
Abstract
Background:
The aim of this study was to evaluate 24-hour pH monitoring results before and after gastrostomy in neurological impaired (NI) children who underwent gastrostomy or Nissen fundoplication (NF) concurrently with gastrostomy.
Materials and Methods:
Between March and December 2018, NI patients who had previously received pre- and postgastrostomy (Group 1) or gastrostomy + NF (Group 2) underwent pH monitoring pre- and postoperatively.
Results:
Twenty patients [12 males (60%) and the median age of 5.6 (14 months–14.7 years) years] with NI were followed up during the study period. When pre- and postgastrostomy weight and BMI z-scores were compared, the results were significantly higher in both groups after procedure (P = .043, P = .040, respectively). The clinical results of the patients after the operation showed improvement in both groups. The pH index of Group 1 (n = 11) was 2.32 (0–3.8) before gastrostomy and 3.18 (2.1–6.9) after gastrostomy (P = .061) and in Group 2 (n = 9) it was 5.85 (4.9–15.8) and 0.61 (0.3–1.3), before and after procedure (P < .001). There was a statistically significant difference in reflux index of each group. This difference was not statistically significant between the groups (P = .072). When the total bolus exposure index was compared, it was 4.01 (2.1–5.2) before gastrostomy and 5.67 (4.6–6.3) after gastrostomy in Group 1 (P = .041). In group 2, that index was found to be 9.8 (8.3–10.2) before and 1.28 (0.5–1.4) after (P < .001). There was a statistically significant difference in index after gastrostomy in Groups 1 and 2 (P = .023).
Conclusions:
Gastrostomy feeding is an effective and safe option to achieve enteral feeding in NI children. NF concurrent with gastrostomy should be decided according to the individual patient. Clinical trials protocol registration ID number was PRS NCT 0445112.
Introduction
Gastrointestinal (GI) problems causing malnutrition may develop quite frequently in patients with neuromotor developmental delay. Impairment of the brain may result in significant dysfunction in the GI tract. Oro-motor disabilities, swallowing in-coordination, abnormal esophageal motility, and gastroesophageal reflux (GER) are the most common problems of these children. 1 Especially GER is the more common problem in neurologically disabled children and referred as gastroesophageal reflux disease (GERD) when it causes symptoms and/or complications. 2
Recurrent episodes of GER can lead to overt or silent aspiration, vomiting, spillage, food aversion, prolonged feeding times, and may result in a significant reduction of nutrient and energy intake. 3 In these patients where oral intake is insufficient or impossible, the development of a child is adversely affected to a significant extent.
Initially, feeding through the nasogastric tube (NG) is used frequently but it may bring along various problems in the long term. Therefore, there is a need for more ideal feeding methods that can replace NG in patients with long-term enteral feeding requirement.4,5 Gastrostomy is often the preferred method for this purpose. Gastrostomy can be performed with open surgery, laparoscopic gastrectomy, or percutaneous endoscopic gastrostomy (PEG).
Diagnosis of GERD in patients with neurological impairment (NI) might be more difficult because of the absence of characteristic features in many cases. One of the best methods for the diagnosis of GER is the 24-hour esophageal pH monitoring. 6
Antireflux surgery should be performed concomitantly with gastrostomy in patients with NI who have reflux detected by pH monitoring along with reflux-related GI and non-GI symptoms. The Laparoscopic Nissen fundoplication (LNF) became the gold standard for antireflux surgery.5,7,8 Although there are some statements in the literature advocating that GER may develop in the late period in patients undergoing only gastrostomy, there are also reports supporting that gastrostomy does not contribute to the development of reflux.9–13 Regardless of whether the patient received antireflux surgery or not, long-term follow-up is necessary in patients feeding with gastrostomy.9–13
The aim of this study was to compare the results of pre- and postoperative 24-hour pH monitoring in patients who underwent gastrostomy only and who underwent fundoplication concurrently with gastrostomy and to evaluate influence of gastrostomy/LNF + gastrostomy on GER.
Materials and Methods
Study design
The study was conducted prospectively on children with gastrostomy between March and December of 2018 in the Department of Pediatric Gastroenterology Hepatology and Nutrition, Ondokuz Mayis University Medical Faculty. All patients underwent 24-hour pH monitoring before gastrostomy was applied. The patients were divided into two groups. Group 1 consisted of patients undergoing gastrostomy only, whereas Group 2 consisted of patients undergoing fundoplication procedure concurrently with gastrostomy.
The gastrostomy method was PEG in all patients who underwent gastrostomy alone. The PEG catheter was placed in the fundus of the stomach in the lower region with the endoscope so as not to affect the angle of His. LNF and laparoscopic gastrostomy were performed in all patients who underwent simultaneous antireflux surgery. Antireflux surgery decision was made according to the clinical status of the patients (growth retardation, recurrent aspiration pneumonia, and recurrent vomiting unresponsive to medical treatment), findings compatible with reflux in 24-hour pH monitoring.
Patients' age, sex, and primary diseases, preoperative height (in case of possibility) and weight measurements, preoperative contrast-enhanced imaging, and 24-hour pH monitoring results were recorded. Postoperative height and weight measurements and 24-hour pH monitoring were performed for patients throughout the study. Anthropometric measurements were taken including body weight and height. Percentiles and Z scores of weight, height, and body mass index (BMI) were calculated using WHO Anthroplus v 1.0.4 software. 14 Patients with BMI < −2 Z-score were considered children with malnutrition.
Twenty-four-hour pH monitoring
Twenty-four-hour esophageal pH monitoring was conducted using an ambulatory system (Ohmega, MMS, Enschede, the Netherlands). This system consists of a portable data logger (MMS Investigation and Diagnostic Software®) and a disposable catheter that contains two pH electrodes (Unisensor, Attikon, Switzerland).
Before recording, the pH electrode was calibrated in the special buffer solutions at pH values of 1 and 2. The catheter was placed transnasally and the pH sensor was situated 2–3 cm above the lower esophageal sphincter, as calculated by the Strobel formula (0.252 × body length [cm] + 5), and then confirmed by X-ray. Patients were asked not to use antireflux medications for at least 3 days before the procedure. All the children were admitted to our inpatient unit on the day of the procedure and discharged the following day. During the monitoring period, patients were permitted to continue daily activities and oral or enteral intake of anything except acidic foods. Caregivers were asked to press the labeled buttons and complete a diary recording at the same time for the meals and body position. Twenty-four-hour esophageal pH monitoring was analyzed using MMS software and manually reviewed by the same investigator (F.D.).
pH reflux index (RI) is the percentage of time with esophageal pH <4. Reflux index >4% was accepted as a positive test result for pH monitoring. Total bolus exposure index is the percentage of time that a bolus is present in the esophagus. 6
The study was approved by the Ethics Committee of Ondokuz Mayis University (Decision no: 2019/192).
Statistical analysis
Statistical analyses were performed using SPSS v. 22.0 software (Statistical Package for Social Sciences, Inc.). Power analysis revealed that at least 9 patients were required for each group. The Mann–Whitney U-test was used to compare two groups. Comparison of continuous variables was performed using the Wilcoxon's matched-pairs signed-rank test. A value of P < .05 was considered statistically significant.
Results
Twenty patients who were followed-up with gastrostomy between March 2018 and December 2018 were included in the study. All patients had severe Class IV neurological deficiency according to the Gross Motor Function Classification System (GMFCSR). Two patients had shunt owing to hydrocephalus, one patient had Rett syndrome, one Bartter type 5, one CHARGE syndrome, one Pompe disease, one subacute sclerosing panencephalitis, and the other patients had epilepsy. Of the 20 patients included in the study, 12 (60%) were male and 8 (40%) were female. Their median age was 5.60 years (14 months–14.7 years). Preoperative contrast (barium) graphy was performed in 14 (70%) patients and reflux was detected in 35% of these patients. No additional pathology was observed on barium radiographs. All patients underwent 24-hour esophageal pH monitoring before the gastrostomy procedure.
There were 11 (55%) patients in Group 1, 7 (63.6%) were male and the median age was 4.7 years (14 months–11 years) and PEG was applied to these patients. In Group 2, there were 9 (45%) patients, 5 (63.6%) were male and the median age was 5.3 (2.1–14.7) (Table 1) and these patients underwent LNF concomitantly with gastrostomy. There were no procedure-related complications in the patients. The postoperative 24-hour pH monitoring and simultaneous height and weight measurements were performed on average of 16.5 months (6–24) after gastrostomy.
Comparison of Demographic Findings of Neurologically Impaired Children
Comparison of pre- and postoperative in the same group (Wilcoxon test).
Comparison of PEG and gastrostomy + NF (Mann–Whitney U-test).
Italics indicate statistically significant values (p < 0.05).
PEG, percutaneous endoscopic gastrostomy.
The median BMI Z-score of the patients in Group 1 before gastrostomy was −0.69 (−1.8 to 1.3) and the same measurement after gastrostomy was −0.38 (−1.1 to 1.6). The median BMI Z-scores of the patients in Group 2 was −0.74 (−2.1 to 1.4) before gastrostomy and −0.10 (−1.9 to 1.6) after the procedure (Table 1).
Statistically significant difference was observed between BMI Z-scores in patients after gastrostomy (P = .040) but no statistically significant difference was found in BMI Z-scores between Groups 1 and 2 (P = .554) (Table 1). The clinical results of the patients after the operation showed improvement in both groups (Table 2).
Comparison of Before and After Clinical Findings of Neurologically Impaired Children
In 24-hour pH monitoring, the median pH index was 2.32 (0–3.8) before gastrostomy and 3.18 (2.1–6.9) after gastrostomy in Group 1 (P = .061). In Group 2, the median value of pH index before procedure was 5.85 (4.9–15.8), and 0.61 (0.3–1.9) after procedure (P < .001). This difference was not statistically significant between the groups (P = .072) (Fig. 1).
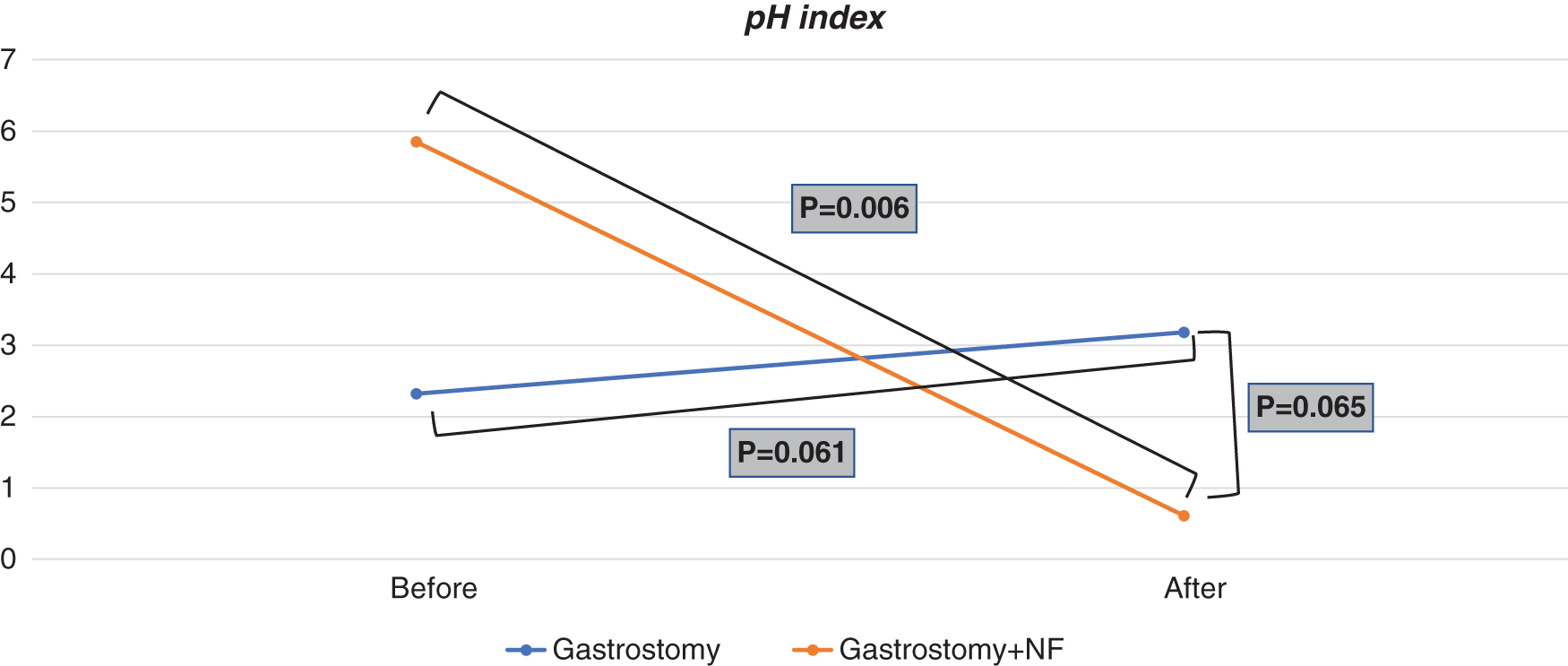
Evaluation of pH index of patients before and after the procedure.
When the total bolus exposure index was compared, it was 4.01 (2.1–5.2) before gastrostomy and 5.67 (4.6–6.3) after gastrostomy in Group 1 (P = .041). In Group 2, that index was found to be 9.8 (8.3–10.2) before procedure and 1.28 (0.5–1.4) after procedure (P < .001). There was a statistically significant difference in total bolus exposure after gastrostomy in Groups 1 and 2 (P = .023). Total bolus exposure index was significantly lower in Group 2 than in Group 1 (Fig. 2).

Evaluation of total bolus exposure index (%) of patients before and after the procedure.
Patients' lowest pH value, number of reflux episodes >5 minutes and the longest reflux episode before and after gastrostomy measurements are given in Table 3.
Comparison of pH Measurements of Neurologically Impaired Children
Comparison of pre- and postoperative in the same group (Wilcoxon test).
Comparison of PEG and gastrectomy + NF (Mann–Whitney U-test).
Italics indicate statistically significant values (p < 0.05).
Discussion
This study is the first in this field to compare the 24-hour pH measurement before and after gastrostomy in neurological impaired children who underwent gastrostomy and gastrectomy + NF as a method of reflux procedure. GI problems that cause malnutrition such as swallowing disorder, GER, vomiting, delayed gastric emptying may develop quite frequently in NI patients. Nutritional problems that frequently develop in NI children have an important place in the care and treatment of these children. The degree of malnutrition is directly related to the duration and severity of the neurological disease. 15 The cause of malnutrition in these patients may be malnutrition and/or reflux-related GI or non-GI symptoms owing to oral motor dysfunction and metabolic changes.
In this study, we found a significant increase in BMI Z-scores after gastrostomy in both groups. Dahlseng et al. 16 found that 33% of 1295 NI patients were fed with gastrostomy in six different European countries and their feeding was significantly improved compared with patients who were not intubated for feeding. In our group of patients with severe swallowing disorder owing to oral motor dysfunction, tube feeding provided both adequate and safer feeding. Tube feeding after gastrostomy contributed to appropriate caloric intake, which revealed a significant increase in BMI Z-score.
Gastrostomy was applied to 55% patients and after gastrostomy indication in NI patients all were evaluated for GERD (clinical findings, history of recurrent aspiration and anatomical evaluation with esophageal gastric duodenum X-ray and reflux evaluation with 24-hour pH monitoring).
GERD is an important problem in these patients as much as feeding difficulty. Diagnosis of GER may be more difficult in children with neurological damage because these children may not present the characteristic features of the disease. A high frequency of GER in NI children (15–78%) led some centers to endorse gastrostomy and NF as a routine treatment. 17 Although the experience of endoscopic and laparoscopic gastrostomy has increased considerably, the relationship between gastrostomy and GER is still controversial. 18 Some authors argue that routine antireflux surgery should be added, whereas others suggested that antireflux surgery had complications and a low success rate in these patients and therefore recommends only gastrostomy.19–21 We believe that in case of antireflux surgery indication, it should be determined according to the condition of the individual patient.
Laparoscopic gastrostomy and simultaneous NF are now accepted as the gold standard surgical procedure for children with refractory GERD. We use PEG as the gastrostomy method in our clinic because it is minimally invasive, easy to perform, and allows early feeding. If the pathological reflux in the 24-hour pH monitoring is detected in a patient with GI and non-GI complications because of GERD, NF with gastrostomy is the preferable choice of surgery in our clinics. Most children with NI may have extremity deformities and respiratory problems. We prefer the laparoscopic method because it not only shortens the duration of surgery but also provides the opportunity to work on a much better field of vision.
Although actual experience with endoscopic or laparoscopic gastrostomy has increased considerably, the relationship between gastrostomy and GER is still controversial. There are authors arguing that gastrostomy increases GER, but some are vindicating that it has no effect on the reflux.19–21 In this study, there was a difference between reflux index before and after gastrostomy in both groups. After gastrostomy, pH index decreased significantly in both groups. No significant difference was found between the groups in terms of pH index after gastrostomy. When the total bolus exposure index was evaluated, the duration of reflux was found to be significantly shorter in the group that received NF, but this difference did not raise a pathological GER finding in the group that received gastrostomy.
Thomson et al. 22 evaluated 10 NI children before and after gastrostomy with multiple intraluminal impedance and reported the rate of reflux affecting up to the proximal esophagus as 56% before gastrostomy compared with 82% after gastrostomy. In the study by Burd et al., 23 clinical history and preoperative radiological evaluation and pH studies were normal, but the authors reported that GER could develop in NI children after gastrostomy because of anatomical alterations and changes in the type and volume of postsurgical feeding. In the study of Kawahara et al., 12 there was a significant increase in the degree of esophageal acid exposure after gastrostomy in the nonreflux group in the 24-hour pH meter assessment performed before and after the procedure, but this was largely controllable by medical treatment.
The authors suggested that the anatomical changes caused by stomach sticking to the abdominal wall after gastrostomy may affect gastric emptying and this may occur as a result of laying the groundwork for reflux. Although there was an increase in total reflux time after the procedure in our group of patients who had only gastrostomy, medical treatment was not administered because there was no GER finding. We believe that preserving the natural anatomy by means of endoscopic catheter placement from the large curvature inferior of the stomach and taking care to preserve the sensation angle in the group that received gastrostomy only is reflected in our results.
In the study of Fukahori et al., 24 in 2016, which evaluated esophageal motility before and after laparoscopic NF in NI children with GER by means of combined multichannel intraluminal impedance pH meters, significant reduction was observed in the pH and bolus exposure indices after fundoplication. Similar to our study in NI patients, many studies19,24 examining the relationship between gastrostomy and GER observed that the incidence of GER did not increase after gastrostomy, and that GER could even be reduced with improved nutritional status and weight gain experienced by the patient.
There are some limitations in this study. The limited number of patients and the detection of acidic reflux by 24-hour pH measurement without assessment of alkaline reflux were the disadvantages of this study.
Conclusion
In conclusion, gastrostomy alone or in combination with antireflux surgery improves clinical parameters along with the quality of life and increases family satisfaction in children with neurological damage suffering from swallowing disorders. Patients who had GERD symptoms should be evaluated for reflux before the procedure. Although gastrostomy alone does not increase the incidence of reflux and does not adversely affect the clinical and growth parameters of the patients, LNF should be reserved for patients with the presence of GER. For prophylactic concomitant fundoplication to be worthwhile, LNF with gastrostomy must demonstrate acceptable comparable risks to gastrostomy-only surgery. New studies are needed in this field.
Informed Consent
Informed consent was obtained from all individual participants included in the study. Written informed consent was obtained from all individual participants included in the study and their parents (or legal guardians). All procedures performed involving human participants were in accordance with the ethical standards of the local ethics committee and with the 1964 Declaration of Helsinki and its later amendments.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors. The study was approved by the Ethics Committee of Ondokuz Mayis University (OMU KAEK decision number 2019/192).
Footnotes
Authors' Contribution
All authors contributed to the research. Study conception and design: F.D., G.C.; Acquisition of data: F.D.; Analysis and interpretation of data: F.D.; Drafting of article: F.D., B.D.D., H.A., G.C.; Critical revision: F.R.B., A.G.K.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.