
Abstract
Background:
Achalasia may occasionally occur among women of childbearing age. Pregnancy may lead to deterioration of the disease and negatively affect maternal and perinatal outcomes. However, the impact of peroral endoscopic myotomy (POEM) on reproductive outcomes has been understudied.
Methods:
A retrospective study on prospectively maintained database, including women aged 18–45 who underwent POEM during 2012–2017 at a university hospital.
Results:
During the study period, POEM was performed in 86 patients. Of them, 23 were women of childbearing age (median age 31.9 [26.0–40.7] years). Follow-up data were available for a median of 24 [16–41] months. Treatment success (Eckardt score <3) was achieved in 22 (95.7%) women. Six (26.1%) women reported attempting to conceive after POEM. Overall, 7 post-POEM pregnancies among 5 women were encountered. All 7 pregnancies were naturally conceived with a median surgery-to-conception interval of 16 [10–21] months. The median gestational weight gain was 10 kg, and was insufficient in all pregnancies. None of the women was hospitalized during the index gestation. All pregnancies resulted in term live-birth vaginal delivery. The median neonatal birthweight was 2940 g, with only one case of a small-for-gestational age infant. Achalasia-related symptoms recurred during 2 pregnancies, with resolution following delivery.
Conclusions:
Pregnancy after POEM for the treatment of achalasia was associated with favorable maternal and perinatal outcomes. This data should reassure women who wish to conceive following peroral myotomy.
Introduction
Achalasia is a rare esophageal motility disorder characterized by inadequate relaxation of the lower esophageal sphincter (LES) and ineffective esophageal peristalsis. Its reported incidence is 1–3 cases per 100,000/year with an equal sex preponderance1,2; an initial peak in the incidence of achalasia occurs between 17 and 30 years of age, whereas a second peak is encountered in the fifth and sixth decades of life.1–3 As such, achalasia may occasionally occur among women of childbearing age.
Little is known regarding reproductive outcomes among women with achalasia, as most data are derived from small case series and scattered case reports.4,5 Based on the aforementioned publications, it has been reported that women with achalasia who conceive are likely to experience deterioration in their health condition which may adversely affect maternal and perinatal outcomes.4,5
Treatment of achalasia is a challenging issue, as medical treatment is mostly ineffective, interventional strategies are commonly utilized. While the gold standard surgical treatment for achalasia is laparoscopic Heller myotomy, it is gradually being replaced by a less invasive technique, peroral endoscopic myotomy (POEM). Since its introduction in 2008, 6 POEM, an endoluminal procedure, avoids laparoscopy and unnecessary dissection, providing an efficient procedure with low rates of operative complications.7,8 However, data are limited regarding reproductive outcomes of women following POEM. Given the paucity of literature, we aimed to report our single-center experience with POEM among women of childbearing age and its related reproductive outcomes.
Patients and Methods
Patients
We performed a review of our prospectively maintained database of patients who underwent POEM at the Hadassah–Hebrew University Medical Center in Jerusalem, Israel during 2012–2017 to identify women of childbearing age (defined as 18 to 45 years). Perioperative investigations included complete history and physical examinations, upper gastrointestinal (GI) endoscopy, high-resolution manometry (HRM, Chicago classification v3.0 was used for the diagnosis of achalasia 9 ), and barium swallow study. All women had symptomatic achalasia before surgery.
Surgical procedure
All POEM procedures were performed using a standardized technique. In brief, following general anesthesia with endotracheal intubation in a supine position, an upper GI endoscopy is performed. The esophagus is cleaned to remove all food residues and measurement of esophagogastric junction (EGJ) location is made. A mucosal lift is performed 10 cm proximal to the EGJ and a 15 mm incision of the mucosa is performed. The endoscope is inserted through the mucosal incision into the submucosal space and a submucosal tunnel is created on the anterior part of the esophagus extending to 2 cm distal to the EGJ. At this stage, myotomy is performed, including the circular muscle layer, leaving the longitudinal muscle layer intact. The length of the myotomy is tailored specifically to the patients' disease, but generally an 8 cm myotomy is performed extending from 6 cm proximal and 2 cm distal, to the EGJ. After verification of an open LES looking from the true lumen of the esophagus, the mucosal incision is closed using endoclips. On postoperative day 1, all patients underwent an esophagogram to exclude a leak, followed by the introduction of clear liquid diet and advancement of diet over a number of days. All operations were performed by the same team.
Data collection
We obtained approval from the Institutional Review Board for this study from the Ethics Committee of the Hadassah Medical Center on December 2017 (HMO-0684-17). Data for all patients who underwent POEM were maintained in a prospective database in a real-time manner. Achalasia-related symptoms were evaluated throughout the pre- and postoperative period using the Eckardt score, a well-established tool in this subset of patients, allowing quantification of the severity of symptoms (consisting of dysphagia [0–3], chest pain [0–3], regurgitation [0–3], and weight loss [0–3]; total score varies between 0 and 12) 10 (Supplementary Table S1). For the purpose of this study, the following data were extracted: demographic characteristics, anthropometric parameters, preoperative information (duration of disease, prior achalasia-related interventions, gravidity, parity, manometry results, and Eckardt score), and postoperative data (manometry results, current weight, Eckardt score, reflux symptoms, satisfaction from surgery, and attempts at becoming pregnant). In addition, for those who conceived following surgery, pregnancy characteristics (surgery-to-conception time interval, hospitalization throughout gestation, gestational weight gain, pregnancy-associated hypertensive disorders, gestational diabetes mellitus [GDM], and predelivery Eckardt score) and delivery data (gestational age [GA] at delivery, mode of delivery, and neonatal birthweight) were retrieved. Reflux symptoms were reported as occurring every meal, daily, occasionally, or none. Clinical success was defined as a reduction in the postoperative Eckardt score by 4 points from baseline or a score of less than 3. 11 The degree of gestational weight gain was defined as insufficient, appropriate, or excessive according to the Institute of Medicine (IOM) recommendations, based on women's pregestational body mass index (Supplementary Table S2). 12 GA was based on ultrasonography performed during the first trimester. Preterm delivery was defined as GA <37 completed weeks. Small-for gestational-age (SGA) was defined as <10th percentile, using birth weight z-scores calculated with the formulas published by Dollberg et al. on a similar population in Israel, adjusting for GA and the offspring's sex. 13
Statistical analysis
Data are described as proportions for categorical variables, and as medians and interquartile ranges for continuous variables without a normal distribution. The data were analyzed using Software Package for Statistics and Simulation (IBM SPSS version 24; IBM Corp., Armonk, NY).
Results
During the study period, POEM was performed in 86 patients. Of them, 23 (26.7%) were women of childbearing age and constituted the study group. A flowchart of the establishment of the study cohort is shown in Figure 1.
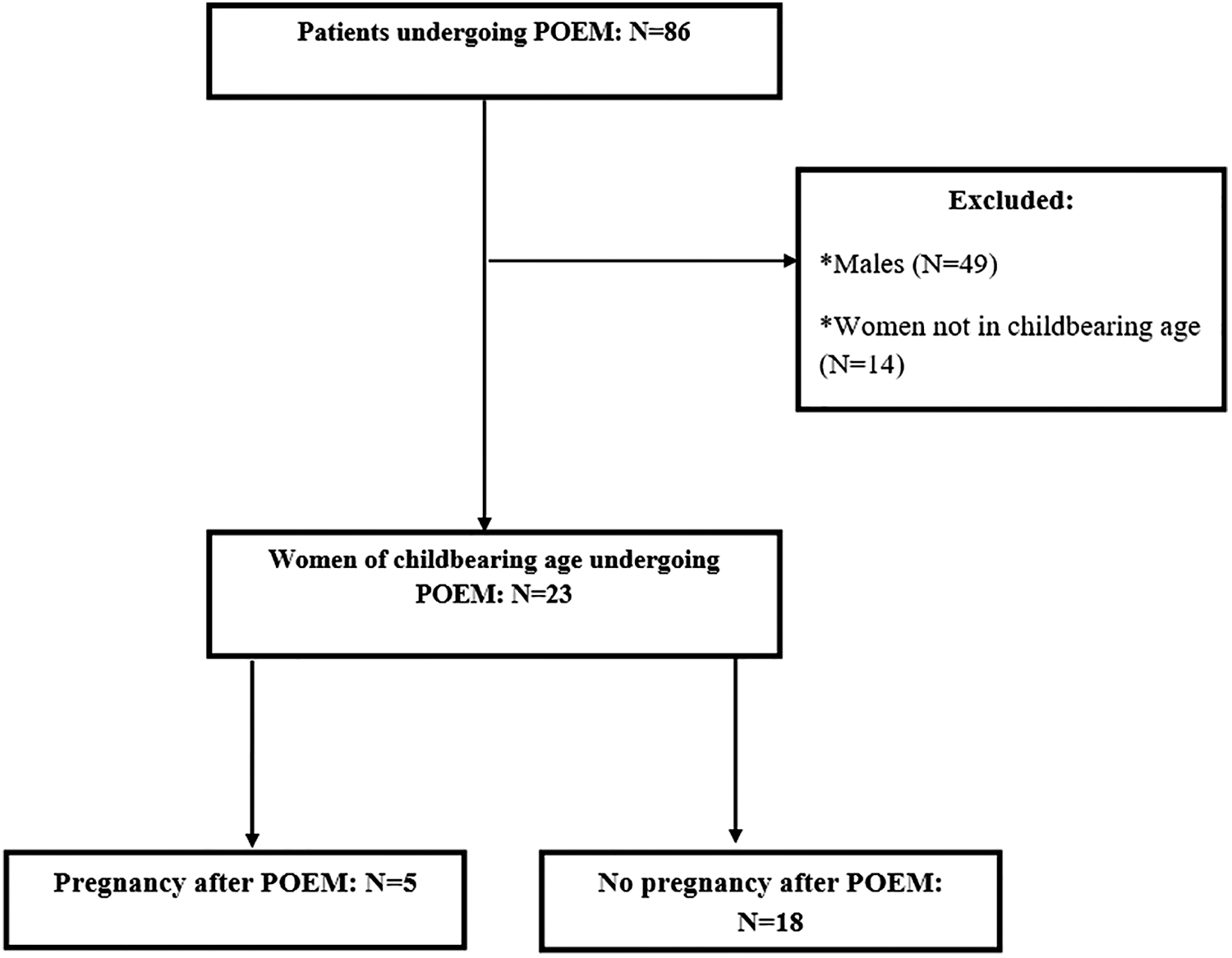
Schematic flowchart of patient inclusion in the study.
Baseline characteristics of the study group are shown in Table 1. The median age of the study group at the time of surgery was 31.9 [26.0–40.7] years; 6 (26.1%) were nulliparous. Median duration of achalasia up to the time of POEM was 2 [1–5] years and the preoperative Eckardt score was 9.5 [8.8–10.3] points. The most common type of achalasia was type 2 (n = 19), followed by type 1 (n = 3) and type 3 (n = 1).
Baseline Characteristics of Reproductive-Aged Women Undergoing Peroral Endoscopic Myotomy
All continuous variables are expressed as median [interquartile range] (mean).
BMI, body mass index; IRP, integrated relaxation pressure; LES, lower esophageal sphincter.
Data regarding women's outcomes are described in Table 2. Follow-up data were available for a median of 24 [16–41] months. At the end of follow-up, treatment clinical success (Eckardt score <3 or a reduction in Eckardt score by 4 points from baseline) was achieved in 22 (95.7%) women. Three-month postoperative HRM studies demonstrated significant decreases in both LES basal pressure and integrated relaxation pressure.
Long-Term Follow-Up Data of Reproductive-Aged Women Undergoing Peroral Endoscopic Myotomy
All continuous variables are expressed as median [interquartile range] (mean). The Mann–Whitney U test, a nonparametric test was used for continuous variables without a normal distribution.
Statistically significant compared to preoperative status.
On a scale from 0 (lowest satisfaction) to 10 (highest satisfaction).
BMI, body mass index; IRP, integrated relaxation pressure; LES, lower esophageal sphincter; POEM, peroral endoscopic myotomy.
Six (26.1%) women reported attempting to conceive after POEM. Overall, 7 post-POEM pregnancies among 5 women were encountered during the follow-up period. All 7 pregnancies were naturally conceived. The median surgery-to-conception interval was 16 [10–21] months. Pregnancy-related hypertensive disorders did not occur in any of the pregnancies, while GDM was diagnosed in 1 woman. The median gestational weight gain was 10 kg, and was insufficient in all pregnancies. None of the women was hospitalized during the index gestation. Occasional reflux symptoms were present in 3 (42.9%) pregnancies. The appearance of achalasia-related symptoms (Eckardt score >3) was reported in 2 pregnancies of the same patient, with resolution following pregnancy. All pregnancies ended in live-birth following unassisted vaginal delivery. The median GA at delivery was 39 [38–40] weeks with no preterm deliveries. The median neonatal birthweight was 2940 [2750–3300] g, with only one case of a SGA infant. Detailed description of pregnancy and delivery outcomes is shown in Table 3. Reflux symptoms at the end of follow-up were reported to occur at least occasionally in 8 (34.8%) women of the entire cohort.
Detailed Description of Pregnancy and Delivery Characteristics and Outcomes
BMI, body mass index; GA, gestational age; GDM, gestational diabetes mellitus; GWG, gestational weight gain; Preop, preoperative; SGA, small-for gestational-age.
Discussion
This study aimed to investigate the outcomes of reproductive-aged women undergoing POEM. POEM was shown to be highly effective in terms of achalasia-related symptoms. Almost one-fourth of women became pregnant after surgery, with overall favorable maternal and neonatal outcomes, and relatively low rate of aggravation in achalasia symptoms.
Since food intake is heavily impaired in most patients with achalasia, a potential negative influence on both the mother and the growing fetus may take place during pregnancy.4,5 Based on small case series, pregnancy among women with achalasia has been associated with serious adverse outcomes, including preterm delivery, fetal growth restriction, perinatal death, and maternal mortality.4,5 Moreover, the increased intra-abdominal pressure and elevation of the diaphragm throughout gestation may further worsen achalasia symptoms. 4 As such, appropriate preconception therapeutic intervention among women with achalasia who wish to conceive may be beneficial. 4 While there are multiple options for the treatment of achalasia, including botulinum toxin injection and pneumatic dilatation, the gold standard remains surgical myotomy. 14 In the past several years POEM has become increasingly more popular as a viable alternative to traditional surgical myotomy. Although not without risks, there are many inherent benefits with POEM, including its minimal invasive nature, lower risk of procedure-related infection, lack of postoperative hernias, and the ability to treat those in whom a longer myotomy is required. 15
Since its introduction over a decade ago, POEM has evolved from a novel concept to a mainstream treatment strategy for patients with achalasia with a reported success rate of over 90%, leading to a major shift in achalasia therapeutics.16–18 The success rate of POEM in the current cohort of reproductive-aged women concurs with these previous publications, with over 95% success rate, a similar rate to that found in our entire cohort of POEM patients. 19 In addition, 6 women representing over one-fourth of the study cohort reported attempted to conceive after POEM. All but 1 woman successfully became pregnant during study period. This is in line with previous reports showing that achalasia does not seem to negatively affect fertility. 4 Furthermore, the course of pregnancy and delivery was favorable in terms of maternal and perinatal outcomes, with no preterm births encountered and only a single case of a SGA infant. Finally, the rate of deterioration in achalasia-related symptoms was low compared with prior publications,4,5 and no medical or interventional treatment was needed throughout pregnancy in this regard. These data, together with prior studies regarding the safety and efficacy profile of POEM, should reassure women of childbearing age who wish to conceive following surgery.
One of the most prominent concerns with regard to POEM involves the occurrence of postoperative gastroesophageal reflux disease (GERD). Indeed, in the current cohort, one-third of women reported to at least occasionally suffer from heartburn. Throughout the 7 post-POEM pregnancies encountered, reflux symptoms were common. It is possible that while the high progesterone level associated with pregnancy coupled with the increased intra-abdominal pressure may potentially aggravate GERD symptoms. 4 Nevertheless, these symptoms, which are encountered in 40%–85% of normal gestations, 20 tended to resolve following delivery.
Some questions remain unanswered. The optimal timing of pregnancy following POEM, with regard to maternal and perinatal outcomes, remains not well established. It is possible that avoiding pregnancy in the first months after surgery may be preferable. Another area of uncertainty is the proper degree of gestational weight gain after POEM. Applying the IOM pregnancy weight gain guidelines to our cohort showed inadequate weight gain in all cases. As gestational weight gain may be an important determinant of fetal growth,21,22 whether specific recommendations should be used in this subset of women remains to be further elucidated. Future studies are needed to elucidate these unsettled important issues.
Study limitations
Our study has several caveats. First, despite the novelty of the current report, the sample size was modest, limiting the ability to draw firm conclusions. Second, the conduct of the study in a single tertiary care center may further hamper the generalizability of the results. In addition, as we did not use a validated questionnaire to evaluate reflux symptoms, it may have hampered our ability to properly assess their occurrence during study period. Despite these limitations, as this is the first report, to the best of our knowledge, to investigate the reproductive outcomes, including the course of pregnancy following POEM, we believe that it represents a valuable contribution to the current literature.
Conclusions
In the current study evaluating the outcomes of POEM among reproductive-aged women, POEM was shown to be an effective treatment for achalasia. A substantial portion of women attempted becoming pregnant after surgery. Among the 7 pregnancies encountered in the current cohort, maternal and perinatal outcomes were generally favorable. Recurrence of achalasia-related symptoms occurred in the minority of women during pregnancy. Further prospective studies are warranted, to confirm our findings and better delineate reproductive outcomes among women of childbearing age undergoing POEM to improve the perioperative and preconception counseling, as well as antepartum care.
Authors' Contributions
Study Design, data acquisition, and data interpretation: A.R., R.B., and Y.M.; Drafting the article: A.R., R.B.; Treated the patients: A.R., R.B., Y.M., A.B., G.M., and H.J. Final approval: A.R., R.B., Y.M., A.B., G.M., and H.J.
Consent
Institutional Review Board approval was obtained for this study.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.