
Abstract
Endoscopic retrograde cholangiopancreatography (ERCP) is the minimally invasive standard of care for the treatment of several biliary and pancreatic pathologies. One of the limitations of this technique is the lack of endoluminal vision within the biliary tree or Wirsung's duct. This limits the diagnostic accuracy of the procedure and reduces the effectiveness of many treatments. Technological progress and the use of increasingly ergonomic and high-definition imaging equipment have led to the dissemination of peroral cholangioscopy (POC). Thanks to the high quality of video image resolution, POC could well be a powerful tool used to characterize malignant biliary strictures. It could also allow targeted biopsies or local treatments, hence reducing the risk of complications and increasing outcomes. The technological improvement of the last generation of POC is opening new horizons in the treatment of biliopancreatic pathologies, thereby contributing to refine and enhance the ERCP management of several diseases in the near future.
Introduction
The advent of the digital era has encouraged the development of minimally invasive techniques in the surgical field with the use of cutting-edge, high-performance technology. The need to work with systems which improve real-time optical diagnosis reproducing images of high quality and definition has also become essential in the area of digestive endoscopy.
Endoscopic retrograde cholangiopancreatography (ERCP) is an endoscopic interventional procedure, which allows the treatment and diagnosis of several biliopancreatic conditions. The procedure is performed under fluoroscopic guidance. The biliary tree is examined by carefully injecting a contrast medium, and specific radiopaque devices are used to perform the intervention under X-ray assistance. However, fluoroscopic imaging is limited by a two-dimensional (2D) visualization and it merely provides partial and indirect information about the presence of abnormalities inside biliary and pancreatic ducts. Moreover, the cannulation of the biliary tract or of Wirsung's duct can be troublesome and time consuming, exposing patients and operators to high doses of radiation. This is especially true for complex cases and nonexperienced operators.
To overcome such limitations, newer fluoroscopic units have been equipped with a 180° rotation c-arm computed tomography (CT) for real-time 3D image rendering (Fig. 1). The first case series describing the clinical use of 3D-ERCP with cone-beam CT was published in 2015. Authors demonstrated a high level of accuracy of 3D-ERCP in the diagnosis of stenosis and biliary leak. 1 Additionally, the correct understanding of the tridimensional orientation of the biliary tree and pancreatic duct at the beginning of the intervention is extremely useful to enhance the operator's perception of the anatomy and facilitate the technical gesture, making the image-guided procedure faster and less complex.

3D-ERCP:
Another strategy included the rendering of different imaging modalities (preprocedural 3D magnetic resonance imaging images with real-time 2D fluoroscopic images at the time of ERCP) to obtain a 3D roadmap of the biliary tree. 2 This technique, called bimodal ERCP, helped to enhance the fluoroscopic visualization of the lesion of interest and the understanding of ductal anatomy. However, despite the use of the most sophisticated and advanced radiological imaging techniques, these modalities can provide only indirect visualization of intraductal pathologies.
The possibility to directly inspect the ducts through an endoluminal vision would undeniably allow targeted and extremely precise procedures, reducing the risk of complications.
Since the 1970s, peroral cholangioscopy (POC) has been advocated as a means to navigate biliary and pancreatic tracts under direct endoscopic view.3,4 The technological evolution has made cholangioscopes more and more sophisticated, highly performant, and handy to use, contributing to their widespread and increased fields of application. Currently, three different techniques to perform POC are available, that is, dual-operator technique with mother/baby system, direct cholangioscopy, and single-operator cholangioscopy.
Cholangioscopy Techniques
The mother/baby cholangioscopy was the first platform to be developed. It consists of a two-way tip deflection cholangioscope (baby) inserted into the operative channel of a duodenoscope (mother) (Fig. 2). The first POC was bulky and had a fiber-optic system with poor image quality. Over the years, this model has been replaced with POC with smaller diameters and better-quality digital images. 5 The advent of narrow-band imaging in flexible endoscopy allowed the magnification of biliary surface structure and microvessels.6,7 Despite such improvements, the fragility of the baby cholangioscope and the high repair costs have limited the dissemination of this technology.
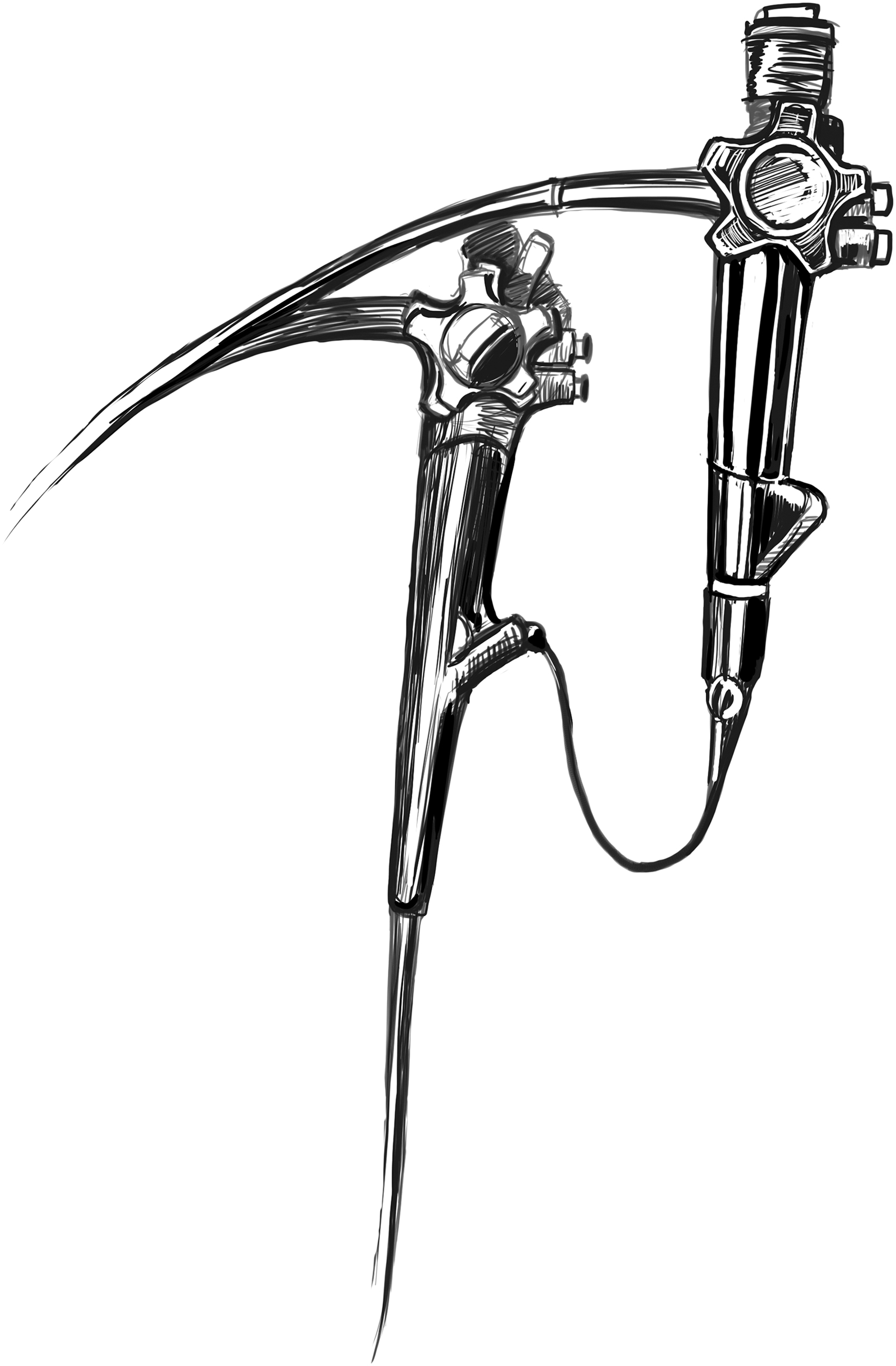
Mother/baby cholangioscope.
Direct POC is performed by directly inserting an ultra-slim endoscope into the common bile duct (CBD) (Fig. 3). Advantages of direct POC include high-resolution image quality, availability of electronic chromoendoscopy, and a large working channel (2.2 mm). However, the procedure is extremely challenging, hence reducing the dissemination of the technique. 8 There are several elements which increase the technical difficulty of the intervention, such as the instability of the ultra-slim endoscope within the biliary tree, the facility in gastric looping formation, the complexity in biliary cannulation, and the diameter of the scope that cannot access the nondilated CBD. 9 In 2020, Lee et al. performed a prospective randomized controlled clinical trial comparing a new multibending (MB) ultra-slim endoscope with a conventional ultra-slim endoscope for the free-hand insertion of an endoscope into the CBD. They demonstrated that the MB ultra-slim endoscope had a high technical success rate (89% versus 30.4%, P < .001) without severe adverse events and it effectively decreased procedure time as compared with a conventional ultra-slim endoscope. 10
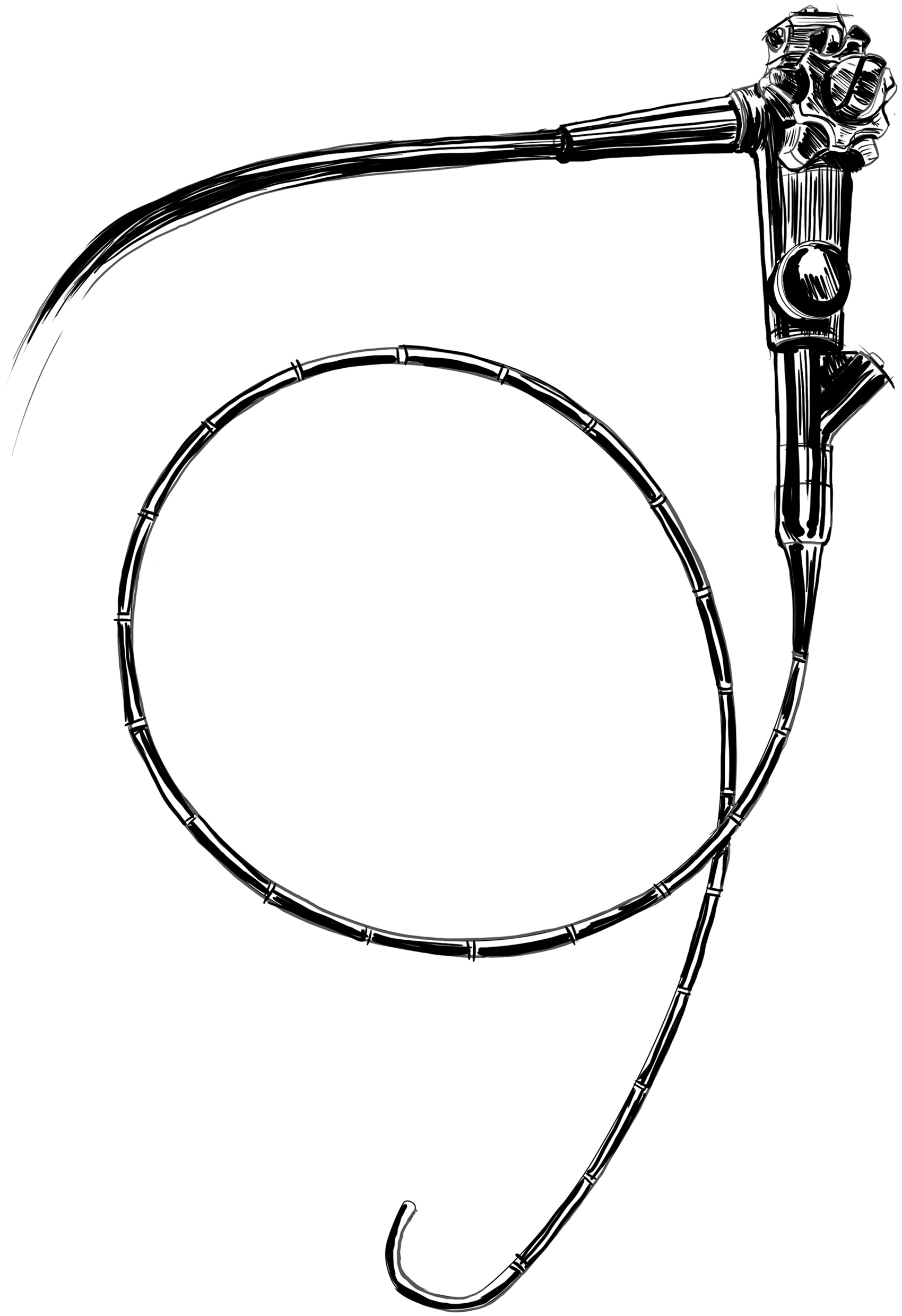
Direct cholangioscope.
Single-operator POC was described for the first time in 2005 11 (Fig. 4). The SpyGlass system (Boston Scientific Corporation, Marlborough, MA) had several advantages over the previous POC. The handle of the disposable delivery catheter was mounted directly onto the duodenoscope handle, allowing for a single-operator procedure. In addition, the catheter could achieve a four-way deflected steering within the bile duct, making the procedure easier and faster. Moreover, two dedicated irrigation channels ensured a sustained continuous irrigation. On the other hand, the reusable optical probe generated low-quality images and was fragile, lasting about 3 to 4 times. These limitations, combined with the small diameter of the operating channel, reduced its use and diffusion.
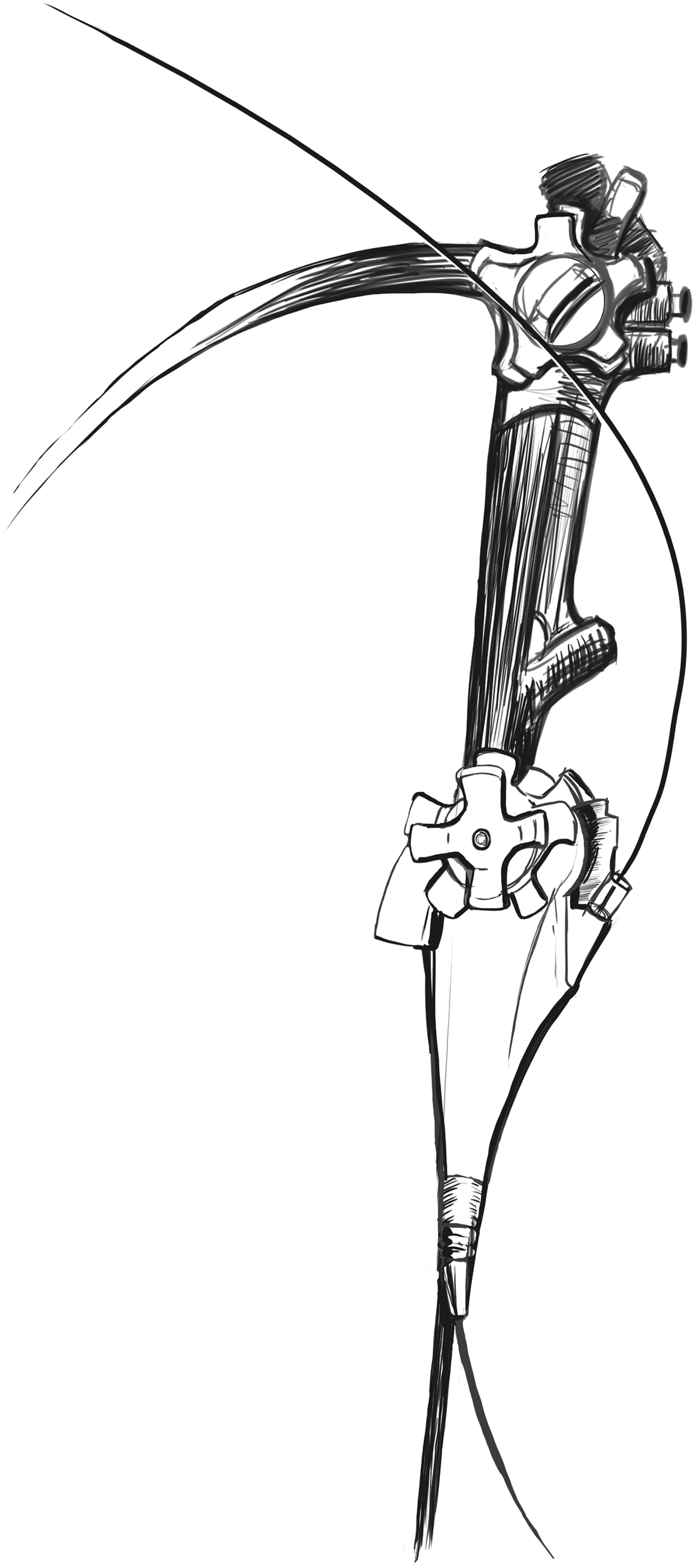
Single-operator cholangioscope.
The second-generation SpyGlass DS (Boston Scientific Corporation) was developed in 2015. The fully disposable system had significant improvements, including digital image quality, a wider field of view (110 versus 70), a redesigned working channel, a brighter light source, and an easy “plug-and-play” set-up. 12 In 2018, Boston Scientific upgraded the SpyGlass system to a third generation system called the SpyGlass DS II. This new platform features an increased resolution, at 2.5 × that of the SpyScope™ DS, and adjusted lighting to provide visibility. Additionally, a brand-new SpyGlass retrieval basket and a SpyGlass retrieval snare were launched with the SpyGlass DS II. In 2020, a new SpyBite Max Biopsy Forceps was developed to acquire more than 2X tissue in an average bite with respect to the legacy SpyBite biopsy forceps.
All technical improvements and upgrading in terms of image quality, maneuverability, diagnostic, and therapeutic potential have increased the SpyGlass popularity among the scientific community, contributing to the recognition of POC as a recommended procedure for several indications.
Indications for POC
Common indications for POC include removal of difficult biliary stones performing visually guided electrohydraulic lithotripsy (EHL) and laser lithotripsy (LL), evaluation of biliary strictures, and histological characterization of endobiliary lesions. Moreover, POC is used to guide targeted ablation of endoluminal biliary tumors and facilitating guidewire or device access across narrow biliary strictures. The cholangioscope can also be employed to perform pancreatoscopy for the treatment of several pancreatic pathologies.
Difficult management of bile duct stones
The most common therapeutic indication for POC is difficult CBD stone extraction 13 (Fig. 5). Biliary stones are defined as difficult to treat according to their diameter (>1.5 cm), thickness, number, shape, location (intrahepatic, cystic), or depending on anatomical factors (e.g., stone impaction, distal CBD angulation <135°). 14 POC allows for a direct visualization of the stone and a consequent guided lithotripsy. After stone fragmentation and debris extraction, clearance of the biliary tree is assessed by means of endoluminal inspection, hence reducing the risk of stone recurrence (Fig. 6). Technical success rates of POC lithotripsy is 71% to 100%.15–18
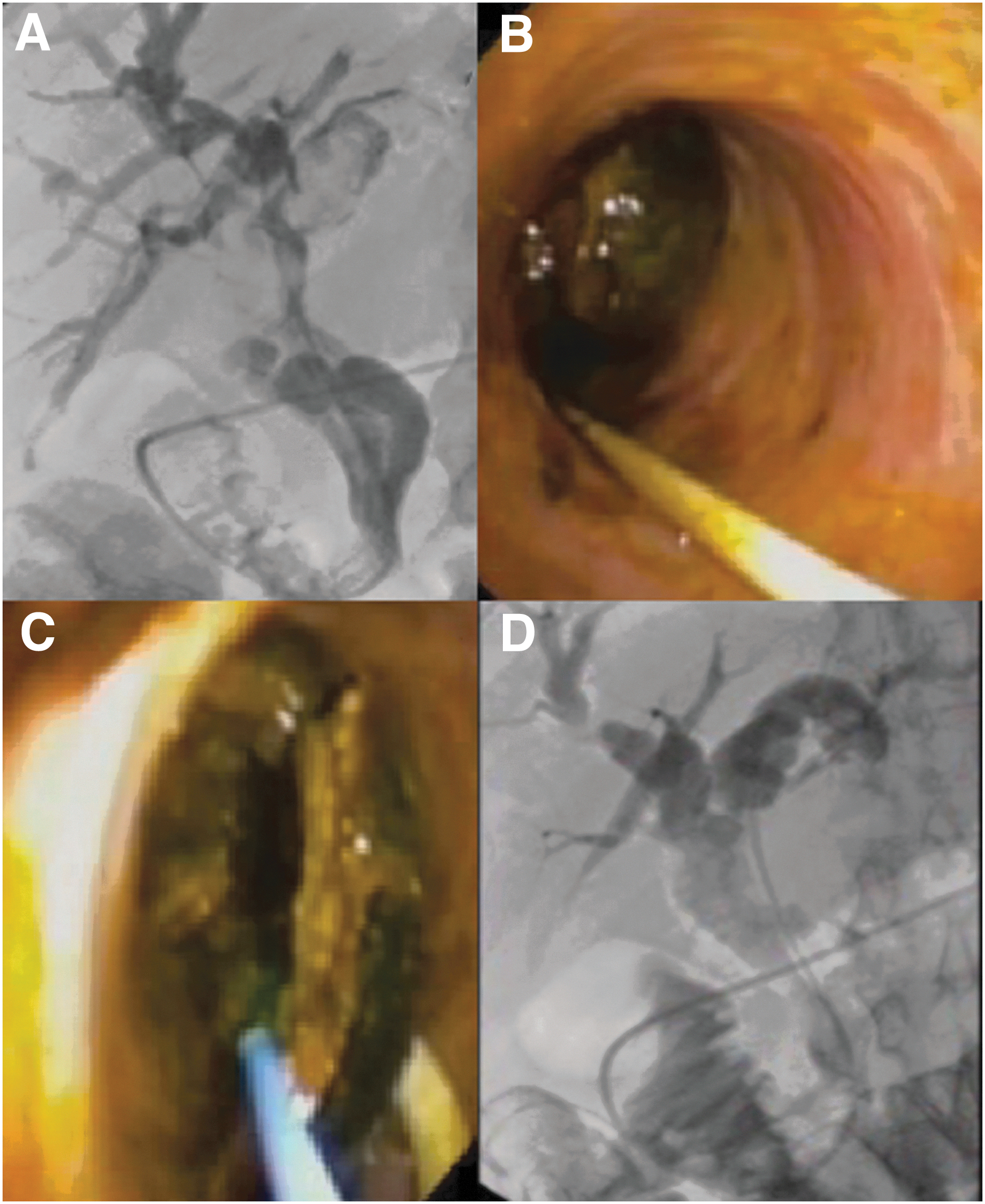
Direct cholangioscopy:

Single-operator cholangioscopy using the SpyGlass™ DS I system to treat Mirizzi's syndrome.
A multicenter retrospective study by Gutierrez et al. compared digital single-operator EHL with LL, reporting a 96.7% success rate with EHL and a 99% success rate with LL. Procedure time was reported to be lower in the LL group as compared with the EHL group (49.9 versus 73.9 minutes on average). In a randomized trial, cholangioscopy-guided laser lithotripsy increases the incidence of endoscopic clearance of large bile duct stones (93% versus 67%, P = .009) and decreases the need for surgery as compared with conventional therapy alone. 19
Characterization of endoluminal biliary lesions and strictures
The evaluation of bile duct strictures during an ERCP procedure has a significant imaging limitation. The diagnosis of endoluminal lesions using fluoroscopy is not accurate and can lead to the risk of a missed pathology and errors. Brush cytology and fluoroscopy-guided biopsy during ERCP have very limited sensitivity in diagnosing malignant biliary strictures (45%–48%) even when combined (54%). 20 Additionally, before placing an uncovered self-expandable metal stent (SEMS) to treat a biliary stenosis, the anatomopathological diagnosis should be required. Direct visualization of intraductal biliary lesions or strictures with targeted biopsy is one of the main applications of POC.
The use of increasingly sophisticated and high-quality systems to explore the endobiliary tract drove some authors to characterize the cholangioscopic appearance of benign and malignant intrabiliary lesions.21,22 Typically, tortuous and dilated vessels, infiltrative strictures, and fish-egg lesions were more likely to be malignant. Conversely, lesions with smooth mucosa and no abnormal vessels were supposed to be benign. In 2018, Robles-Medranda et al. proposed a new classification system based on neoplastic and non-neoplastic findings on cholangioscopy, which presented a high reproducibility among observers. 23
Recently, in a systematic review, Kulpatcharapong et al. 24 have analyzed the diagnostic performance of the different POCs to characterize biliary strictures. The authors concluded that POCs have a high performance to diagnose malignant biliary strictures, with a majority of studies showing a sensitivity higher than 70% and a specificity higher than 80%. Digital single-operator POC and direct POC have a higher sensitivity, specificity, and accuracy than digital dual-operator POC (80%–90%, 89%–100%, and 87%–93%, respectively, for digital single-operator POC; 78%–100%, 73%–100%, and 75%–93%, respectively, for direct POC; 38%–100%, 49%–100%, and 50%–100%, respectively, for digital dual-operator POC).
Globally, diagnosis made under visual impression had higher sensitivities than POC-guided biopsy (67%–100% versus 38%–100%) whereas the overall specificities were comparable (73%–100% versus 75%–100%). These data show that POC is a good tool for the visual and onsite characterization of endobiliary lesions. However, biopsy sampling with the 3 mm SpyBite forceps does not guarantee an accurate histological diagnosis. The new Max SpyBite forceps was redesigned to acquire biopsies of larger dimension. Nevertheless, due to the novelty of the device, there are still no study assessing its efficacy at present.
Ablation therapies
Cholangiography could allow targeted radiofrequency ablation (RFA) of endoluminal tumors under direct vision, hence reducing the risks associated with the standard ERCP-RFA therapy under fluoroscopic guidance. 25 In a retrospective study performed in 12 patients with SEMS ingrowth for malignant biliary tumors, the authors described the effects of RFA under POC guidance, 26 demonstrating a 100% technical success rate and only one postprocedure cholangitis.
Pancreatic diseases
Peroral pancreatoscopy (POP) could be useful to diagnose intraductal papillary mucinous neoplasm, evaluate strictures of the pancreatic duct, and treat pancreatic stones using LL or EHL.27,28 The two methods of POP are the mother/baby and the single-operator technique. Pancreatic sphincterotomy of the major or the minor papilla is generally required to access Wirsung's duct with the scope. 29 In a recent 13-year experience study, the visual diagnosis of pancreatic neoplasm had a sensitivity, specificity, and accuracy of 87%, 86%, and 87%, respectively. 30
In contrast, tissue sampling through POP is technically challenging, mainly because it reduces the maneuverability of the small biopsy forceps in the narrow pancreatic duct. Lithotripsy and removal of pancreatic stones could be performed under direct guidance when other options have failed or are not available. Recent reports on EHL and LL or mechanical lithotripsy under POP guidance demonstrated a complete stone clearance rate superior to 80%.31,32
Other clinical applications
Improvement in technical characteristics and performance of new cholangioscopes have broadened the range of applications of this cutting-edge technology, which is now easily accessible. The use of cholangioscopy through a percutaneous approach has been increasingly described in the literature.33,34 In addition, POC is used as a visual guide to pass the guidewire through a tight biliary tract stenosis, not accessible under fluoroscopic guidance.35,36 Cases when the SpyGlass was used through a hepaticogastrostomy after EUS-guided biliary drainage had also been described. 37 Other reported applications include hemobilia, 38 gallbladder drainage through the cystic duct, 39 and foreign body removal from the bile duct. 40
Safety
POC is generally considered a safe procedure with a very low rate of serious events (1%, 95% CI: 1%–2%). 41 The most frequently described complication is cholangitis typically associated with ductal irrigation.15,42 Limited cases of postprocedural pancreatitis, hemobilia, and bile leaks usually related to EHL/LL have also been reported. 43 Rare complications, including air embolization could be potentially lethal, thereby strongly recommending the routine use of carbon dioxide during the procedure.44,45
Conclusions
The incredible technological evolution investing the field of flexible endoscopy is leading to a revolution in the treatment of biliopancreatic pathologies. Currently, several methods, such as 3D-ERCP and bimodal ERCP, are using the most cutting-edge imaging modalities to obtain the best anatomical reconstruction of the biliary tree and of the pancreatic duct to facilitate the procedure, reducing complications. Cholangiopancreatoscopy allows for the direct endoluminal visualization of the CBD and of Wirsung's duct. Thanks to the progress of new single-operator cholangioscopes and the introduction of increasingly sophisticated devices, this technology is gaining popularity. The chance to visualize intraductal abnormalities and to perform targeted and controlled treatments opens the field to new diagnostic and therapeutic possibilities, which will certainly be increasingly investigated in the near future.
Footnotes
Acknowledgments
Authors are grateful to Guy Temporal and Christopher Burel professional in medical English proofreading, for their valuable help in revising the article. Authors thank Catherine Cers for illustrations.
Disclosure Statement
M.P. and S.P. have no conflicts of interest or financial ties to disclose. I.B. is consultant for Cook Medical, Apollo Endosurgery, Boston Scientific, and has a research grant from Apollo Endosurgery.
Funding Information
No funding was received for this study.