
Abstract
Introduction:
Emergency departments (EDs) during the novel coronavirus disease 2019 (COVID-19) pandemic are perceived as possible sources of infection. The effects of COVID-19 on patients presenting to the hospital with surgical complaints remain uncertain.
Methods:
A single tertiary center retrospective study analysis compared the ED attendance rate and severity of patients with surgical complaints between March 2020 (COVID-19 outbreak) and pre-COVID-19 periods: February 2020 and the same 2 months in 2019 and 2018.
Results:
Overall, 6,017 patients were included. The mean daily ED visits of patients with nontrauma surgical complaints in the COVID-19 outbreak period declined by 27%–32% (P value <.01) compared with pre-COVID-19 periods. The log number of confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) cases in Israel in March 2020 was negatively correlated with the number of ED visits (Pearson's r = −0.59, P < .01). The proportion of patients requiring hospitalization increased by up to 8% during the outbreak period (P < .01), and there was a higher proportion of tachycardic patients (20% versus 15.5%, P = .01). The percentage of visits to the ED by men declined by 5% (P < .01). The ED diagnosis distribution significantly changed during COVID-19 (P = .013), with an 84% decrease in the number of patients hospitalized for diverticular disease (P < .05).
Conclusion:
During the COVID-19 outbreak, the overall number of patients presenting at the ED with surgical complaints decreased significantly, and there was a higher admissions ratio. The extent to which the pandemic affects hospital ED attendance can help health care professionals prepare for future such events. ClinicalTrials.gov ID: NCT04338672
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and associated novel coronavirus disease 2019 (COVID-19) pose a catastrophic threat to public health worldwide. Since the beginning of the pandemic (December 2019), data on its effect on health care systems prompted recommendations for social distancing and quarantine decrees issued by local governments. 1 These measures, together with the public fear of the spread of the virus, are presumed to have markedly affected the number of noncoronavirus-related hospital emergency department (ED) visits.2,3
EDs play an important role in controlling the pandemic, but are also perceived as hotspots for infection due to the high risk of exposure. Previous experience from the 2003 SARS outbreaks in Hong Kong, Taiwan, and Toronto that documented reduced ED visits by up to 50%4–6 suggests that people are reluctant to come to the ED for nonrespiratory symptoms or defer the visit for as long as possible. The result can be an exacerbated clinical course that may put them at increased risk for morbidity and mortality, especially those with surgical emergencies, for whom delaying medical attention can be fatal. Evaluating the extent to which the pandemic affects hospital attendance volume can help health care systems prepare for future such events. This is of the utmost importance in light of the forecasted second wave of COVID-19. 7
The aim of this study was to investigate the impact of the COVID-19 pandemic on the arrival of people with surgical complaints to a tertiary hospital ED. We hypothesize that during the COVID-19 pandemic, the number of people requiring surgical consultations will decline, whereas those who do appear will come with more severe presentations.
Materials and Methods
Study design
In this retrospective study, the medical records of patients presenting at our ED with complaints requiring a surgical consult between February 1 and March 31 in 2018, 2019, and 2020 were reviewed. March 2020 is defined as the COVID-19 outbreak period, with pre-COVID-19 periods consisting of February 2020 and February–March 2019 and 2018 (Clinical-Trials.gov ID: NCT04338672). The attendance trends were compared in all 6 months, whereas the clinicopathological characteristics were compared between March 2020 and March 2018 and 2019.
Inclusion criteria included patients presenting with chief complaints that deemed a general surgical consult in our ED: anal pain, abdominal pain, abscess, constipation, gastrointestinal hemorrhage, hemorrhoids, postsurgical complaints, proctological complaints, surgical site infection, and suspected obstruction. These chief complaints are filled by the ED triage nurse upon initial arrival of the patient. Patients <18 years of age and trauma patients were excluded. Post hoc analyses included analyzing the number of appendectomies in our institution during the study periods.
Measurements
Data collected included the daily number of patients, their clinical–pathological characteristics, diagnoses in the ED according to International Classification of Disease, Ninth Edition, Clinical Modification (ICD-9) format, and time in the ED. The severity of presentation was assessed using the emergency severity index (ESI), 8 vital signs, laboratory value (white blood count [WBC]), the need for hospital admission, and 7-day mortality. A total of 431 different ICD-9 diagnoses were evaluated. We classified these into 143 mutually exclusive clinical groups using the Agency for Healthcare Research and Quality Clinical Classifications Software (CCS), 9 which organizes ICD-9 diagnosis codes into clinically homogeneous groups.
Essential background
Israel has universal health coverage, enacted under a National Health Insurance (NHI) law. Furthermore, emergency care is made available to all individuals, including individuals without health insurance, such as undocumented migrants. The Sheba Medical Center is an academic tertiary center that has ∼1900 beds with two general surgery wards consisting of 120 beds. It is the largest hospital in Israel. The first COVID-19 patients diagnosed in Israel on February 21, 2020, were travelers returning from the Diamond Princess cruise ship off the coast of Japan. 10 The Sheba Medical Center admitted these patients and became the first medical facility in Israel to treat COVID-19 patients. We examined the number of confirmed SARS-CoV-2 infections in Israel and the critical government measures enacted during the outbreak of COVID-19 in an effort to provide context in which the outbreak was occurring. 11
Statistical analysis
Data were analyzed using R software for statistical computing (R-Project, version 3.4.1, 2017). We performed the Fisher exact test for comparison of categorical values and Wilcoxon rank sum test for continuous values. The chi-square (χ2) test with Yate's continuity correction was used for analyzing difference in the distribution of diagnosis. The correlation assessment of daily ED visits for surgical complaints and confirmed SARS-CoV-2 infected cases in Israel was calculated using the Pearson correlation coefficient (rpears). Referred reference values for strength of effect size were “very weak” 0.00–0.19, “weak” 0.20–0.39, “moderate” 0.40–0.59, “strong” 0.60–0.79, and “very strong” 0.80–1. 12 Statistical significance was set at P < .05. Data on ED attendance are presented as mean ± standard deviation.
Patient confidentiality was preserved by deidentifying health records. The study was approved by the Sheba Medical Center Institutional Review Board (Approval No. SMC-4025-17).
Results
A total of 6,017 patient records were reviewed. The mean daily number of people who presented at the ED with nontrauma complaints that necessitated a surgical consult declined by 32% and 27% in the COVID-19 period, March 2020 (25 ± 10), compared with the same period in 2019 (37 ± 13; P < .001) and 2018 (34 ± 14, P < .001), respectively. The results were strengthened when we compared the mean daily attendance in February 2020, just before the outbreak period, with that in February 2019 and with that in the outbreak period (March 2020): February 2020 (36 ± 11) was similar to February 2019 (36 ± 10; P = .88) and significantly higher than the outbreak period (P = .001). Daily ED attendance data in the 6 months reviewed in the study are presented in Table 1, and a comparison of daily attendance throughout March 2018–2020 is shown in Figure 1. The number of confirmed SARS-CoV-2 infected cases and the government measures enacted during the outbreak period are also presented in Figure 1. During the outbreak in March 2020, the number of confirmed cases of SARS-CoV-2 in Israel (in log scale) had a moderate negative correlation with the number of ED visits of our cohort (rpears = −0.59, P < .001), as shown in Figure 2.
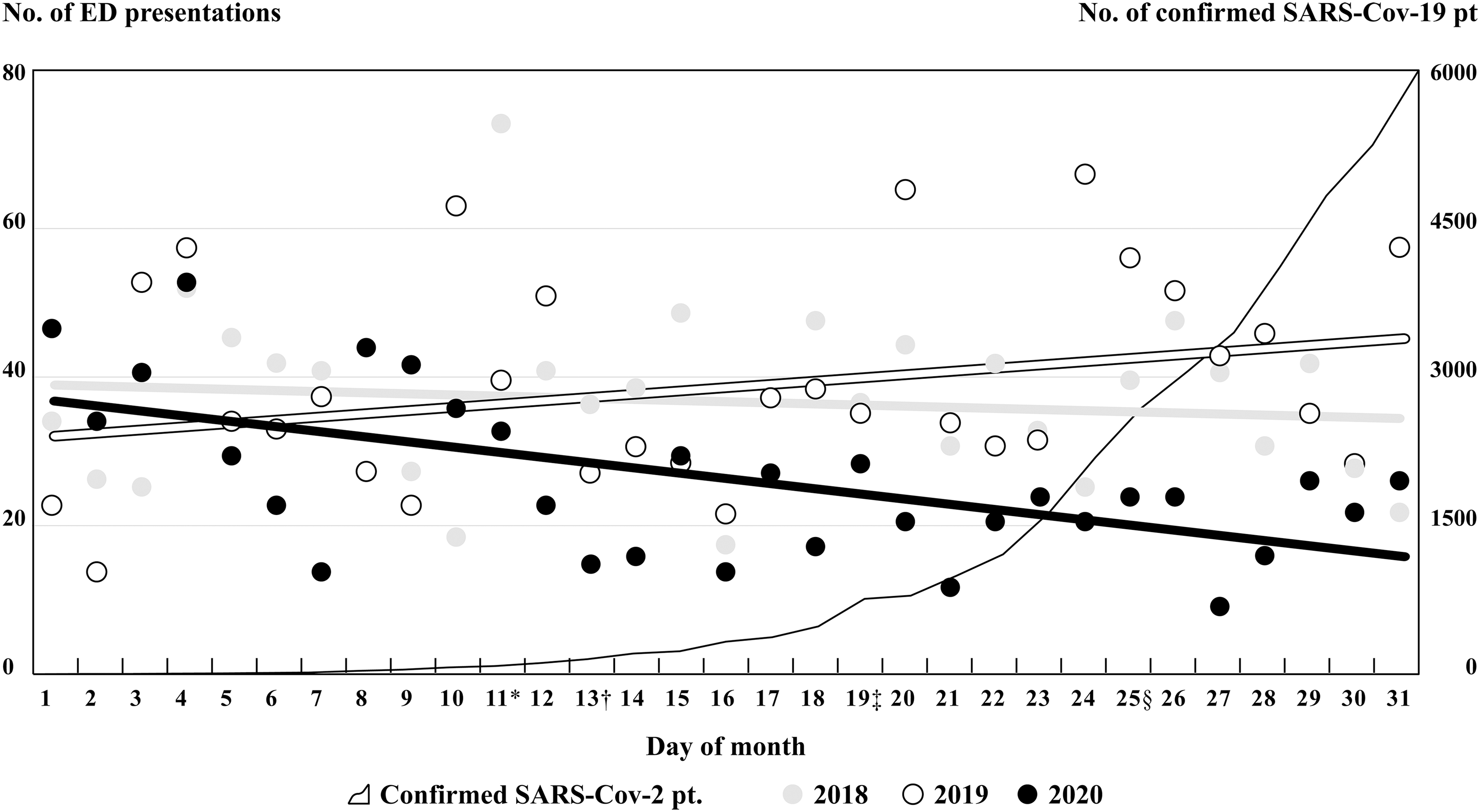
Daily number of patients presenting with surgical complaints in a tertiary hospital ED between March 1 and 31 for the years 2018, 2019, and 2020, and the daily diagnosed cases of SARS-CoV-2 in Israel during the outbreak of March 2020. Linear regression analysis shows a negative relationship between March 2020 ED attendance and the days of the month (r2 = 0.28, P value <.001). There was a 32% and 27% decrease in the mean daily number of attendees when comparing 2020 with 2019 and 2018, respectively (P < .001). Official Israeli government declarations/measures are marked adjacent to the date of issue/implementation: *limitation on visitors in hospitals; †closer to schools and universities; ‡official call to stay at home; §official decree restricting out-of-house movement. No.: number; pt.: patients. ED, emergency department; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
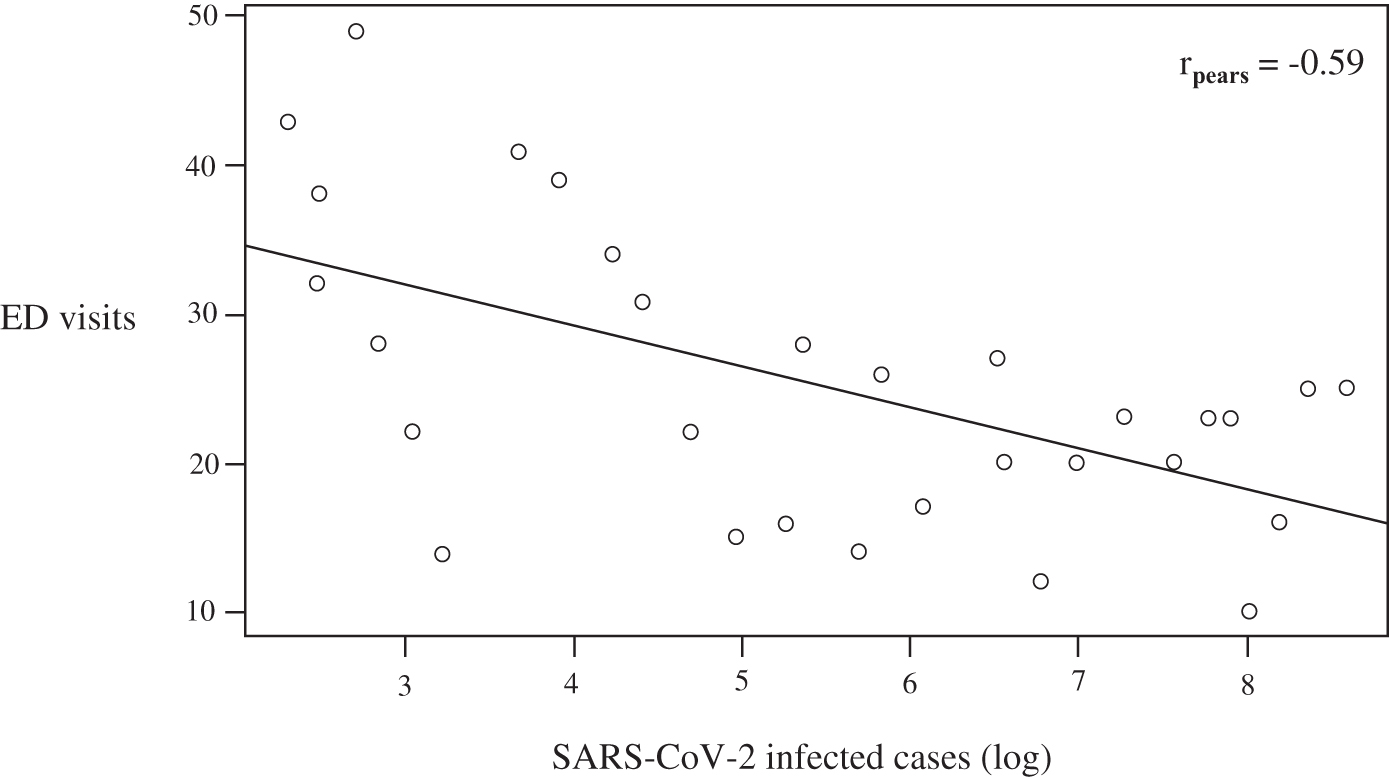
Correlation of daily ED visits with surgical complaints and log confirmed cases of SARS-CoV-2. Pearson correlation coefficient (rpears) = −0.59, P < .001. ED, emergency department; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Emergency Department Visits of Patients with Surgical Conditions During February and March of the 3 Study Years (2018, 2019, and 2020)
Data presented as mean number (n) of daily cases and SD. The percentage of change (Δ) in the novel COVID-19 outbreak period in Israel (March 2020) is calculated relative to the preoutbreak corresponding month in 2019 and 2018. Statistical significance was calculated using Wilcoxon test.
COVID-19, coronavirus disease 2019; SA, standard deviation.
Table 2 presents the clinical characteristics and outcomes of surgical patients attending the ED in March 2020 compared with the corresponding periods in previous years. The admissions proportion increased by 6% in 2020 compared with the averages in 2019 and 2018 (P = .01). There was also a larger proportion of patients presenting with tachycardia (heart rate ≥100 beats per minute), P = .01. Other significant results include a higher share of female patients (increase of 5%, P = .03) and patients with an oncological comorbidity (increase of 6.5%, P < .001). The mean time in the ED for each patient was 42 minutes less in March 2020 (5.7 ± 3.7 hours) compared with the average of March 2019 (6.2 ± 3.6 hours) and 2018 (6.6 ± 3.6 hours) P < .001. There was no statistically significant correlation between outcomes and other clinical characteristics, including age, ESI, fever, pain, WBC, cardiovascular, respiratory and renal comorbidity, smoking status, and 7-day mortality.
Clinical Characteristics and Outcomes of Patients with Surgical Complaints Attending the Emergency Department in March 2020 (Coronavirus Disease 2019 Outbreak Period) Compared with the Corresponding Periods in Previous Years
The percentage changes (Δ) for the COVID-19 outbreak period (March 2020) are calculated relative to the preoutbreak percentage reference baseline (averages of 2018 and 2019). Data are number of cases with percentage in parentheses. Statistical significance was calculated with Fischer exact test.
Fever is in Fahrenheit; oncology: patient with a malignant oncological comorbidity; mortality was assessed for 7 days after admission.
COPD, chronic obstructive pulmonary disease; COVID-19, novel coronavirus disease 2019; CRF, chronic renal failure; DM, diabetes mellitus; ESI, emergency severity index; HR, heart rate (beats per minute); HTN, hypertension; IHD, ischemic heart disease; WBC, white blood count (per microliter of blood).
We further analyzed the ED diagnoses at presentation and the diagnoses in the subgroup of admitted patients in March 2018, 2019, and 2020. Chi-square test showed a significant difference in the distribution of the most common diagnosis groups between the average of March 2018–2019 and March 2020, both in the total attending patients (P = .013) and in the subgroup of patients who were eventually hospitalized (P < .001). Table 3 gives the distribution of diagnosis in hospitalized patients comparing the COVID-19 outbreak period with the same months in 2018 and 2019. The biggest difference was in patients who received the general abdominal pain diagnosis at the end of their ED evaluation: a total of 237 patients in the outbreak period compared with an average of 426 in the corresponding months in 2018–2019 (P < .001). During the COVID-19 outbreak, there was a 47% rise in the number of patients who were diagnosed with appendicitis: 33 in March 2020 compared with 23 in March 2018 and 22 patients in March 2019 (P = .007).
Diagnoses Distribution of Admitted Patients with Nontrauma Surgical Conditions During the 2020 Coronavirus Disease 2019 Outbreak in Israel (March 1–31) Compared with the Corresponding Month in 2018 and 2019
The percentage changes (Δ) for the novel COVID-19 outbreak period are calculated relative to the preoutbreak percentage reference baseline (average of 2018 and 2019). Data are number of cases with percentage in parentheses. Statistical significance was calculated with Fischer exact test. Clinical Classifications Software was used to group visits based on first-listed International Classification of Disease, Ninth Edition, Clinical Modification, diagnoses. Percentages have been rounded to the nearest integer.
COVID-19, coronavirus disease 2019.
There was also a 50% increase (P = .26) in the total number of ED diagnosed peritonitis and intestinal abscess, although not statistically significant: 6 patients in March 2020, and an average of 3 patients in March 2018–19 (P = 0.16). In contrast, there was an 84% drop in the number of patients hospitalized for diverticular disease: from a monthly average of 12.5 patients in March 2018–19 to 2 patients in the outbreak period (P = .049).
Discussion
The results demonstrate the significant impact of the COVID-19 outbreak on the presentation of patients with surgical complaints at our hospital ED. The patient load was only two-thirds compared with the same period the previous year, whereas the proportion of admitted patients was up to 8% higher. The finding of a negative correlation between the national number of diagnosed SARS-CoV-2 infected cases and the presentation at our ED can be explained by the government's orders for social distancing and the public's fear of infection. The public fear of EDs might have been enhanced by the fact that our institution was the nation's first hospital in Israel to admit confirmed SARS-CoV-2 patients.
Several studies have looked at the number of visits to EDs during an outbreak of similar respiratory infectious diseases. Man et al. 4 reported a 50% decrease in the mean daily visits to EDs at the peak of the SARS outbreak in 2003 in Hong Kong compared with the comparable period in 2002. In a study on the impact of SARS in Taiwan in 2003, Chen et al. found a 33.4% drop in the total number of patients coming to the ED. 5 Heiber et al.'s study on the impact of SARS on a community hospital ED in Toronto during the early spread of the virus in 2003 reported results in line with those in Hong Kong and Taiwan, but with a less significant decline of only 21% when comparing all visits. 6 First data regarding trends in hospital presentations in the COVID-19 era were recently published by Italian neurologists who witnessed a decline in new cases of ischemic stroke. 3 None of the studies looked at the specific trends of attendance of patients with surgical conditions during these outbreaks.
The public is well aware that EDs are not the best places to seek care for any ailment, but many are unable to determine whether their condition is serious and warrant a trip to the ED. 13 Adding the risk of possible infection with SARS-CoV-2 tips the scale toward avoiding the ED. It is possible that a portion of the patients contacted other sources for medical care (family practitioners, online advice, etc.), but the exact extent was beyond the scope of this study. We assume that some patients with major ailments decided to postpone their medical care for as long as possible, despite the possible result of significantly worsening their condition.
In the SARS 2003 outbreak, Man et al. documented an increase in the total admission rate at the peak of the outbreak, and a trend of increased severity at presentation—with ESI categories 1 and 2 increasing from 1.5% to 2.5%, although the latter was not statistically significant. 4 Our cohort also had a higher rate of admissions during the outbreak period than the corresponding periods in 2019 and 2018, and more patients presented with tachycardia during the outbreak than in the previous periods, two significant factors that are correlated with a more severe clinical presentation. These results suggest that although fewer people visited hospitals at the time of the outbreak, those who did had a more serious condition. These findings are strengthened by the higher attendance of patients with an ED diagnosis grouped under the ICD-CCS code for peritonitis and intestinal abscess: 6 cases in March 2020 compared with 1 and 4 in 2018 and 2019, respectively, although not statistically significant. Whereas we found no difference between the outbreak period and the corresponding months in 2018–2019 for other factors associated with severity of presentation, such as ESI, self-assessed pain, WBC, and 7-day mortality. We hypothesize that the triage ESI algorithm was not sensitive enough to discriminate between the severity of the presentations, resulting in the majority (85%–90%) of these patients being assigned to level 3. Other important factors indicative of severity, such as the urgent need for surgery, hospital length of stay, and long-term mortality, were not assessed.
Interestingly, the proportion of men presenting during the outbreak period was lower than in previous years, possibly due to publications reporting the poorer prognosis for male patients with COVID-19. 14 A secondary outcome was the change in diagnosis distribution of ED attendees (P = .013)—most significantly in the number of abdominal pain diagnoses. This is a diagnosis code indicating a chief complaint, one usually reserved for patients to which an initial evaluation in the ED ruled out the most urgent etiologies. The 44% decrease in patients given the general diagnosis of abdominal pain (P < .001) is likely explained by the assumption that during this outbreak period, people in a similar situation—presumably with mild pain and without additional objective sign—were inclined to postpone their hospital visit.
In our cohort, there was a 47% increase in the absolute number of ED-diagnosed appendicitis from an average of 22.5 a month in March 2018 and 2019 to 33 in the COVID-19 outbreak period (P = .007). A possible explanation might be that these patients presented later than those in pre-COVID-19 periods, with clear signs of appendicitis resulting in post-ED evaluation diagnosis. It could be plausible that if they have presented earlier, the given diagnosis would have been “abdominal pain,” an indistinct diagnosis code given at times when the etiology is unclear. This is especially true in cases evaluated in the ED at times wherein imaging is unavailable, and the diagnosis is reliant only on physical examination. To better clarify this trend, we compared the monthly number of appendectomy procedures in our institution during the study time: 35 in March 2018, 28 in March 2019, and 25 in March 2020. These data strengthen our assumption, yet further research focused on this subgroup of patients is warranted, especially as the incidence of acute appendicitis has been shown to be influenced by various factors 15
The drastic decline in visits to the ED documented in our study indicates a major health risk to the populations with serious chronic or recent onset diseases. Although the actual outcomes of serious cases that refrained from coming to the ED were not measured, the data argue for public health initiatives to raise awareness of the risks of deferring medical attention at times of crisis. Findings of both our study and those cited previously should convince all clinicians, surgeons among them, to actively reach out to their patients at times of outbreaks. Reduction in the rates of delayed medical care may be achieved, for example, by offering telemedicine consults in which patients can be evaluated without leaving home and receive professional guidance on whether to go to the ED. 16 This option has the added benefit of freeing up doctors and other health care personnel from the EDs to attend to COVID-19 cases, providing the much-needed relief for staff and space 17 and reducing mortality among the more serious cases. 18
The study is limited by its focus on a single population. Furthermore, we had no information about the COVID-19 status of the reviewed patients. It has been shown that the virus can manifest with symptoms that meet the inclusion criteria for surgical cases in our study, such as abdominal pain, but in considerably low numbers. 19 Notwithstanding these limitations, to the best of our knowledge this is the first study to demonstrate the trends of ED attendance of patients with surgical complaints during a COVID-19 outbreak. Our findings call for further research to better evaluate the downstream consequences of the COVID-19 outbreak, specifically the surgical outcomes of patients admitted during the outbreak.
Conclusions
During the COVID-19 outbreak in Israel, we found a significant decrease in the overall number of patients presenting at the ED with nontrauma complaints necessitating a surgical consult. We also witnessed a higher proportion of admissions and patients with tachycardia. These findings imply a more severe presentation, possibly due to patients deferring hospital visits.
Footnotes
Acknowledgments
Almog Yair from the Hebrew University, Jerusalem, Israel, was consulted regarding data analysis and Yotam Arad assisted in figure design. The authors thank health care providers worldwide on the frontline of the COVID-19 crisis.
Authors' Contributions
Each author listed contributed to study design, data collection, data analysis, data interpretation, writing, and critical revisions.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.