered individually, specific components of consenting information were significantly more likely to be raised with certain patient groups. Figure 3 provides a summary of the administrative and general surgical components that were found to be discussed more frequently with a particular patient subgroup. For example, we found that patient information leaflets were more likely to be provided to women than men (RR 2.76; 95% CI 1.09–7.00), more than three times more likely to be given to younger patients than those >60 years (RR 3.32; 95% CI 1.39–7.90), and eight times more likely to be given to patients who undergo a laparoscopic procedure compared with those who underwent open surgery (RR 8.04; 95% CI 2.50–25.88). Laparoscopic patients were also somewhat more likely to be informed of the name of the responsible consultant (RR 1.29; 95% CI 1.03–1.62), the grade of the consenting physician (RR 1.61; 95% CI 1.19–2.18), and the benefits of the procedure, including both symptom alleviation (RR 1.97; 95% CI 1.25–3.12) and the prevention of complications (RR 1.99; 95% CI 1.38–2.86).
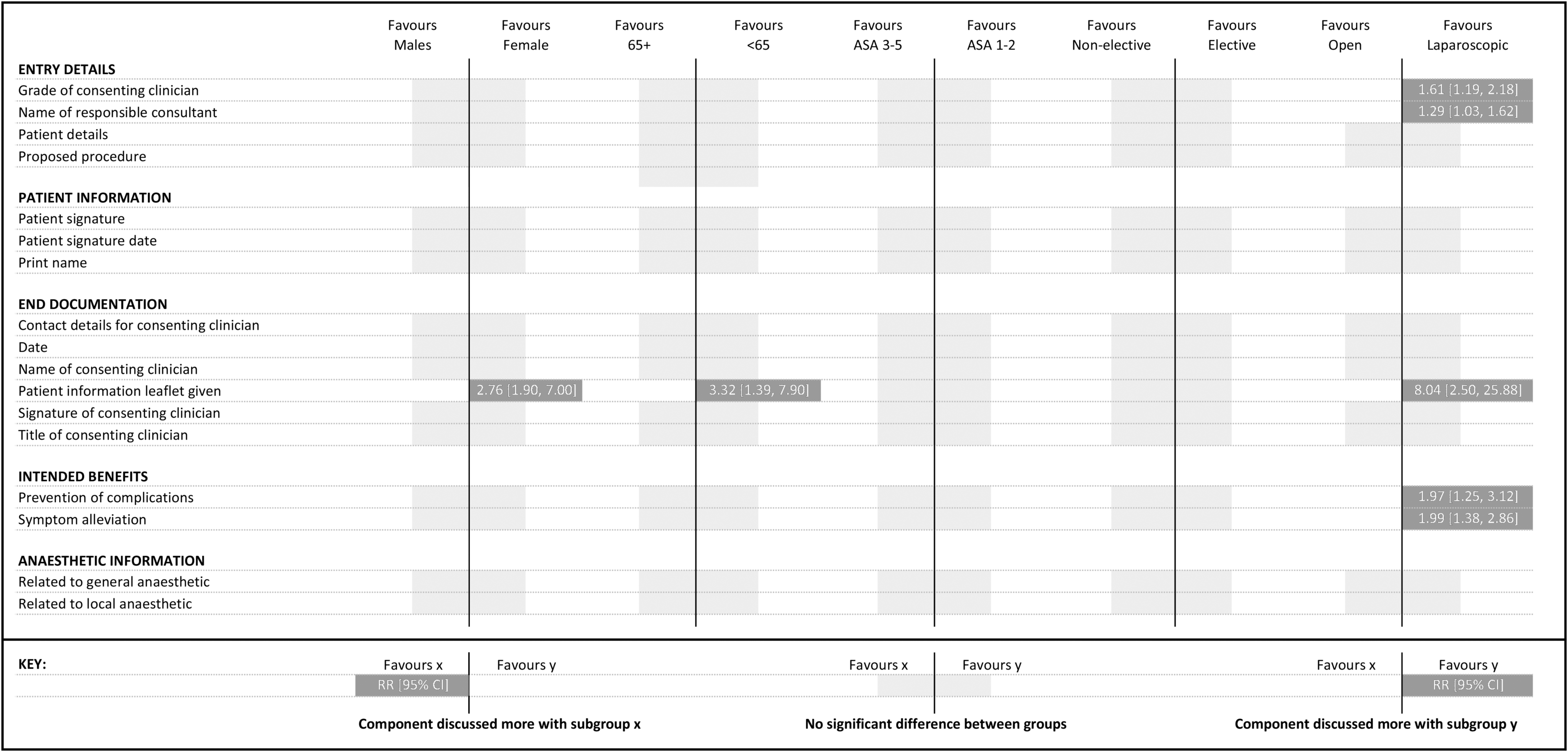
Summary of the administrative and general surgical consent components for which the likelihood of being discussed with a patient was impacted by patient's gender, age group or ASA fitness grade, surgical setting, or mode of operation. ASA, American Society of Anesthesiologists.
Similar discrepancies were seen in the likelihood of individual cholecystectomy-specific components being discussed (Fig. 4). Particularly, elective patients appeared to receive far less information about the potential risks of cholecystectomy than their nonelective counterparts. With elective patients, consenting surgeons were less likely to discuss the risks of bile spillage (RR 0.20; 95% CI 0.04–1.00), intraoperative cardiac disorders (RR 0.29; 95% CI 0.09–0.94), gastrointestinal injury (RR 0.78; 95% CI 0.62–0.99), cardiovascular accidents (RR 0.56; 95% CI 0.32–0.97), postoperative fluid collection (RR 0.56; 95% CI 0.37–0.84), pulmonary embolism (RR 0.84; 95% CI 0.70–1.00), or the potential requirement to convert to open surgery (RR 0.63; 95% CI 0.40–0.99). Elective patients were, however, more likely to be warned about the risk of postoperative diarrhea than nonelective patients (RR 2.88; 95% CI 1.04–7.92).

Summary of the cholecystectomy-specific consent components for which the likelihood of being discussed with a patient was impacted by patient's gender, age group or ASA fitness grade, surgical setting, or mode of operation.
Discussion
Our primary aim was to evaluate the overall quality of consent for patients who were scheduled for conventional cholecystectomy but instead underwent STC. We found the informed consent procedure for such patients had been inadequate, where the majority of patients had not been informed of the possibility of undergoing STC before their gallbladder surgery. Only 14% of patients received Trust Clinical Governance Committee-approved patient information leaflets, although the importance of providing comprehensive verbal and written information to the cholecystectomy patients before obtaining their consent is well known.1,6 Many intraoperative risks, including severe cardiac disorders, infected bile, gallstone spillage, and diathermy-induced injuries, as well as alternative management options were rarely disclosed to patients. This finding is particularly concerning when considered in conjunction with previous research on the consent process for cholecystectomy. Cholecystectomy patients have reportedly found gathering information on the risks and benefits of all the available treatment options to be an important step in their development of confidence in the procedure. 14 Others' decisions to undergo cholecystectomy were influenced by an unquestioning trust in their surgeon to solve their health issue, and it is equally important that such patients' convictions are balanced by a full knowledge of the potential complications of the surgery. It is important to consider that patients are likely to be unaware of the specific limitations of their knowledge around the procedure. Bollschweiler et al. 15 found that 80% of cholecystectomy patients were satisfied with their consent procedure, but when assessed, less than half had a good knowledge of their disease, the possible alternatives to cholecystectomy, or the potential complications. The consenting clinician's role is, therefore, critical in providing all the components of information that may be of interest to a patient, without making assumptions about prior knowledge.
In this study, we explored the relationship between patient and procedure-specific factors and the quality of consent for cholecystectomy patients. We found demonstrable variation in the likelihood of single components of information being discussed, corresponding with a growing body of literature supporting the notion that patient–doctor relationships are affected by factors such as gender and age. Female patients have been shown to ask more questions during consultations than male patients, whereas doctors' approaches to communication also differs between male and female patients. 16 Doctor–patient communication is also altered for patients of different ages; clinicians are asked fewer questions by older patients and they elaborate less on the biomedical details of the condition than when faced with a younger patient. 17 Adding to this evidence, we found the provision of patient information leaflets varied greatly between different patient subgroups, favoring women over men and those aged <60 years over older patients. This finding is particularly concerning for older patients, who have been shown to have a lower health literacy than younger patients, to leave consultations having asked fewer questions, and to appreciate being given concise written information that they are able to refer to at a later time at home.17,18
We also found evidence that the surgical setting and operation mode impacted on the information given during the consent procedure. Nonelective patients were less likely to be informed about the risk of postoperative diarrhea, suggesting that clinicians perceive patients in emergency situations to be uninterested in less serious side effects. However, they were more likely to be warned of multiple severe complications, suggesting that consenting clinicians feel more comfortable disclosing the more alarming risks in this setting. We also found that patients who underwent laparoscopic STC were more likely to receive a patient information leaflet than those undergoing open surgery, although we acknowledge that patient information leaflets were also provided more frequently to women than men; the effect seen here may, therefore, be due to the significant correlation between the female and laparoscopic cohorts. However, a surprising finding was that consultations with laparoscopic patients were also more likely to include a discussion of the consultant's name, the consenting clinician's grade, and the intended benefits of the procedure. It is possible that with these patients who appear to be less complicated, more importance is given to ensuring that the administrative details are completed adequately. Each of these findings indicates an assumption on the behalf of the consenting clinician about the components of information that will be most important to the patient.
One limitation of the methodology used for the assessment of consent quality is that it relied on the retrospective analysis of generic consent forms, which may not accurately describe the quality of information that patients received. The authors consider it unlikely that the analysis of secondary evidence would cause bias by differentially affecting specific subgroups, but the findings of the study would be strengthened by further research using primary evidence such as video or audio recordings of consultations. 19 It is also important to acknowledge that there is a risk associated with analyzing a high number of variables, as the likelihood of detecting a statistically significant difference by chance increases. 20 We must, therefore, be careful how we interpret the findings of the effect of patient and procedural factors on the likelihood of individual components of information being discussed. However, given the strength of effect sizes seen for some components, and that there appeared to be trends where similar effects were seen for multiple components within the same category, it seems safe to conclude that consenting clinicians were influenced in some way by patient and procedural factors.
Our results suggest that consenting clinicians make certain assumptions regarding what the patient considers as important. During their medical education, clinicians adopt and develop skills of pattern recognition that are useful when diagnosing complex conditions and deciding on best management plans for patients.21,22 Paradoxically, this attitude could potentially fuel unhelpful stereotypes when it comes to consenting patients, with clinicians choosing to leave out information that they assume to be inconsequential. Although surgeons should be trained to recognize and reflect on such tendencies, the findings of this study highlight the potential usefulness of cholecystectomy-specific consent forms, including a comprehensive patient information leaflet, to improve the quality of the consent procedure. Their introduction to common surgical practice could mean that clinicians are provided with helpful prompts to aid the delivery of a more consistent range of information to all patients, regardless of patient demographics or clinical factors.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No author received any specific funding for this work.