
Abstract
Background:
Laparoscopic surgery is a choice of treatment for liver diseases; it can decrease postoperative morbidity and length of hospital stay (LOS). Hepatocellular carcinoma (HCC) in patients with cirrhosis and portal hypertension may benefit from minimally invasive liver resections (MILRs) instead of open liver resections (OLRs). Whether minimally invasive approaches are superior to conventional ones is still a matter of debate. We thus aimed to gather the available literature on this specific topic to achieve greater clarity.
Materials and Methods:
PubMed, EMBASE and Web of Sciences databases were assessed for studies comparing OLRs versus MILRs for HCC in cirrhotic patients up to February 2020. Data from our surgical experience from June 2010 to February 2020 were also included. Demographic characteristics, liver function, the presence of portal hypertension, tumor number, and tumor size and location were assessed; operative time, need for Pringle maneuver, estimated blood loss (EBL), major or minor hepatectomy performance, and conversion rate were evaluated for operative findings. Postoperative outcomes and liver-related complications, surgical site infection (SSI) rate, blood transfusion (BT) rate, need for reintervention, LOS, in-hospital or 30-day mortality, and radicality of resection were also considered. Meta-analysis was performed employing Review Manager 5.3 software.
Results:
One thousand three hundred twenty-one patients from 13 studies and our own series were considered in the meta-analysis. At preoperative settings, the OLR and MILR groups differed significantly only by tumor size (4.4 versus 3.0, P = .006). Laparoscopic procedures resulted significantly faster (120.32–330 minutes versus 146.8–342.75 minutes, P = .002) and with lower EBL than open ones (88–483 mL versus 200–580 mL, P < .00001), thus requiring less BTs (7.9% versus 13.2%, P = .02). In terms of overall morbidity, minimally invasive surgeries resulted significantly favorable (19.32% versus 38.04%, P < .00001), as well as for ascites (2.7% versus 12.9% P < .00001), postoperative liver failure (7.51% versus 13.61% P = .009), and SSI (1.8% versus 5.42%, P = .002). Accordingly, patients who had undergone MILRs had significantly shorter postoperative hospitalization than patients who underwent conventional open surgery (2.4–36 days versus 4.2–19 days P < .00001). Both groups did not differ in terms of mortality rate and radicality of resection (OLR 93.8% versus 96.1% laparoscopic liver resection, P = .12).
Conclusions:
Based on the available evidence in the literature, laparoscopic resections rather than open liver ones for HCC surgery in cirrhotic patients seem to reduce postoperative overall morbidity, liver-specific complications, and LOS. The lack of randomized studies on this topic precludes the possibility of achieving defining statements.
Introduction
Hepatocellular carcinoma (HCC) is the most frequent primary liver malignancy with a definite higher incidence in cirrhotics. 1 Several curative treatment options are now available, and among these, liver resections are considered among the therapeutic ones.2–8 The first laparoscopic liver resection (LLR) for HCC was reported about 25 years ago. 9 Since then, several authors have attempted to compare minimally invasive approaches with conventional open liver resections (OLRs).10–14 Patients with cirrhosis associated or not with portal hypertension have been historically recognized as having increased perioperative risks and morbidity compared to healthy people, in proportion to the severity of their liver disease.15,16 LLR seemed to be able to minimize the high rates of postoperative complications in patients affected by chronic liver disease.17–23 Whether the outcomes after minimally invasive liver resection (MILR) are superior to OLR is still unclear and has been at the center of debate in the last decade. Accordingly, we aimed to assess the advantages of laparoscopic surgery in cirrhotic patients by gathering the available literature on this topic and reporting results of our personal experience. Eventually, all data were collectively reviewed in a global meta-analysis.
Materials and Methods
The literature search was guided by PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) 24 recommendations to identify scientific articles comparing laparoscopic and open liver resections for HCC in cirrhotic patients. Data for the meta-analysis were extrapolated from the included studies following the itemized pre-established pattern. Two authors (D.C. and C.D.P.) performed an independent literature search work up to February 2020. The PubMed/MEDLINE, EMBASE, and Web of Science electronic databases 25 were searched using a combination of the following medical subject headings (MESH): “laparoscopic liver surgery,” “laparoscopic liver resection,” “robotic liver resection,” “cirrhosis,” “portal hypertension,” and “hepatocellular carcinoma.” All articles dealing with the comparison between laparoscopic and open approaches were considered eligible. Full-text articles considered for inclusion were appraised and the relative references were hand-searched for additional suitable studies. Retrieved studies were included in the analysis if they were in English; they present a comparison between laparoscopic versus open liver resection; adult patients with cirrhosis were enrolled; and it was surgery for HCC. Studies without detailed data for subgroup of cirrhotic patients were thus excluded. Another author (C.P.) extrapolated data from the included studies for a meta-analysis. Eventual disagreements concerning inclusion were resolved by consensus among the authors.
Data from our prospectively collected database from June 2010 to February 2020 were also retrospectively analyzed (G.L.G. and V.D.P.). Twenty-seven cirrhotic patients who had undergone MILRs (20 pure laparoscopic and 7 robot assisted) with a diagnosis of HCC were assembled for the analysis. To make the comparison between balanced groups, 27 patients who had undergone OLR were case matched one-to-one by age, sex, tumor number, tumor size and location, and portal hypertension. 26 The presence of portal hypertension was defined according to indirect signs as the presence of esophageal varices and splenomegaly associated or not was thrombocytopenia.27,28
According to the predeveloped patterns, groups were compared on the following: preoperative characteristics such as age, body mass index (BMI), number of patients in each group, Child-Pugh score,29,30 the presence of portal hypertension, indocyanine green retention rate at 15 minutes (ICG-R15), 31 model for end-stage liver disease (MELD) Score, 32 barcelona clinic liver cancer (BCLC) staging, 33 tumor number, and tumor size and location according to the Brisbane classification 34 ; operative findings like operative time, need for Pringle maneuver, estimated blood loss (EBL), major or minor hepatectomy performance, and conversion rate; and postoperative outcomes, particularly, complications according to Clavien-Dindo (CD) classification, 35 ascites, bile leakage, postoperative liver failure (POLF), surgical site infection (SSI) rate, blood transfusion (BT) rate, need for reintervention, length of hospital stay (LOS) and in-hospital or at 30-day mortality, and radicality of resection. Data of our personal experience according to the pre-established patterns were included in the meta-analysis.
Statistical analysis
We report data in descriptive statistics. The SPSS v20.00 (SPSS, Inc., Chicago, IL), Fisher-test, and unpaired t-test were used when needed. Meta-analysis was performed by employing Review Manager 5.3 software (Cochrane Collaboration, Oxford, England) with a mixed-effects model. Estimated effect measures were calculated for event-related outcomes as odds ratio (OR). Mean differences (MD) with inverse-variance were also calculated considering a study confidence interval of 95% for continuous variables. Missing means with standard deviations were extrapolated either from medians with a range according to the formula proposed by Hozo et al. 36 or from interquartile ranges following the Cochrane Handbook for Systematic Reviews of Interventions guidelines. 37
Statistical heterogeneity and the Z-test for overall effect and relative two-sided P value were also assessed. Statistical significance was set at the <.05 probability value.
Quality assessment of the included studies were appraised by the guide of the Risk of Bias in Nonrandomized Studies- of Interventions (ROBIN-I) tool (Supplementary Table S1). 38
Results
Literature search
The first literature search identified 677 records globally. After duplicate exclusion, and title and abstract examination, 13 articles met the inclusion criteria and relative data entered the meta-analysis (1 study was an randomized controlled trial [RCT], 5 propensity score matching analysis, 2 case-matched analysis, and 5 comparative retrospective analysis).39–51 A total of 1267 patients were retrieved. Figure 1 shows the search strategy.
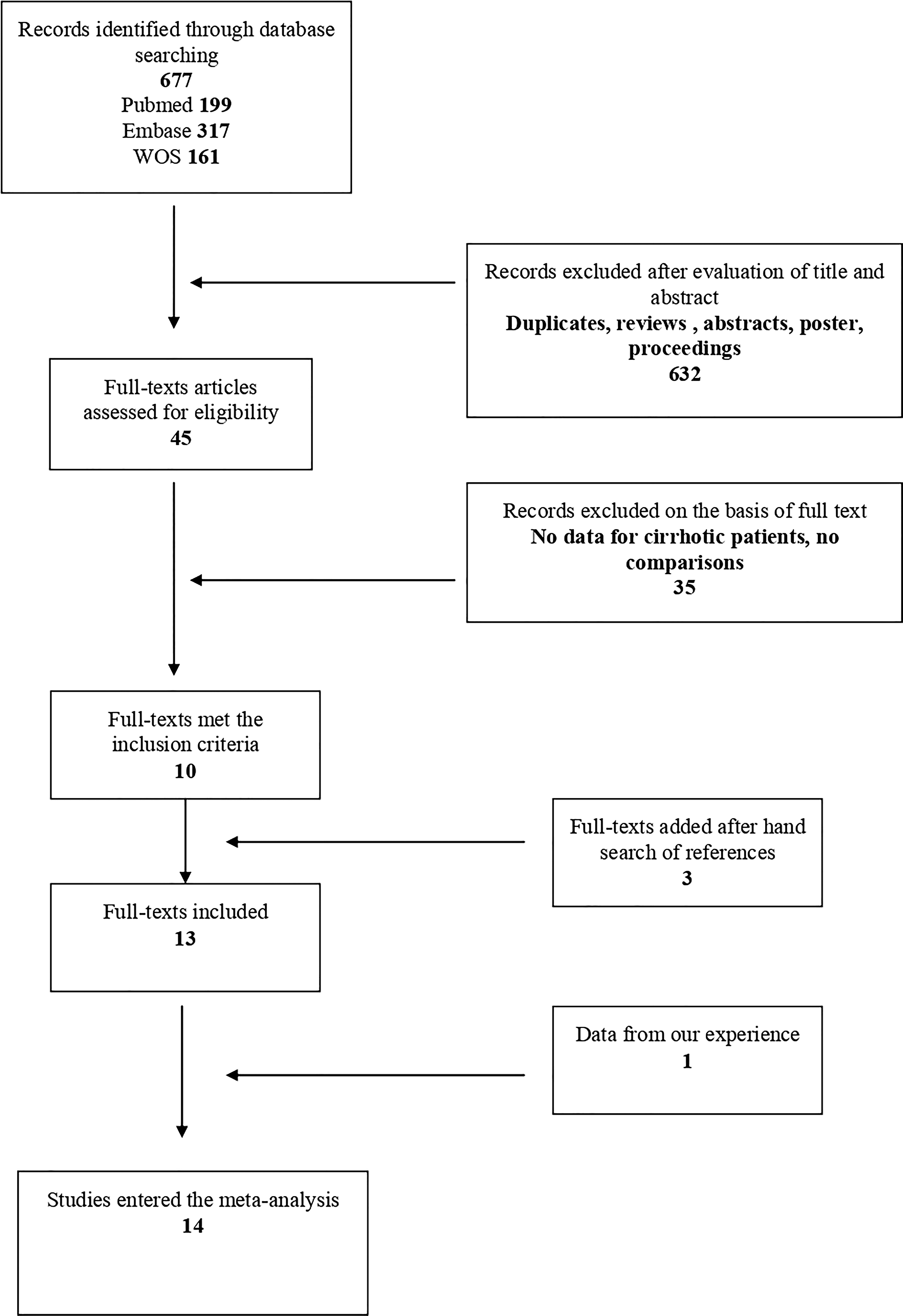
Flow diagram with search strategy.
National Cancer Institute surgical experience
Out of 719 liver resections performed at our center from June 2010 to February 2020, 158 had a diagnosis of HCC and 127 of these had also a background of cirrhosis. Within cirrhotic patients, 27 underwent MILR (20 liver resections and 7 robotic resections), who were case matched compared with a similar group of patients who underwent OLR. Table 1 depicts results of our case series that entered the meta-analysis. Retrieved data were added to those of a literature review, and finally, a total of 1321 patients, 757 in the OLR group and 564 in the MILR group, were considered in the meta-analysis. Characteristics of all the included studies are shown in Table 2.
Data About Our Series
P values in bold are statistically significant.
AL/POST, anterolateral/posterior; BCLC, barcelona clinic liver cancer; BMI, body mass index; BT, blood transfusion; ICGR 15%, indocyanine green retention; LOS, length of hospital stay; MELD, model for end-stage liver disease; MILRs, minimally invasive liver resections; OLRs, open liver resections; POLF, postoperative liver failure; SD, standard deviation; SSI, surgical site infections.
Characteristics of Included Studies
Data of our series.
BMI, body mass index; ICGR 15%, indocyanine green retention; MILRs, minimally invasive liver resections; OLRs, open liver resections.
Preoperative characteristics
Both groups had similar demographic characteristics.
Weighted mean age was 61.31 versus 62.35 in OLR and MILR groups, respectively; details on BMI were available from 474 patients from 7 studies with an average value of 24.79 versus 25.06. Child A patients were 654 and 504, Child B 55 and 40, and no Child C case was reported in the OLR and MILR groups, respectively (detailed data from 13 studies, 1253 patients). Of these, 99 had portal hypertension in the open group rather than 84 in the laparoscopic one (7 studies reported data about 524 patients). The meta-analysis was not possible for MELD Score and BCLC staging because only our and other three series reported.42,45,50 Only 9 articles (680 patients) included data about ICGR 15% with an average value of 16.55 versus 16.92 with no significance between the groups (MD = −0.30, I2 = 54, P = .76); 99 patients in the open group and 66 in the laparoscopic group had multiple tumors (data available from 9 studies); all articles (1321 patients) reported tumor size with a mean of 4.4 versus 3.0; as a result, the OLR group had greater statistical significance than the MILR (MD = 0.47, I2 = 82%, P = .006) (Table 3).
Preoperative Characteristics
P values in bold are statistically significant.
BMI, body mass index; ICGR 15%, indocyanine green retention; MILRs, minimally invasive liver resections; OLRs, open liver resections.
Operative findings
Major hepatectomies were performed in 64 patients (8.45%) from the open group and in 29 (5.15%) from laparoscopic one (data from all studies, 1321 patients, OR = 1.73, P = .03, I2 = 84%). Data dealing with tumor location and relative resection were available for 628 patients (data from 9 studies); relative percentage of anterolateral versus posterior segments were 76.34% versus 23.66% for OLRs and 88.1% versus 11.9%for MILRs. The mean operative time varied between 120.32 and 330 minutes for MILR and between 146.8 and 342.75 for OLR. At the meta-analysis, there was an MD of 10.08, P = .002, with high heterogeneity among the studies, I2 = 84%. Overall, the Pringle maneuver was required in 85 (21.19%) OLR patients versus 41 (13.75%) MILR patients (data of 7 studies, 699 patients). Results showed lower EBL in the laparoscopic group (from 88 to 483 mL) compared to the other group (from 200 to 580 mL) (MD = 169.29, I2 = 84%, P < .00001). Figure 2. Conversions varied among the studies included (0–10). The overall proportion of laparoscopic procedures converted to conventional open surgery was 8.4% (40, data from 11 studies, 473 patients) (Table 4).
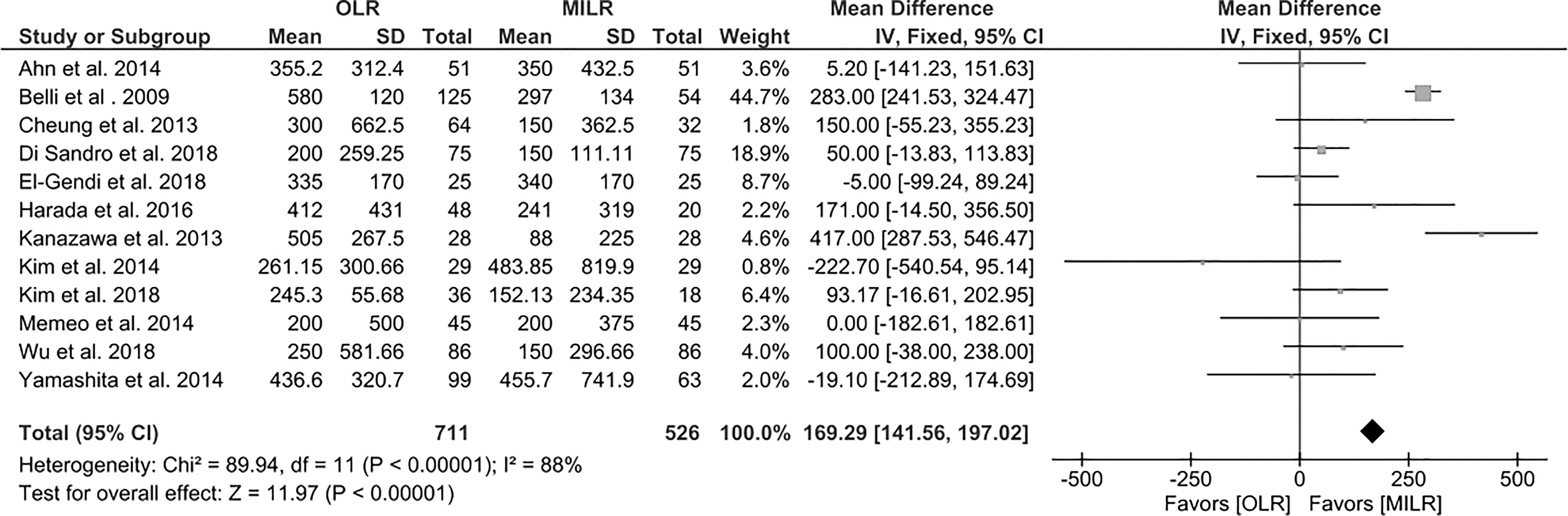
Forest plot depicting estimated blood loss.
Operative Findings
P values in bold are statistically significant.
AL/POST, anterolateral/posterior; EBL, estimated blood loss; MILRs, minimally invasive liver resections; OLRs, open liver resections.
Postoperative outcomes
All included studies reported data regarding postoperative morbidity. The postoperative outcomes are illustrated in Table 5. There was a statistically significant difference between the 2 groups in overall morbidity, with 38.04% (288 out of 757 patients) and 19.32% of patients (109 out of 564) suffering from complications in the OLR and MILR groups, respectively (OR = 2.90, P < .00001, I2 = 0%).
Postoperative Outcomes
P values in bold are statistically significant.
BT, blood transfusion; LOS, length of hospital stay; MILRs, minimally invasive liver resections; OLRs, open liver resections; POLF, postoperative liver failure; SSI, surgical site infections.
For 980 patients (detailed data from 12 studies, 3 of these reported only grade ≥III), postoperative complications were reported in accordance with the CD classification system. Around 15.75% of patients had CD ≤ II in the open group and 8.8% in the laparoscopic one showing significance in favor of the MILR group (OR = 1.96, P < .002, I2 = 0%); CD ≥ III was 12.75% versus 5.66 and the laparoscopic group reported significantly less major complications (OR = 2.01, P < .02, I2 = 14%).
With regard to postoperative ascites, data on 992 patients from 12 studies were available. The overall incidence of ascites was 8.46% (84 patients), 12.9%, and 2.7% being the relative rates for MILR and OLR, respectively. This difference was statistically significant (OR = 5.16, P < .00001, I2 = 11%) (Fig. 3).
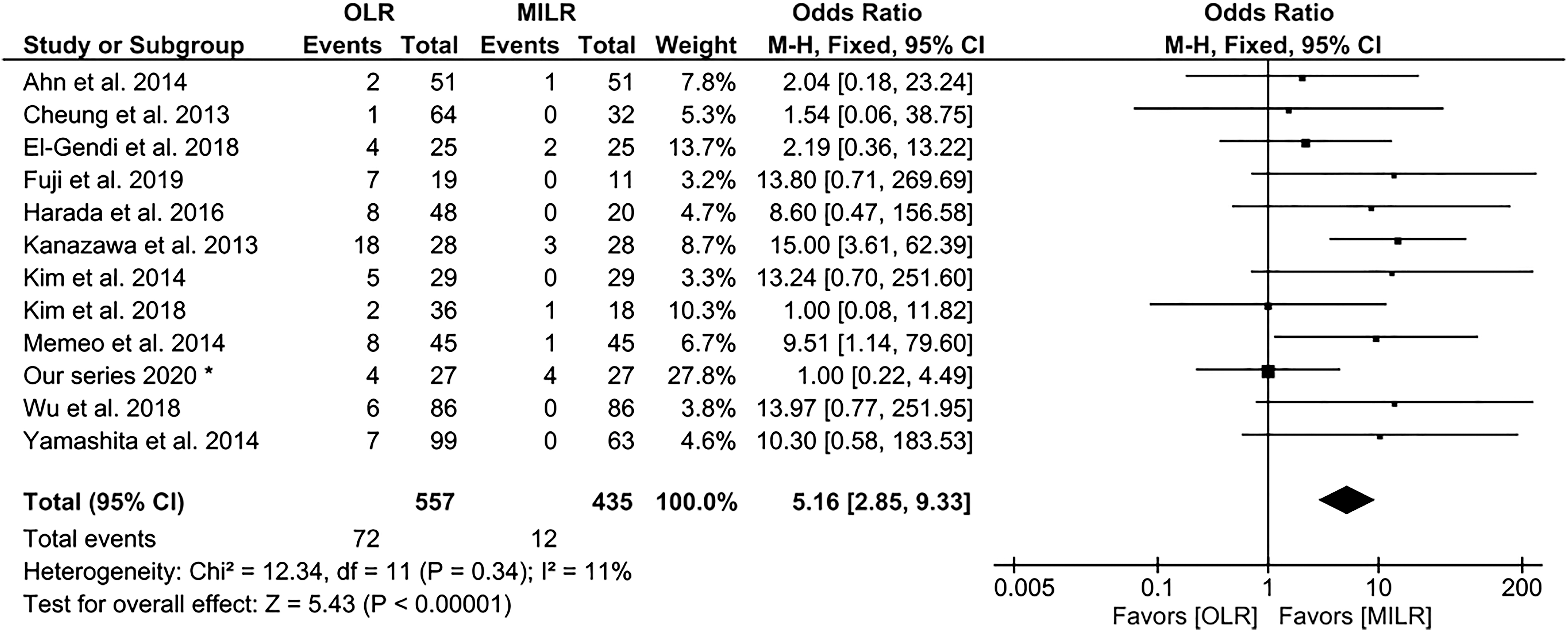
Forest plot showing postoperative ascites.
The bile leak rate was 1.7% (18 out of 1027 patients, 10 studies). It did not vary significantly between the 2 groups (1.7 OLR versus 1.8 MILR percent, OR = 0.0, P = .96, I2 = 0%). By analyzing the 9 studies that provided circumstantial data, 10.7% of patients had POLF in the postoperative period (78 out of 728 patients). There was a statistically significant difference in favor of LLR group (13.61% versus 7.51%, OR = 0.06, P = .009, I2 = 0%) (Fig. 4).
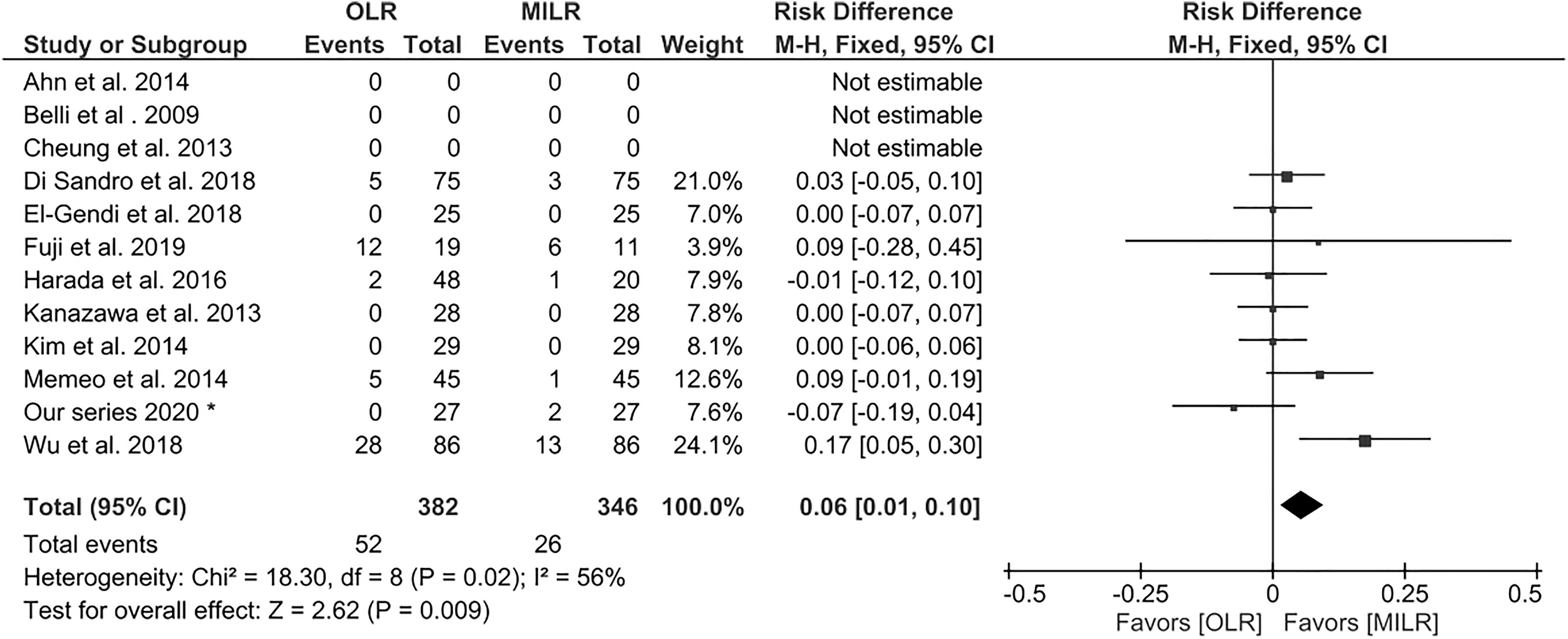
Forest plot about POLF. POLF, postoperative liver failure.
Data on SSI were available from 13 studies, including 1291 patients. Overall, 3.87% of patients had evidence of postoperative SSI, 5.42 and 1.8 being the relative incidence for OLR and MILR, respectively (OR = 2.75, P = .002, I2 = 0%).
Six studies provided data on the incidence of reintervention. There were 5 cases of reoperation among 510 patients (0.98%). The difference between the groups did not reach statistical significance (OR = 1.52, P = .65, I2 = 0%).
A total of 138 patients underwent BT (10.9%). The 2 groups differed in significance (OLR 13.2 versus MILR 7.9%, OR = 1.58, P = .02, I2 = 10%) (Fig. 5).
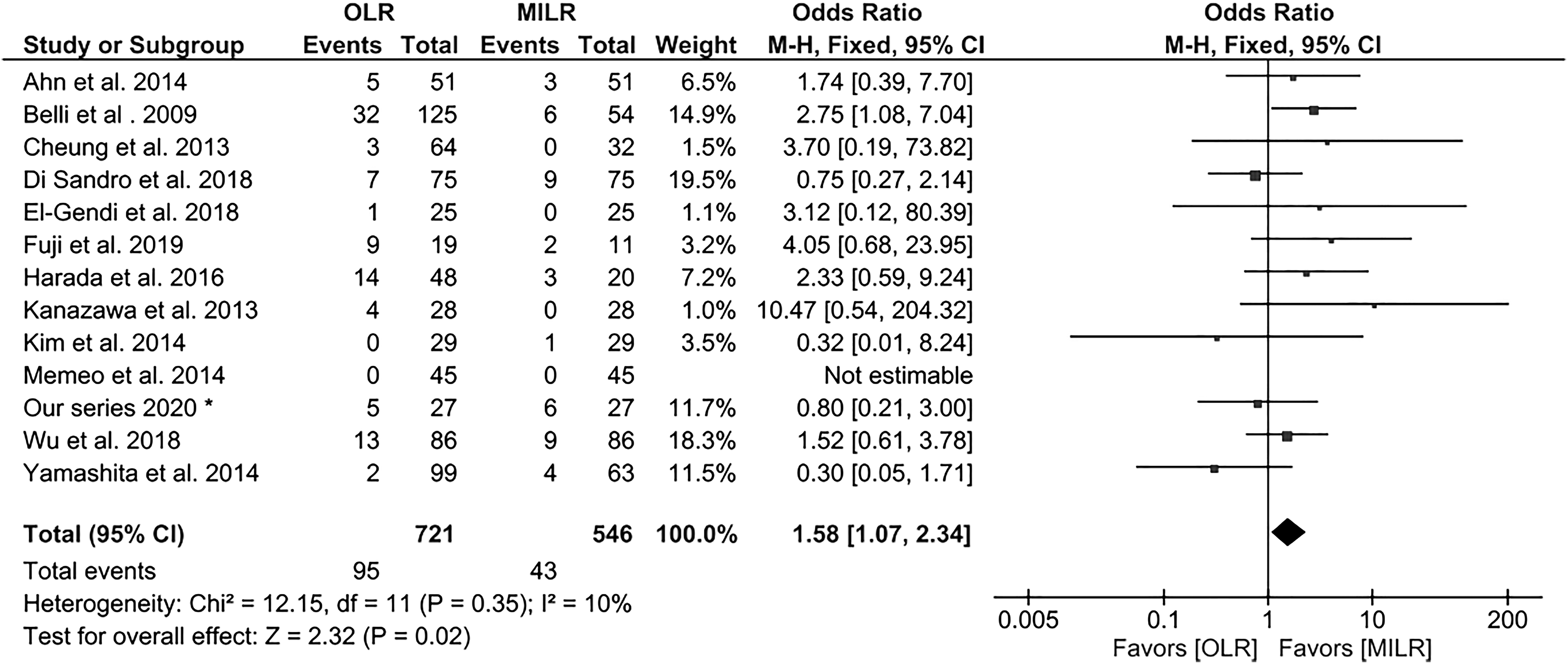
Forest plot depicting blood transfusion.
All studies provided specific data on mortality. In all the studies considered, mortality was defined as an in-hospital death or at 30 days from surgery. In total, there were 10 deaths among a total of 1291 patients (13 studies), defining an overall mortality rate of 0.8%. The relative rates of mortality did not differ between the 2 groups (OR = 2.32, P = .23, I2 = 0%).
The LOS ranged between 4.28–19 and 2.4–36 following OLR and MILR, respectively. Patients receiving minimally invasive surgery had significantly shorter postoperative hospitalization than patients undergoing conventional open surgery (MD = −3.30, P < .00001, I2 = 78%) (Fig. 6).
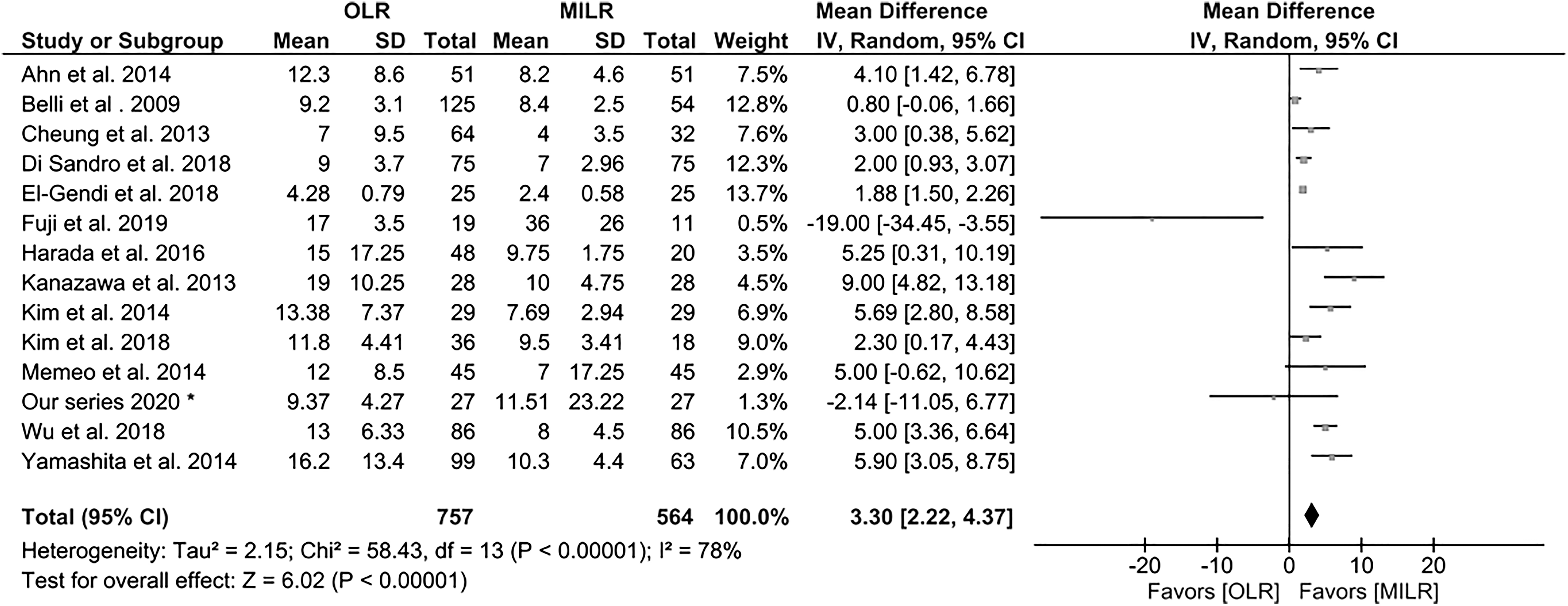
Forest plot of length of hospital stay.
Eight articles, including 731 patients, contributed to the analysis of radicality of resection. The overall rate of R0 resection was 94.8%, no significant difference between the groups was shown (OLR 93.8% versus 96.1% MILR, OR = 0.57, P = .13, I2 = 0%) (Fig. 7).
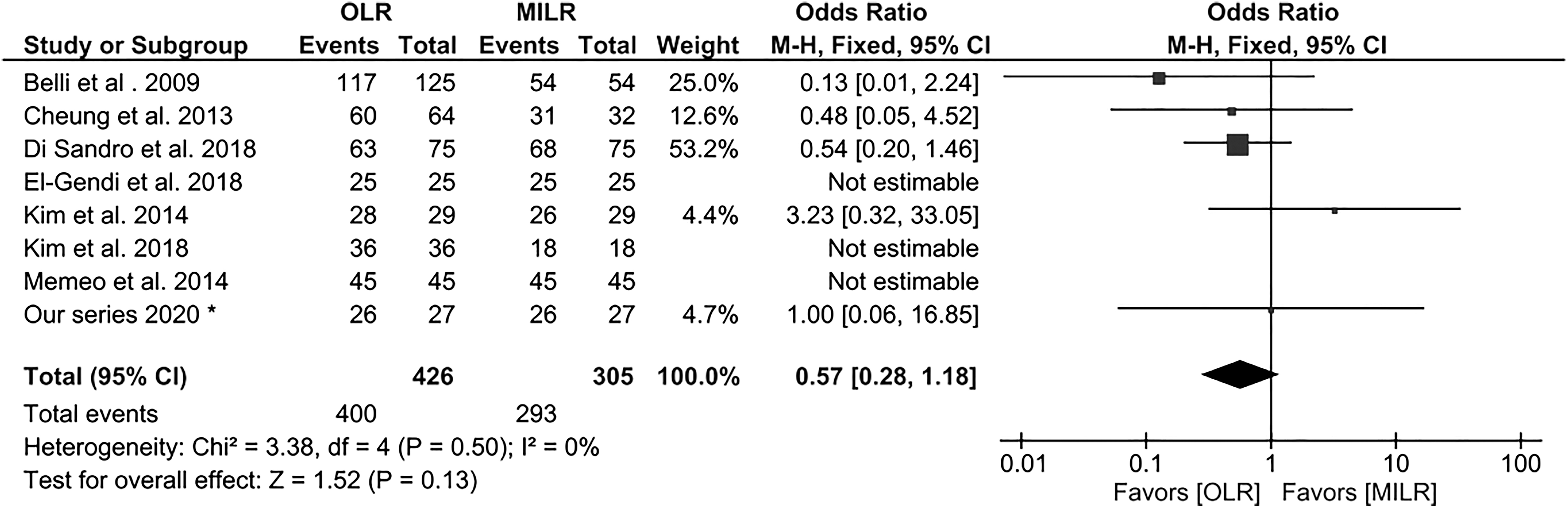
Forest plot depicting radicality of resection, R0.
Discussion
The aim of our study was to verify the available literature comparing MILRs versus OLR for HCC in patients with cirrhosis and portal hypertension. A systematic review and a meta-analysis including our surgical experience were performed. Data from a total of 1321 patients entered the study. MILRs showed to be superior over the conventional OLRs in operative time, EBL, BTs, postoperative complications, and LOS.
Minimally invasive surgery has gained great favor in general and digestive surgery showing better outcomes when compared to conventional surgical approaches from its early employment also in the field of oncology.48,52–57 MILRs enhanced its indications in the past decade, becoming the surgical approach of choice in almost all types of liver resections in minor and major hepatectomies, allowing to decrease postoperative complications, surgery-related and liver-specific morbidity, BT, and LOS.58–64 It is well known that cirrhotic patients have increased risk factors in developing complications in the postoperative period.65–67 Liver cirrhosis and portal hypertension could preclude liver resection as the treatment of choice in cases of hepatic malignancy. In conventional open hepatic resection, an abdominal incision is needed for proper mobilization and resection of the liver parenchyma in difficult conditions due to fibrosis, high portal pressure, altered coagulation, and refractory ascites with a higher risk of postoperative complications and increased mortality rate. 68 The laparoscopic approach seems to be able to overcome the perioperative difficulties common to cirrhotic patients, thanks to minimizing surgical trauma with small incisions, which avoids ligation of paraumbilical veins, and reducing time of pedicle clamping.69–72 Several authors reported good outcomes of LLRs in liver malignancy and one shows the superiority of minimally invasive surgery over the conventional open approach.23,73,74 The debate on whether laparoscopic surgery is superior to open surgery in cirrhotic patients with HCC remains substantially unresolved. We aimed to analyze the literature on this topic to answer this question.
From our meta-analysis, OLR and MILR groups resulted well balanced in regard to demographic and preoperative characteristics, except for tumor size showing significantly greater nodules for the open group. Since most of the studies are not randomized trials, these results are likely due to the preoperative selection of patients and the relative indication for surgical approach, and that patients with larger tumors were scheduled for open procedures.
Major hepatectomy was performed for about 7.04% of all series with a higher number in the OLR group for posterior resections. These data on the one hand shows that the open approach could facilitate major surgery, but on the other, the small overall percentage reveals the unwillingness to perform greater technically difficult liver resections in cirrhotic patients like Aranha et al. In the early 1980s, his article described a simple cholecystectomy as a “formidable operation.” 75 In the patient selection criteria for the laparoscopic approach, two mean criteria were considered by all the authors, they are tumor location and tumor size. Neoplasms located in segments 2 to 6 are considered the best indications for laparoscopic procedures compared to 7, 8, and 1, which are difficult to visualize laparoscopically and require appropriate hepatic mobilization for resection. The role of minimally invasive surgery for lesions in posterior segments and for major resections has not yet been completely codified. As for the dimension of tumors, except for exophytic lesions apparently easy to resect, laparoscopy is usually not recommended for tumors greater than 5 cm in diameter because of the difficulty during neoplasm mobilization with risks of rupture or possibility of inadequate margins.17,59,69,76–83
As for operative time and EBL, MILRs reported significantly faster procedures with minor intraoperative bleeding, perhaps due to the minority of tumor size and thus the width of resection. Consequently, also the data regarding BTs rate showed a significant lower number of transfusions in MILR. Overall, conversion was about 8.4%, in line with those reported from several authors for MILR to date. 84 The OLR group was accompanied by a significantly greater number of postoperative complications, overall morbidity was nearly double the percentage rate compared to MILR. As for liver-related complications, in particular POLF and ascites, once more, minimally invasive resections have reached significantly better outcomes compared to conventional open results, despite similar preoperative values of ICGR 15%. These expected results confirmed that reduced surgical trauma due to closed-abdomen surgery, lower portal pressure, and consequent minor EBL has less influence on the balance of liver homeostasis. No differences were noted on bile leaks depending perhaps on factors that are not related to minimally invasive or conventional surgical approaches.
Another outcome in favor of MILR was the rate of SSI with a statistically significant lower incidence compared to OLR, indisputably due to the large incision performed during conventional surgery and its relative intrinsic modality of action.
According to the results reported above, even the LOS resulted significantly shortened for the MILR group; El-Gendi et al. reported the lowest median hospital stay as 2.4 day. 43
No difference between the groups regarding mortality of reintervention rate was noted.
Like previous reports affirming that minimally invasive surgery achieves the same radicality of resection, our study shows a slightly higher percentage of R0 resections for the MILR group, but without reaching statistical significance.17,85–88
However, several limitations in this study must be recognized. First, the studies considered represent mostly retrospective analyses and case series; only one RCT met the inclusion criteria and was included in the meta-analysis. We also should consider much of the data derived from single and initial experience of surgeons or surgical teams. Second, we had to exclude some studies due to the lack of cirrhotic patient subgroups and the absence of needed detailed data. Third, data reporting on tumor locations were not in line with the Brisbane definitions in all considered studies and were usually not specified when multiple nodules were considered in the same segment. This did not allow to describe true differences between anterolateral and posterior resections within the groups. With regard to oncological outcomes, very few studies reported data on radicality of resections comparing the MILRs to OLRs, which may affect the chance of considering this important feature.
Conclusions
Evidence present throughout literature on the efficacy of MILRs and on the superiority of one technique over another is still scarce. Minimally invasive techniques rather than open approaches for HCC surgery in cirrhotic patients could reduce postoperative overall morbidity, liver-related complications, and LOS. Nevertheless, the lack of high-level studies on this peculiar topic precludes the possibility of obtaining decisive conclusions.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.