
Abstract
Introduction:
Management of the distal ureter during laparoscopic nephroureterectomy (LNU) for upper tract urothelial carcinoma (UTUC) is controversial. The aim of this review was to determine whether this affects oncological outcomes.
Methods:
A literature review was conducted searching MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials in June 2019. Studies reporting outcomes of LNU in UTUC using either open, laparoscopic, or endoscopic approaches to excise the distal ureter were identified. All eligible studies underwent critical appraisal and were excluded if not of sufficient quality. Cumulative analysis of the results was performed.
Results:
Nine studies with a total of 383 patients (168 open, 159 laparoscopic, and 56 endoscopic excision of distal ureter) were eligible for inclusion. Study design and outcome reporting were variable between studies. Mean age of patients was comparable (67.7 years versus 65.0 years versus 66.6 years). Mean follow-up duration was comparable between open and laparoscopic groups (46.2 months versus 45.5 months) but reduced in the endoscopic group (33.4 months). The open group had a higher proportion of high grade/G3 tumors and pT2-4 tumors when compared to the laparoscopic and endoscopic groups (P < .001 and P = .002). The open group had a higher rate of intravesical recurrence and the laparoscopic group had a higher rate of distant metastases (P < .001).
Conclusion:
This review has identified differences in oncological outcomes between different techniques of managing the distal ureter in LNU for UTUC. However, the poor reporting of potentially confounding factors does not enable any one technique to be recommended as superior and requires further research.
Introduction
Upper tract urothelial carcinoma (UTUC) accounts for 5%–10% of all cases of urothelial carcinoma and is around twice as common in the pelvicalyceal system than the ureter.1,2 In recent years, the average age at diagnosis has risen from 67.9 to 72.9 years, the incidence has doubled, and we have seen a decline in 5-year survival rates, estimated to be 48% compared to 60% during the 1980's. 3
Traditionally, the treatment of UTUC was with an open nephroureterectomy (ONU). But the development of laparoscopic and endoscopic surgery now provides a number of alternative options. Laparoscopic nephroureterectomy (LNU) was first described in 1991. 4 Comparative studies have demonstrated LNU to have similar efficacy to ONU, with the expected benefits of improved postoperative pain and shorter recovery time.5–8 In 2017, 71% of all radical nephroureterectomies in the United Kingdom were performed laparoscopically. 9 Therefore, it is crucial that we understand the best technique to perform LNU to achieve the best oncological outcomes.
One of the main concerns with LNU is the management of the distal ureter which is arguably the most important step to gain adequate oncological control. UTUC has a high recurrence rate, and if the distal ureter is not completely excised, the ureteric remnant is at risk of recurrence with reported rates of 33%–75%. 10 Given the extensive use of LNU, there is a need to understand the safety and efficacy of different techniques to excise the distal ureter, particularly in relationship to oncological outcomes. A number of different techniques have been described to excise the distal ureter during LNU, which can be broadly defined as open, endoscopic, laparoscopic, or robotic.
Open removal and bladder cuff excision
Open removal of the distal ureter in LNU is similar to ONU. The kidney and proximal ureter are mobilized laparoscopically, and then to excise the distal ureter and bladder cuff, a lower midline, modified Pfannenstiel, or Gibson incision is made. 11 The distal ureter is clamped and bladder cuff obtained via placement of an extravesical clamp or an anterior cystotomy. 12 The entire specimen can then be removed en bloc and bladder closure performed.
Several studies have made comparisons between LNU and ONU using the open approach for distal ureter removal and found noninferior oncological outcomes.6,13–19 Therefore, it is appropriate that alternative techniques for excising the distal ureter in LNU are compared with the open approach.
Endoscopic excision
Two main methods for excising the distal ureter and bladder cuff endoscopically have been described: the “pluck” technique and intussusception.
In 1952, the “pluck” technique was first described for use in ONU and later adapted for use in LNU.20,21 This involved endoscopic resection of the ureteric orifice using a Collin's knife into the perivesical fat to free the distal ureter. Then the ureter was placed on traction through the flank incision to pull it away from the bladder and complete the nephroureterectomy. 20 Several variations of the procedure have since been described focused on occluding the distal ureter before resection to minimize the risk of seeding cancer cells. These have included placement of an endoloop or Hem-o-lok clip around the intramural ureter, ureteric balloon catheter, fibrin sealant, as well as coagulation using a bipolar button or Thulium laser to seal the lumen.22–28
The intussusception or ureteral stripping technique was described in 1953 involving insertion of a ureteric catheter to which the distal ureter was secured. The nephrectomy was performed, ureter divided, and then, under cystoscopic guidance, the ureteric catheter was retracted until the mucosa was completely everted in the bladder and circumferential resection was performed around the everted ureteric orifice. 29 This technique has been demonstrated to have poorer oncological outcomes and is the only technique in the EAU guidelines to be actively discouraged.30,31
Pure laparoscopic excision
A pure laparoscopic approach can be challenging requiring the surgeon to work in a small space in the pelvis with a limited range of motion. In the first description after mobilizing the kidney, the ureter was clipped and dissected distally until the detrusor muscle fibers at the level of the vesicoureteric junction were reached. Using gentle traction, the ureter was tented up and a tissue stapler or Hem-o-lok clip was applied. 32 This initial description combined the procedure with endoscopic ureteric unroofing and was therefore not a pure laparoscopic approach. Yoshino et al. performed a pure laparoscopic approach by incising the bladder cuff and including the intramural ureter and ureteric orifice before stapling the base. 33 However, they noted that some patients went on to form stones at the staple site and modified their technique to not require stapling. 34
Robotic excision
Robotic surgery enables an improved range of motion when compared with laparoscopic surgery. 35 The initial description by Nanigian et al. used the robot to first incise the dome of the bladder to enable an intravesical approach for removal of the ureteric orifice and intramural ureter. 36 Other descriptions have used an extravesical technique. 37 In both approaches' bladder closure is also performed.
These numerous described techniques demonstrate the difficulties in the management of the distal ureter in LNU for UTUC presents. Most of the focus within the literature has been on comparing ONU to LNU with only limited comparisons made between different techniques to manage the distal ureter. There is currently a lack of understanding on the most efficacious technique to use to produce the best oncological outcomes. The purpose of this review is to compare the techniques of managing the distal ureter in LNU for UTUC with a focus on the oncological outcomes.
Methods
Search strategy and study selection
A literature review was conducted using a systematic approach and reported according to the PRISMA guidelines. The aim of the review was to answer the question, “Does the technique of managing the distal ureter during LNU affect oncological outcomes (recurrence and survival) and surgical outcomes for UTUC?” The primary outcomes were intravesical and extravesical recurrence rate, development of metastatic disease, cancer specific, and overall survival. Secondary outcomes were operating time, length of hospital stay, estimated blood loss (EBL), blood transfusions, complications, and positive surgical margins.
An electronic search of MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials was conducted in June 2019. In addition, a hand search of key urology journals, conference abstracts, and reference lists of retrieved articles was undertaken. The following key search terms were used in combination with Boolean operators; “urothelial,” “transitional cell,” “carcinoma,” “cancer,” “upper urinary tract,” “upper tract,” “kidney,” “renal,” “renal pelvis,” “ureter*,” “nephroureterectomy,” “nephro-ureterectomy,” “laparoscop*,” “robot assisted,” “robot-assisted,” “recurrence,” “mortality,” and “survival.” The full search strategy is given in Appendix Table A1.
Following the literature search, all duplicates were removed and the eligibility of the remaining articles was assessed. Studies eligible for inclusion were those written in English involving human patients undergoing LNU for UTUC only with a clearly defined approach to managing the distal ureter (open, laparoscopic, endoscopic, or robotic) and reporting at least one of the primary outcomes specific to the approach taken. Studies that were excluded included case reports, patients with a history of bladder cancer, metastatic disease, renal transplant, or dialysis. In cases where results from the same group of patients were published at different time points, the most recent publication was selected for inclusion.
All eligible studies were appraised using the Joanna Briggs Institute (JBI) critical appraisal tools. It was decided that to achieve a high-quality review, a score of 8 or more was required to be eligible for inclusion.
Data extraction
The following variables were extracted from each study: author, period of study, country of origin, study design, patient number, age and gender, body mass index (BMI), performance status, American society of anesthesiologists (ASA) grade, tumor location, stage and grade, nodal status, presence of carcinoma in situ (CIS), lymphovascular invasion, presence of tumor necrosis, cellular architecture, positive surgical margins, details of technique used to manage the distal ureter, use of intravesical chemotherapy, operating time, length of hospital stay, EBL, intraoperative and postoperative complications, rate of intravesical and extravesical recurrence, port-site metastases, distant metastases, time to recurrence, cancer-free survival, overall survival, and length of follow-up.
Data synthesis and analysis
Study characteristics and outcomes were synthesized into a narrative review. Meta-analysis was not performed due to the methodological and clinical heterogeneity of the studies. For the cumulative analysis where necessary to standardize reporting between studies conversion of the median and range to mean was based on established methods. 38 It was not possible to provide a statistical assessment of the significance between groups of parametric data due to the lack of information in the original study required to perform the ANOVA test. Nonparametric data were compared using the chi-square and Fisher's exact tests. When a statistically significant difference between groups was identified, post hoc analysis was performed to identify where that difference was. Statistical significance was defined as P < .05.
Results
After duplicates were removed the titles and abstracts for 364 studies were screened for eligibility. Full texts of 135 studies were retrieved. After screening, 25 studies were deemed eligible for potential inclusion (Fig. 1). Each study underwent the relevant JBI critical appraisal and a further 16 studies were excluded in accordance with the agreed quality score. Finally, 9 studies were eligible for inclusion in this review.
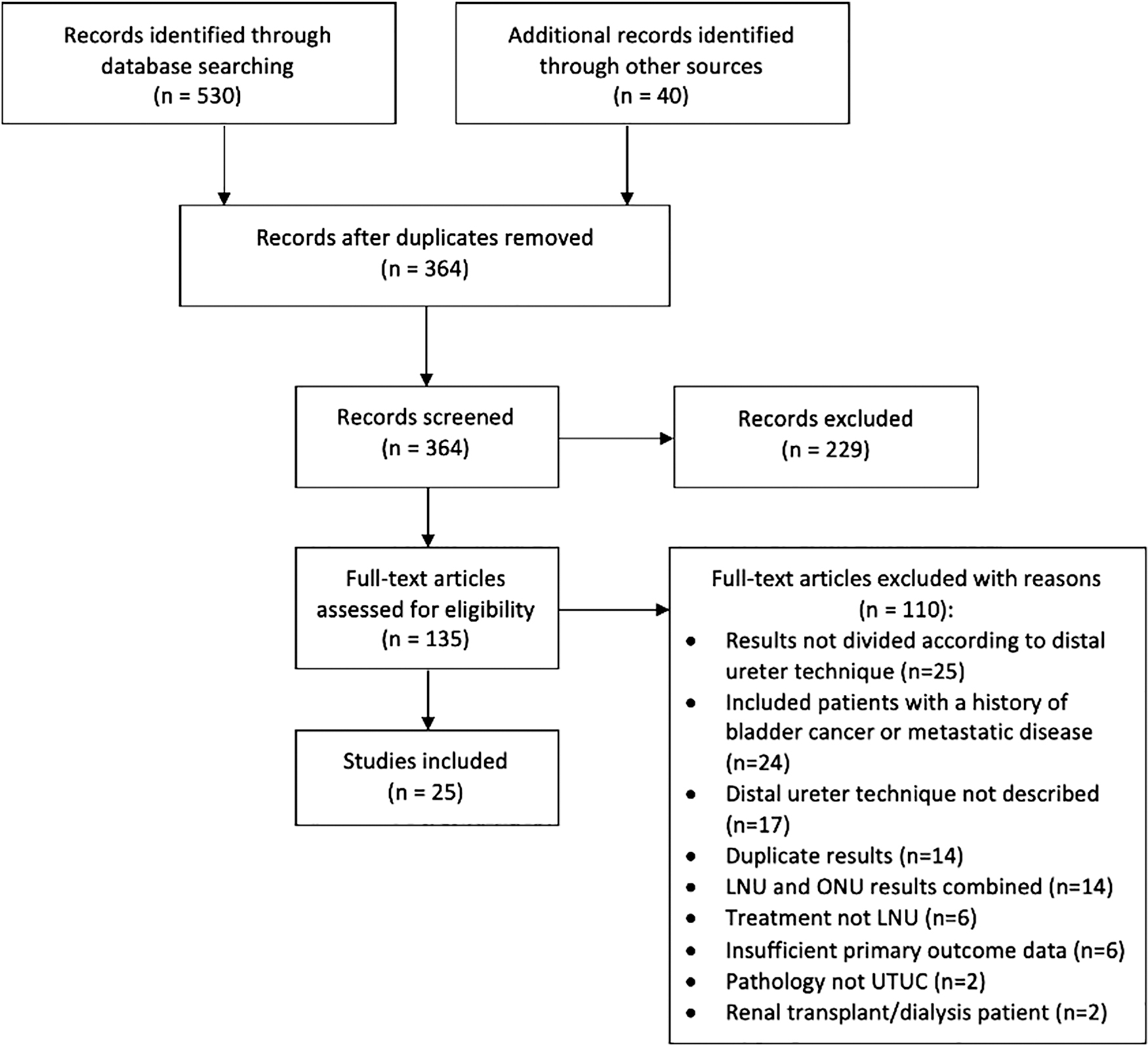
PRISMA flowchart depicting the study selection process.
Description of studies
The characteristics of the 9 included studies are shown in Table 1. Eight studies were reporting outcomes from a single center. One study was performed across three centers. 39 Four studies originated from China. Of the remaining 5 studies, one each originated from Germany, Italy, Japan, United Kingdom, and United States.
Study Characteristics Including Technique to Manage the Distal Ureter and Approach to Laparoscopic Nephroureterectomy for the Studies Included in This Review
RCT, randomized controlled trial.
The studies consisted of 1 randomized controlled trial (RCT), 4 cohort studies, and 4 case series. The RCT compared LNU and ONU using a standardized method for distal ureter excision. 40 Of the 4 cohort studies, 2 compared different techniques for managing the distal ureter.41,42 A further cohort study compared outcomes of patients who had received LNU using a standardized technique to ONU. 43 The final cohort study compared patients in two groups, based on pneumoperitoneum time, that had all undergone LNU. 39 The remaining 4 studies were all case series.28,44–46
Surgical technique and follow-up
The number of patients in each study ranged from 6 to 129 with an overall total number of 383. The studies used open, laparoscopic, or endoscopic approaches to manage the distal ureter. None of the included studies used a robotic technique.
There were 4 groups totaling 168 patients who received an open technique to excise the distal ureter. In one group it was clearly specified that the ureter was occluded before excision and bladder closure was achieved. 46 The other three groups did not specify.
A pure laparoscopic technique, in which the distal ureter was occluded before excision and bladder closure was achieved, was used in 5 groups with a total of 159 patients. Each study used different techniques to assist in the laparoscopic excision. Liu et al. applied a bulldog clamp to the baseline of the bladder cuff. 45 Gillan et al. used standard laparoscopic equipment to excise the distal ureter. 42 Greco et al. and Simone et al. used a Ligasure.40,43 Romero et al. used an endovascular gastrointestinal stapling device. 41
Finally, 3 groups with a total of 56 patients underwent endoscopic excision of the distal ureter. Guo et al. used a Thulium laser to occlude and excise the ureteral orifice and bladder cuff. 28 The authors did not specify whether bladder closure was achieved. Gillan et al. had a control group that used an endoscopic technique but did not specify the details. 42 Zou et al. used a Collins knife mounted on a resectoscope to score the ureteric orifice. 44 The authors then inserted a laparoscopic port directly into the bladder and used forceps to lift the distal ureter and bladder cuff to allow a Hem-o-lok clip to be applied to close the distal ureter before detachment from the bladder.
The use of intravesical chemotherapy after the procedure was reported in 3 studies. In 2, it was routinely given to all patients.28,44 In the third study, 33 patients received intravesical chemotherapy, but it was unclear how these patients were selected. 39
Follow-up of patients was reported to include regular cystoscopic surveillance for all studies. However, Guo et al. reported that only 31 of their 38 patients underwent cystoscopy and it was unclear whether the remaining 7 were lost to follow-up. 28 Therefore, these were excluded from the cumulative analysis for oncological outcomes. Regular follow-up of upper tract imaging either in the form of computed tomography or intravenous urogram was reported in 5 studies.39,40,43,44,46 The remaining 4 studies did not specify if imaging was performed as part of surveillance.
Patient demographics
Results of each individual study are shown in Tables 2–4. A cumulative analysis by technique of managing the distal ureter divided into open, laparoscopic, and endoscopic is shown in Table 5.
Patient Demographics and Tumor Characteristics of the Included Studies
All tumors located in renal pelvis or upper ureter this study did not differentiate further.
Only 10 of the 12 patients within the study with a reported
BMI, body mass index; CIS, carcinoma in situ.
Oncological Outcomes Reported in the Individual Studies According to Technique for Managing the Distal Ureter
Only 31/38 patients underwent cystoscopy unclear how the other patients were followed or if they were lost to follow-up, therefore excluded from cumulative analysis.
Follow-up time for each group not reported separately and therefore excluded from cumulative analysis.
Cumulative Analysis of All Studies According to Technique Used to Manage the Distal Ureter
Indicates a statistically significant result.
Cumulative analysis shows that mean age was comparable between groups. There was a higher proportion of males in the open compared to laparoscopic group (P < .001) and no difference between other groups (P > .05). Only two studies reported BMI, and it was not included in the cumulative analysis. None of the studies reported performance status or ASA grade.
Tumor location, T stage, and grade were well reported throughout the studies. There was no significant difference in the laterality between groups (P > .05). The location of the tumor in the renal pelvis was significantly higher in the laparoscopic and endoscopic groups compared to the open group (P = .033 and P = .002, respectively). In addition, there was a higher proportion of patients with a tumor located in both the renal pelvis and ureter in the laparoscopic compared to the open group (P = .0019). There was no significant difference in location between the laparoscopic and endoscopic groups (P > .05).
There was a lower proportion of pT2-4 tumors in the endoscopic compared to both the open and laparoscopic groups (P = .002 and P = .033, respectively). There was no significant difference in pT stage between the open and laparoscopic groups (P > .05). However, there was a higher proportion of high grade/G3 tumors in the open compared to laparoscopic groups (P < .001) with no significant difference in tumor grade between the endoscopic and other groups (P > .05).
Nodal status and presence of CIS was poorly reported and was excluded from the cumulative analysis. In addition, the presence of lymphovascular invasion was only reported by 1 study affecting 46 patients (35.7%). 39 Architecture of the UTUC and presence of necrosis were not reported in any study.
Primary outcomes
Intravesical recurrence
All studies were reported on the rate of intravesical recurrence. The highest rate of intravesical recurrence was reported by Shigeta et al. in 67 of their 129 patients (52%) with a median follow-up of 31.1 months (range 11.7–128). 39
There was a significantly higher rate of intravesical recurrence in the open compared to both laparoscopic and endoscopic groups (P < .001 for both) (Table 5). There was no significant difference between the laparoscopic and endoscopic groups (P > .05).
Extravesical recurrence
With the exception of one study in which the primary outcome was intravesical recurrence, all of the remaining studies reported on the incidence of local extravesical recurrence. 39 Only one study identified 2 patients who developed renal bed recurrence. 41 There was no significant difference between groups in the cumulative analysis (Table 5).
All studies reported on the incidence of port-site recurrence with only 1 patient who had received a laparoscopic technique to manage the distal ureter affected. 40 In the cumulative analysis, there was no significant difference between groups (Table 5).
Distant metastases
The incidence of distant metastases was reported in 8 studies with 2 of these reporting developments of distant metastases. Simone et al., in which a laparoscopic approach was used for the distal ureter, reported that 10 of their 40 patients (25%) developed metastases; all with high grade disease on their initial pathology. 40 The study by Romero et al. contained patients undergoing both laparoscopic and open excision of the distal ureter with distant metastases developing in 3 and 1 patients, respectively. 41
Cumulative analysis identified a statistically significant higher rate of metastases in the laparoscopic compared to both the open and endoscopic groups (P < .001 and P = .042, respectively). There was no significant difference when the open and endoscopic groups were directly compared (P > .05).
Time to recurrence
Of the 6 studies that reported patients with recurrence, time to recurrence was reported by 4 studies. Shigeta et al. using an open approach to the distal ureter reported a median time for their 67 intravesical recurrences to be 19.4 months (range 1.7–102.9). 39 Gillan et al. reported the 1 recurrence in the open group to have occurred at the 6-month follow-up and 2 in the endoscopic group by the 3-month follow-up. 42 The only study reporting time to recurrence in the laparoscopic approach by Greco et al. reported a mean of 14 months in their 3 patients. 43 The relatively low incidence of recurrence in most studies and lack of reporting regarding time to recurrence prevented any further meaningful cumulative analysis of this.
Cancer-specific survival and overall survival
Cancer-specific survival and overall survival were reported in 1 study. Shigeta et al. reported a median cancer-specific survival of 29.5 months (range 2.3–147.7) and median overall survival of 35.6 months (range 6.7–147.7). 39 In this study 34 patients died and 31 deaths were a direct result of urothelial cancer. Recurrence-free survival was reported in 1 study as 75% at 5 years. 43 Only one other study reported on mortality. Romero et al. reported 1 patient death of unrelated causes at 19 months from the time of surgery in the laparoscopic group. 41
Length of follow-up
All studies reported on the length of follow-up, which ranged from 4 to 148 months. However, two studies did not divide up the different groups within their study and the length of follow-up for the particular technique of managing the distal ureter was unclear.28,42 These studies were excluded in the cumulative analysis. The cumulative analysis demonstrated comparable mean follow-up times for the open and laparoscopic groups (46.2 and 45.5 months, respectively) with a shorter duration for the endoscopic group (33.4 months) (Table 5).
Secondary outcomes
Operating time
Operating time was reported in all studies (Table 3). Cumulative analysis suggested that the mean operating time was doubled when using an open approach to the distal ureter (Table 5).
Surgical Outcomes of the Individual Studies Shown by Technique Used to Manage the Distal Ureter
EBL and blood transfusion
EBL was reported in 6 studies and was highly variable (Table 3). Cumulative analysis showed that the mean EBL was highest for the group undergoing an open approach to the distal ureter (195.6 mL) followed by endoscopic (159 mL) then laparoscopic (130.6 mL) (Table 5). Four studies reported that there were no blood transfusions and the remaining did not comment.
Length of hospital stay
Length of hospital stay was reported in 7 studies (Table 3). The cumulative analysis for length of hospital stay showed a decreased duration when using a pure laparoscopic approach (4.1 days) compared to the open (7.7 days) and endoscopic (8.9 days) approaches (Table 5).
Complications
The two studies incorporating the largest number of patients did not report whether there were any complications following surgery.39,43 Of the remaining studies, in the patients who underwent an open approach to excision of the distal ureter, one reported no major complications but did not comment on any minor complications. 46 The remaining two studies from Romero et al. and Gillan et al. reported 2 unspecified complications and 1 wound infection, respectively.41,42 For the patients undergoing a laparoscopic approach, three studies reported no complications.40,42,45 One study reported 3 complications but did not provide detail on their nature. 41 One study using an endoscopic approach reported 1 wound infection. 28 The remaining 2 studies using an endoscopic approach reported no complications.42,44 There was no significant difference in the rate of complications between groups (P > .05) (Table 5).
Positive surgical margins
Six studies reported on positive surgical margins (Table 3). Two of the studies that did not report this contributed 144 patients to the open group leaving only 24 patients, in which the outcome was known with no reported positive surgical margins. There were 3 reports of positive surgical margins in the laparoscopic group in patients with renal pelvis urothelial carcinoma. 41 There was 1 report of positive surgical margins in an endoscopic group for a patient with a ureteric tumor. 42 There was no statistically significant difference between groups (P > .05) (Table 5).
Discussion
Management of the distal ureter during LNU for UTUC is a controversial issue. In this review, we have compared the outcomes of patients undergoing LNU using an open, laparoscopic, or endoscopic approach to excise the distal ureter and bladder cuff. The cumulative analysis has suggested potential differences in oncological outcomes, finding a higher intravesical recurrence rate using an open approach and distant metastases using a laparoscopic approach.
The finding of a higher intravesical recurrence rate in the open group was mainly contributed to by one study affecting 67 (52%) of their patients. 39 Other reports in the literature, not eligible for inclusion here, have found similarly high rates of intravesical recurrence using an open approach.10,47,48 However, there are likely to be additional factors that have contributed to this. First, it was unclear whether the ureter was clamped before mobilization and theoretically this could allow seeding of tumor cells. In addition, only 33 patients in this study received intravesical chemotherapy, which has been proved to reduce the risk of intravesical recurrence after nephroureterectomy. 49 The open group also had a higher proportion of tumors located in the ureter, which has been suggested as a risk factor for intravesical recurrence due to its close anatomical location.48,50,51 Furthermore, in the open group there was a significantly higher proportion of pT2-4 tumors than the endoscopic group and a higher proportion of high grade/G3 tumors than the laparoscopic group. Both factors are poor prognostic indicators in UTUC. 31 Therefore, it is likely that the higher intravesical recurrence rate found using the open approach is due to a combination of factors rather than solely the technique of managing the distal ureter.
The significantly higher rate of distant metastases in the laparoscopic group is more concerning given the comparable pT stage and lower grade of tumor when compared to the open group. This must, however, be taken with caution as the largest study in the open group (n = 129) did not report on the incidence of distant metastases and could not be included in the cumulative analysis. 39 However, this study did report 31 deaths relating to urothelial cancer. Clearly these may have involved distant metastases, and had this been reported, there may not have been a significant difference between the laparoscopic and open groups. Furthermore, the follow-up protocol, including the use of upper tract imaging, was not universally reported and it is unclear how some studies reporting no recurrence determined this.
Interestingly, in this review, the endoscopic group did not show any significant difference in the rate of recurrence or development of metastases and no difference in tumor grade compared with the other groups. However, compared to the other groups the endoscopic group did have a lower proportion of pT2-4 tumors, an overall smaller number of patients and a shorter duration of follow-up.
One of earliest resistances to laparoscopic surgery for malignancies was the reported risk of port-site metastases up to 21% in some series. 52 A review performed in 2012 demonstrated the overall rate of port-site metastases in laparoscopic surgery to be comparable to the rate of open surgical wound metastases. 53 Despite this, the topic is still frequently discussed. In this review, among all studies, there was only 1 occurrence of port-site metastases. 40 The overall low incidence again demonstrates that LNU can be safely performed.
The rate of positive surgical margins in the cumulative analysis for all groups was low and in keeping with a previous review. 54 In addition, there were no reports of recurrences at the ureteric orifice resection site demonstrating the general ability of all approaches to successfully and safely excise the distal ureter. Although one laparoscopic technique in which a gastrointestinal stapling device was used to divide and excise, the distal ureter does raise concern. 41 In this group, 25% had positive surgical margins, 50% developed intravesical recurrence, 17% renal bed recurrence, and 25% distant metastases. This was higher than any of the other studies included in this review, and a previous review has also raised concerns about the high rate of positive surgical margins when stapling devices are used. 55 However, it is important to note that in this single study, there was a relatively low number of patients (n = 12), with a high proportion of patients with pT2-4 and high-grade disease (70% and 83.3%, respectively). 41
The cumulative analysis suggested that operating time was double using an open approach to the distal ureter. This is difficult to explain, and it is likely that the result has been skewed by the contribution of one large study reporting an extensive range for operating time with the longest taking over 15 hours. 39 This is substantially higher than other studies in this review and in the literature. One of the earliest published case series when one would expect a longer operating time as the procedure is being learnt reported their longest LNU taking 10.6 hours. 56 Interestingly, the endoscopic group, which requires the patient to be repositioned from the lithotomy to lateral position, had the lowest mean operating time suggesting that repositioning does not negatively impact operating time.
The length of hospital stay was found to be shortest using a pure laparoscopic approach when compared to open and endoscopic. However, differences in the clinical practice from the country of origin are likely to influence this. Two of the studies from China reported that it is standard practice for the patient to remain in hospital until the catheter is removed, which is typically 1 week or more after surgery.28,46
This review has attempted to address the current contentious issue of management of the distal ureter through a thorough systematic approach with strict methodology. However, it does have several limitations. Many of the studies are of a low level of evidence with 4 studies being case series from a single center. The critical appraisal process was designed to prevent the inclusion of poorer quality studies. However, it does potentially open the study to selection bias. It has already been discussed that the lack of clearly defined follow-up protocols particularly with 4 studies not specifying their use of upper tract imaging also expose these studies to observer bias. The total number of patients and studies eligible for inclusion in this review is less than the two previous reviews on distal ureter management.54,55 However, this is the only review to compare open to laparoscopic and endoscopic techniques. In addition, the design of this review attempted to provide better control for potential confounding factors.
There is a vast amount of research into LNU for UTUC, which is mostly focused on its comparisons to ONU. Unfortunately, much of this cannot be used to assess the technique to manage the distal ureter as it was not reported or multiple techniques were used and analysis was performed in combination. Even in the included studies, there was a significant lack of reporting on what could be potentially confounding factors making the results difficult to interpret. Further research will need to address this more closely to assess the implications of technique on oncological outcomes for LNU in UTUC.
Conclusion
Distal ureter management in UTUC is one of many risk factors and controversies in a complex condition. In this review comparisons between open, laparoscopic, and endoscopic approaches to managing the distal ureter have been made. Findings of a higher intravesical recurrence rate using an open approach and distant metastases using a laparoscopic approach, although of concern, are difficult to interpret due to the number of potential confounding factors. Due to the heterogeneity of studies, it is not possible to identify any superior method to manage the distal ureter, and there is a need for further empirical research to address this controversial topic.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.
Appendix
Search Straregy
| 1 | urothelial (Title/Abstract) |
| 2 | transitional cell (Title/Abstract) |
| 3 | carcinoma (Title/Abstract) |
| 4 | cancer (Title/Abstract) |
| 5 | upper urinary tract (Title/Abstract) |
| 6 | upper tract (Title/Abstract) |
| 7 | kidney (Title/Abstract) |
| 8 | renal (Title/Abstract) |
| 9 | renal pelvis (Title/Abstract) |
| 10 | ureter* (Title/Abstract) |
| 11 | 1 OR 2 |
| 12 | 3 OR 4 |
| 13 | 5 OR 6 OR 7 OR 8 OR 9 OR 10 |
| 14 | 11 AND 12 AND 13 |
| 15 | nephroureterectomy (Title/Abstract) |
| 16 | nephro-ureterectomy (Title/Abstract) |
| 17 | laparoscop* (Title/Abstract) |
| 18 | robot-assisted (Title/Abstract) |
| 19 | robot assisted (Title/Abstract) |
| 20 | 15 OR 16 |
| 21 | 17 OR 18 OR 19 |
| 22 | 20 AND 21 |
| 23 | recurrence (Title/Abstract) |
| 24 | mortality (Title/Abstract) |
| 25 | survival (Title/Abstract) |
| 26 | 23 OR 24 OR 25 |
| 27 | 14 AND 22 AND 26 |
| 28 | English (Language) |
| 29 | Date (January 1991–June 2019) |
| 30 | 27 AND 28 AND 29 |