
Abstract
Background:
Although bariatric surgery is a standardized procedure, it is not without complications. Image-guided surgery allows minimally invasive resolution of complications, making it ideal for bariatric patients. The objective of this work was to analyze the image-guided surgery approach to postoperative complications of bariatric surgery.
Materials and Methods:
Retrospective comparative study in patients with complications after bariatric surgery. Patients were included consecutively according to selection criteria. All the patients were treated by the same surgical team.
Results:
n = 58 patients were recruited. The average age was 47.3 (range 16–62) years; the distribution by sex was male 52% and female 48%. Average body mass index was 42% (±1.26). The associated comorbidities were diabetes mellitus 41% (±0.49), dyslipidemia 41% (±0.49), and high blood pressure 39% (±0.48). Of the total, 39 (67.2%) underwent laparoscopic sleeve gastrectomy (LSG) and 19 (32.8%) under Roux-en-Y Gastric Bypass (RYGB) (P ≥ .05). Complications reported were leaks/fistulas (with/without abdominal collections) in 94.8% (±0.22), gallstones 3.5% (±0.18), and hemorrhage 1.7% (±0.13). There was no statistically significant difference between the type of bariatric surgery (LSG versus RYGB) and the complications found (P ≥ .005). There were no intestinal obstructions, strictures or acute gastric dilations, or deaths. The treatment of complications was approached percutaneously (56.9%), endoscopically (29.4%), reoperation laparoscopically (12%), and clinical control (1.7%).
Conclusion:
The image-guided surgery approach to postoperative complications of bariatric surgery is feasible and safe. Good results are obtained with a decrease in the surgical comorbidities associated with the procedure.
Introduction
Obesity is a disease that affects millions of people worldwide. Its incidence is on the rise in the United States, Europe, South America, and Australia. 1 It brings associated severe comorbidities such as arterial hypertension (or high blood pressure, HBP), diabetes (diabetes mellitus [DM]), dyslipidemia (DLP), heart disease, or lung disease. 2 For this reason, its treatment requires an interdisciplinary approach with clinical doctors, bariatric surgeons, nutritionists, psychologists, endocrinologists, and traumatologists, among others. Obesity surgery has shown great benefits in this group of patients. 3
Currently, the most frequently used surgical treatments are laparoscopic sleeve gastrectomy (LSG) and Roux-en-Y Gastric Bypass (RYGB).4,5 The other techniques are reserved for specific patients. Like any surgical procedure, it is not without complications. 6 The most frequent are leaks/fistulas, abdominal collections, hemorrhages, intestinal obstruction, and gallstones.
Image-guided procedures have developed rapidly in recent years. 7 The combination of imaging systems and navigation guides allows minimally invasive postoperative complications to be resolved, with lower complication rates, less pain, and rapid recovery. This approach is ideal due to the characteristics of patients undergoing bariatric surgery.
The increasing number of obese patients, associated with the widespread of bariatric surgery, forces the acting surgical team to detect complications early and learn about treatment options.
The objective of this work was to analyze the application of the image-guided surgery approach to postoperative complications of bariatric surgery.
Materials and Methods
Retrospective comparative study was carried out in patients with postoperative complications after bariatric surgery. It was carried out by the CIEN-DIAGNOMED Center in conjunction with the DAICIM Foundation in Buenos Aires, Argentina, between January 2005 and January 2020.
The following Selection Criteria were applied: (1) Inclusion Criteria: patients with morbid obesity in whom therapeutic bariatric surgery (LSG or RYGB) was performed in our center, patients with immediate–mediate complications after bariatric surgery; (2) Exclusion Criteria: patients with complications after bariatric surgery whose technique has not been LSG and/or RYGB, patients derived from other centers, patients with complications after bariatric surgery not associated with the procedure (deep venous thrombosis [DVT], pulmonary thromboembolism [PTE], others).
All patients were treated by the same group, both during primary surgery and its associated complication.
Surgical technique
Preoperative preparation
All patients underwent preoperative, intraoperative, and postoperative follow-up to decrease any associated complications. 8 The patients presented a preoperative clinical, psychological, and nutritional control according to the same multidisciplinary team.
At the time of surgery, under general anesthesia, the patients were placed in the supine position, with their arms and legs open. The administration of pertinent antithrombotic and antibiotic prophylaxis was performed.
Laparoscopic sleeve gastrectomy
Four ports were placed. The gastric sleeve was calibrated with a 32F orogastric tube. The gastrectomy was made using 3.5 × 60 mm staples. The staple line was reinforced with nonabsorbable material. The tightness of the sleeve was monitored by performing a hydropneumatic test with methylene blue. The sectioned stomach was removed with a bag. A silicone drainage was left at the surgical site. 4
Roux-en-Y gastric bypass
Five ports were placed. The gastrectomy was made using 3.5 × 60 mm staples. The Roux-en-Y was built antecolically. The anastomoses were performed with staplers. Gastric pouch tightness was monitored by performing a hydropneumatic test with methylene blue. A silicone drainage was left at the surgical site. 5
All the patients were controlled with oral fluoroscopic contrast at 48 hours, before the start of oral feeding.
Complications
The global rate of complications associated with bariatric surgery is estimated to be 10%, including bleeding, leakage, fistula and abdominal collection, intestinal obstruction, stricture, and acute gastric dilatation.9–12
Postoperative stenosis
It is defined as the decrease in the size of the digestive lumen. Its postoperative incidence is 3% to 30% for gastrojejunoanastomosis (RYGB) and 0.3% to 4% for gastric sleeve (LSG). The main symptoms may be nausea, vomiting, and abdominal pain. This complication is usually due to a technical error. It usually appears at the level of the gastrojejunal and jejunojejunal anastomoses and in the gastric sleeve.
Leak/fistula
A leak is defined as the output of luminal content from a surgical junction between two hollow viscera or through a staple line of an organ, 13 while a fistula is defined as the abnormal communication between two epithelia. 14 Its incidence after bariatric surgery is 2.4% for LSG and 1% for RYGB.15–17 The main symptoms could be abdominal pain, ileus, fever, or sepsis. Gastric, intestinal, or nutritional debit could be obtained in the drains. It can focus and form an abdominal collection or an abscess. Its origin could be a combination of technical error with failure of the used stapling material. 18
Abdominal collection/abscess
It is defined as the presence of focused and localized fluid in the abdominal cavity. It may contain inflammatory, gastric, intestinal, or blood fluid. When it is made of purulent material it is called an abscess. The main symptoms are abdominal pain, intestinal ileus, vomiting, and fever. It can trigger a sepsis situation. It is usually secondary to a leak or fistula. It usually appears on the staple line of the stomach and anastomoses. Its origin could be the same as that of the leaks and fistulas, in addition to insufficient washing and aspiration of the surgical site.
Biliary lithiasis
One of the most feared complications of gallstones is choledochal lithiasis. It may originate at the gallbladder level with stones that move to the main bile duct (in noncholecystectomized patients) or from de novo or residual gallstones (in cholecystectomized patients). 19 Its general incidence after bariatric surgery is of the order of 37%. The main symptoms could be abdominal pain, nausea and vomiting, loss of appetite, jaundice, choluria, and acholia.
Acute gastric dilation
It is an exaggerated and sudden dilation of the stomach. Its incidence is low but it presents high mortality. The main symptoms could be abdominal pain, nausea, vomiting, and bloating. Its origin is not exactly known.
Diagnosis of complications
The diagnosis of complications was carried out from a clinical approach taking into account their vital parameters (Blood Pressure, Heart Rate, Respiratory Rate, Temperature) and specific parameters (diuresis, general, and particular digestive symptoms), together with an analysis laboratory (hematocrit, white blood cell count, etc.). The presence of abdominal or collection fluid, as well as biliary lithiasis, was confirmed by ultrasonography (US) and/or computed tomography (CT). The detection of leaks and fistulas was determined with the use of contrast fluoroscopic studies.
Percutaneous technique
The basic technique used is called “Seldinger's Technique,” in which a puncture is made of the site to be treated (such as collection, abscess, hematoma, leak site, gastric remnant, and so on) guided by some method per image (US, CT, radioscopy, other) either alone or combining various technologies. Once puncture is complete, a 0.035′′ J-tip guide is inserted through the needle into the job site to ensure access. Confirmed with the image guide the correct position of the guide, the needle is removed and dilators are inserted to facilitate the entry of the final catheter. After removing the dilators in question, a multipurpose catheter is placed, the sizes of which can vary depending on the case. In general, catheters have a “pigtail” type safety system that prevents it from moving. Finally, the catheter is permeabilized with 5 cc of saline solution and fixed to the skin with suture.
Statistical analysis
Statistical data were analyzed using computer programs. The results were expressed in percentage, range, and standardized deviation. The chi-square test was used for the statistical analysis of the variables. A 95% confidence interval was applied, and a value of P < .05 was indicated as statistically significant.
Results
A total of n = 58 patients were consecutively recruited. All presented complications after bariatric surgery. Of these, 39 (67.2%) underwent LSG and 19 (32.8%) underwent RYGB. Regarding sex, 28 were female (±0.5%–48%) and 30 were male (±0.5%–52%). The average age was 47.3 years (range 16 to 62). The average body mass index was 42 (±1.26). Regarding associated comorbidities, 23 (±0.49%–41%) patients presented DLP, 23 (±0.49%–41%) DM, and 22 (±0.48%–39%) HBP (P ≥ .05).
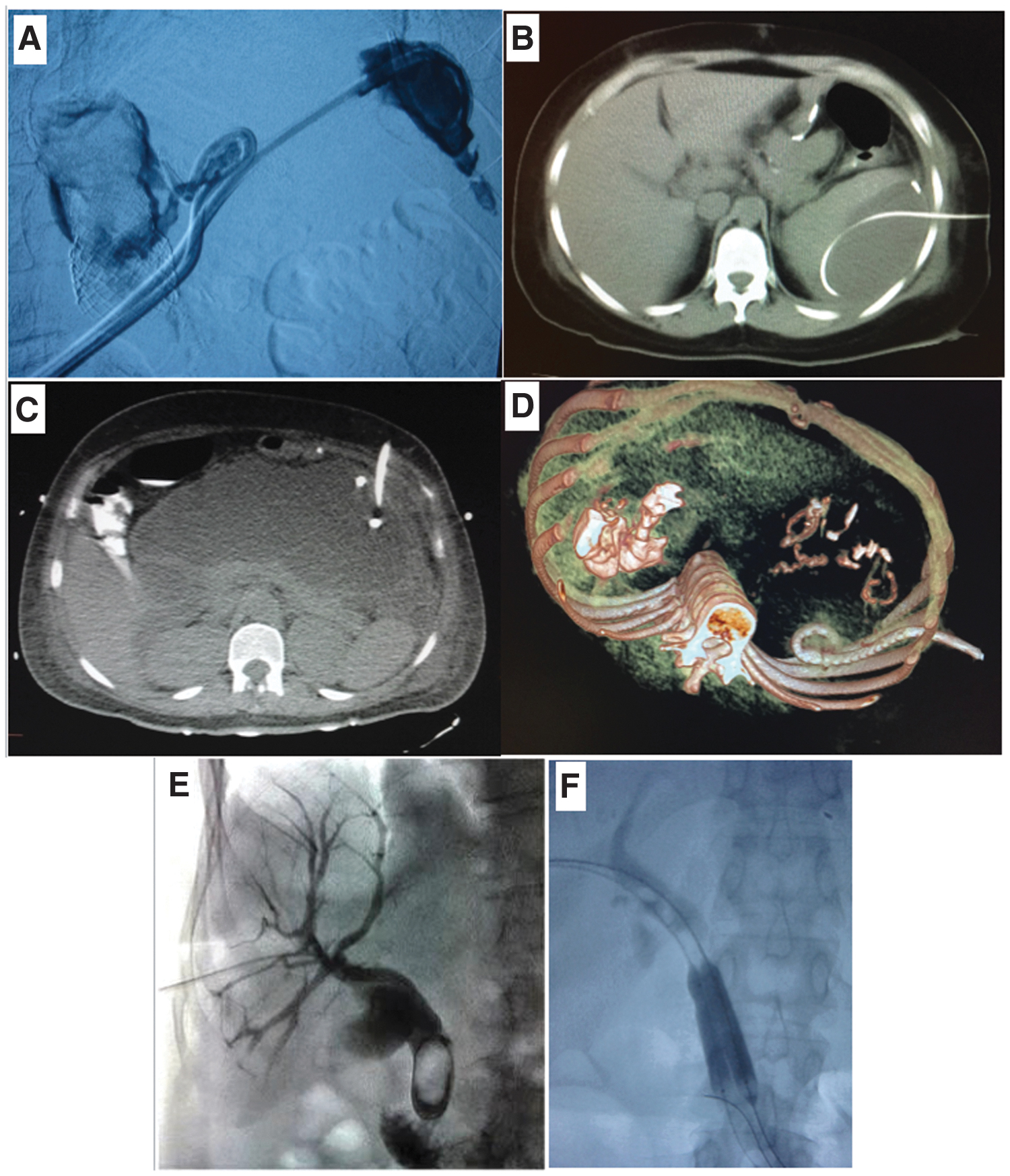
Regarding the complications (Table 1), the following were reported: leaks/fistulas (Fig. 1A), some with abdominal collections (Fig. 1B–D), hemorrhage, and gallstones (Fig. 1E). There were no intestinal obstructions, strictures (stenosis), or acute gastric dilations. Most complications correspond to leaks/fistulas in postoperative LSG patients. There was no statistically significant difference between the type of bariatric surgery (LSG versus RYGB) and the complications found (P ≥ .005). No deaths were reported.
Postoperative Complication Analysis
With or without abdominal collection/abscess.
LSG, laparoscopic sleeve gastrectomy; n/s, non-significance; RYGB, Roux-en-Y gastric bypass.
Regarding the type of treatment (Table 2) established to resolve complications, 56.9% corresponded to a percutaneous approach, 29.4% to endoscopy, 12% required reoperation laparoscopically, and 1.7% sufficed with a clinical control.
Treatment of Complications
Blood transfusion for bleeding.
One patient required ERCP+laparoscopic cholecystectomy for biliary lithiasis.
ERCP, endoscopic retrograde cholangiopancreatography; LSG, laparoscopic sleeve gastrectomy; RYGB, Roux-en-Y gastric bypass.
Discussion
Bariatric surgery has seen an increase in its practice due to the global obesity epidemic. Although there are several types of bariatric procedures that can be performed according to the characteristics of the patient to be treated, the most widely used are LSG and RYGB. Despite being standardized and safe surgeries, they are not without complications, with an overall incidence of 10%. 6 In this work we observe that most of the complications were leaks, patellas, and collections, which is logical due to the large number of LSGs carried out.
On occasions, complications after bariatric surgery are difficult to treat due to the patient context (postoperative, obesity, comorbidities). 20 About 40% of the patients recruited in this work present at least some associated morbidity. At this point is where image-guided surgery takes center stage. Every surgeon must have the possibility of accessing this therapeutic arsenal to resolve any complications that arise.
Minimally invasive surgery rewards the reduction of surgical “aggression” during a procedure. Here we find laparoscopic, endoscopic, and image-guided (percutaneous) surgery. The latter is the combination of invasive procedures with the support of medical images, be it fluoroscopy, US, CT, and magnetic resonance. It allows diagnosing the complication to be treated, planning its treatment, and carrying it out in a minimally invasive manner with all the benefits that this presents (less pain, less bleeding, rapid recovery, bedside procedures).
In this article you can see the range of therapeutic possibilities for these patients. Leaks, fistulas, and collections were first addressed percutaneously. Endoscopy was sometimes used to treat leaks or fistulas that had a large defect. 21 These were favored with the use of clips, covered prostheses, or sealants. Regarding gallstones, we detected choledocyan lithiasis in two cases. One of them was after LSG; a previous ERCP (Endoscopic Retrograde Cholangiopancreatography) was performed to remove the stone and leave the main bile duct clear.22–24 Then the corresponding laparoscopic cholecystectomy was performed. In the other case, it was after RYGB. This last situation is very undesirable, because the normal anatomy of the upper gastrointestinal tract was surgically modified and ERCP cannot be performed. We solved this problem with a very interesting method, using antegrade papillary balloon dilation technique. 25 First, we perform transhepatic percutaneous biliary drainage, then dilate the papilla with a high pressure balloon, and finally push the gallstone through the papilla into the duodenum (Fig. 1E, F).
One of the limitations of this work is the number of patients and the heterogeneity of the procedures applied.
In general, we were able to observe that most of the complications benefited remarkably with image-guided procedures. So much so that no deaths associated with the procedures were reported.
Conclusion
The application of the image-guided surgery approach to postoperative complications of bariatric surgery is feasible and safe. It allows obtaining good results with a notable decrease in the surgical comorbidities associated with the procedure. Minimal invasive surgery could be considered as first-line treatment in obese patients with postoperative complications of bariatric surgery.
Informed Consents
All patients signed an informed consent to participate in research and to allow us to use their data for publication.
Ethical Approval
The approval of our institutional ethics committee was obtained before the start of the study.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.