
Abstract
Introduction:
Thoracoscopic repair of congenital diaphragmatic hernia (CDH) has become a popular approach and several benefits have been published. Patch closure requires demanding thoracoscopic skills and therefore primary closure with tight sutures is often pursued, which increases the risk of recurrence. The purpose of this study was to create and assess the performance of a new technique for thoracoscopic repair of CDH, which facilitates the surgical procedure.
Materials and Methods:
An innovative system for thoracoscopic repair of CDH with a novel patch was developed. The patch is self-expandable and offers a traction suture for stabilization, isolating and protecting the viscera. Its performance was assessed and compared with a conventional patch in an inanimate model of the disease through a quantitative and qualitative multivariate analysis.
Results:
Nine cases of CDH were repaired with each patch. The duration of the procedure was shorter (P < .05) and the level of difficulty was reported to be lower (P < .001) when using the self-expandable patch (SeP). The number of good quality knots was higher and adverse events were less common with this new technique.
Conclusions:
The stabilizing SeP offers safe and ergonomic performance for thoracoscopic CDH repair, facilitating the surgical technique. The main advantage is that it keeps the viscera isolated into the abdomen while offering a flap on the thoracic side for suturing in a practical manner, minimizing the risk of visceral injury and saving surgical time.
Introduction
Congenital diaphragmatic hernia (CDH) is a defect caused by an abnormal development of the pleuroperitoneal fold. It occurs in about 1 in every 3000 births and allows herniation of the abdominal content into the thorax.1,2
The Bochdalek hernia, which is a posterolateral defect, represents 95% of CDHs and affects the left side in 80% of cases. 3
Traditional approaches to repair CDH include thoracotomy or laparotomy with primary or patch closure. 4 Minimally invasive surgery later proved to be feasible in neonates for different pathologies.5–8 Several benefits have been demonstrated for thoracoscopic repair of CDH when compared with open approaches, such as decreased hospital stay, mechanical ventilation days, time to feeding, postoperative partial pressure of CO2, postoperative analgesia, severe complications, hospital charges, and general morbidity.9–16
Although the thoracoscopic approach has become popular in CDH, 17 some cases require demanding thoracoscopic skills and the learning curve is critical for the current technique. 18 Higher recurrences and technical difficulties are increasingly reported,9,10,19,20 especially when the defect demands a patch placement, which happens to be a more challenging procedure to do endoscopically.21,22
Several investigators have been trying to compare different patches and identify new materials to create better meshes.23–32 However, it seems that the surgical technique needs an overall improvement, especially concerning ergonomics, to simplify the procedure and upgrade the results. 9
We have designed an innovative system for thoracoscopic repair in newborns in an attempt to overcome the challenges of mesh placement. The developed system incorporates a self-expandable patch (SeP) that effectively restrains the viscera in the abdomen during the suturing process. The feasibility of the system was assessed in an inanimate model of the disease.
Materials and Methods
We have developed a scientific innovation for CDH repair. Employing the same surgical approach, we have compared the performance of a stabilizing SeP designed by our group with a conventional patch (CP) that is commonly used in clinical practice. The patches used were 5 cm in diameter and the size of the diaphragmatic defects was 4 cm in diameter for standardization. The operations took place on an inanimate model of the disease, also created by our group based on a previously validated model. 33 A group of pediatric surgeons experienced in endoscopic surgery conducted the technical assessment by repairing nine cases of CDH with each type of patch (n = 18 CDH cases).
Patch, functional features
This novel patch system has been created to facilitate the thoracoscopic repair of neonatal CDH. It has characteristics of self-expandability due to the presence of a semirigid ring. Once the ring is expanded in the abdominal side of the defect, it remains deployed in close contact with the diaphragmatic rim facilitated by the positive pressure of the abdominal cavity and the negative pressure of the thoracic compartment. The patch itself isolates and protects the viscera in the abdominal compartment, minimizing the risk of injury.
The patch forges a pocket around the ring, embracing it. The margins of that pocket in its thoracic side will be facing the diaphragmatic rim to allow an easy and precise suture. Eventually, the ring will give a safe surface below every stitch to avoid inadvertent injuries of the underlying viscera.
Finally, the mesh is essentially stable due to a central traction suture that keeps the patch in close contact with the diaphragmatic rim (Fig. 1).
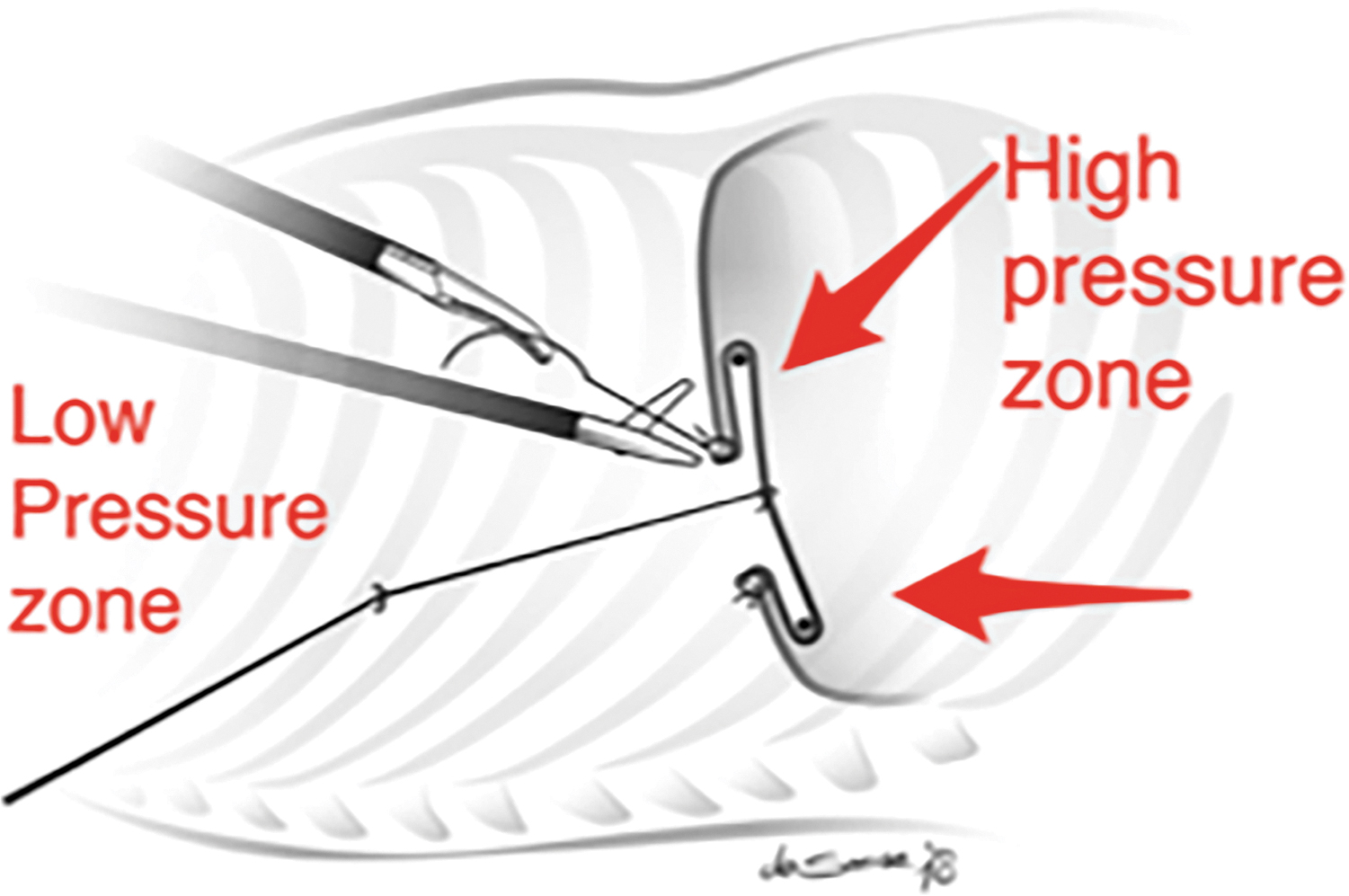
Schematic representation of the novel patch placed in the diaphragmatic defect.
Patch, architectural construction
The SeP can be built with any kind of biocompatible material approved by medical use if it complies with the functional features.
In our model, it has been created with FixomullR Stretch 10 × 2 cm (BSN medical, Ref. 70022-00), which is a stretchable nonwoven polyester coated with a hypoallergenic polyacrylate adhesive. For construction of the thoracic layer, two circles, 6 cm in diameter, were pasted on top of each other, with their adhesive surfaces facing one another (Fig. 2a). For the abdominal layer, two circles (6 and 8 cm) were pasted on top of each other as described for the thoracic surface (Fig. 2b).
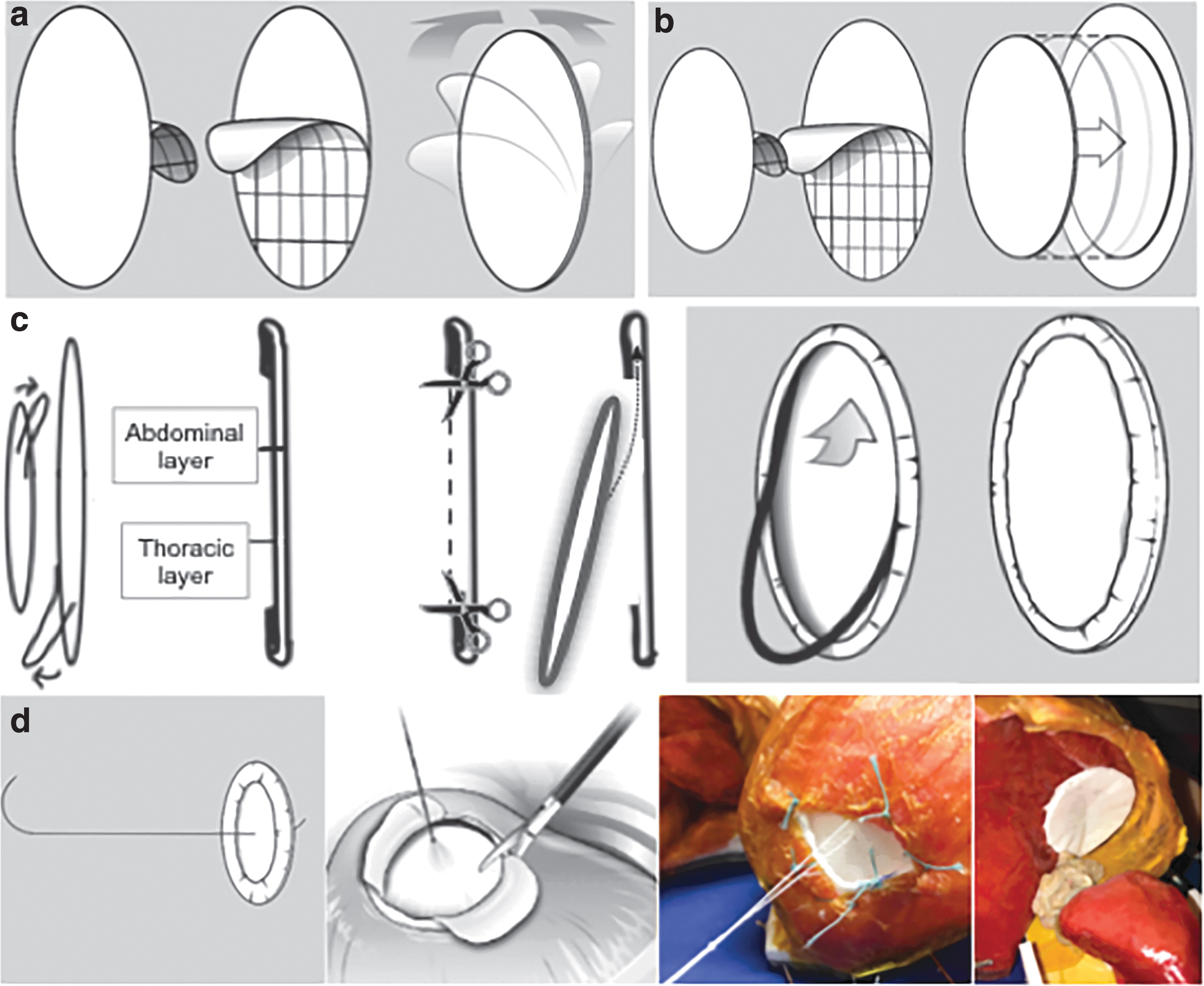
Schematic representation of the SeP construct.
Both abdominal and thoracic layers approached each other (Fig. 2c). The 2 cm difference between the two layers was used to create the pocket by folding that margin over the thoracic surface. Afterward, the center of the thoracic surface was cut off for open access to the pocket, where the semirigid 6-cm ring was placed. This ring has shape memory, so the patch remains expanded. In our model, it has been made with the stent positioner of a pigtail ureteral stent (Cook® Medical Ref. 036308), joining the ends with n-butyl-2-cyanoacrylate adhesive (B Braun Histoacryl® Ref. 1050052).
Finally, we have added a 20-cm 2/0 silk suture in the center of the patch that allows traction from the thoracic cavity against the diaphragmatic rim, giving in situ stability for the suturing process (Fig. 2d).
Surgical technique
An inanimate model of CDH was used to recreate the surgical technique based on a previously validated model (Fig. 3).

Inanimate model for thoracoscopic repair of CDH. CDH, congenital diaphragmatic hernia.
To begin the thoracoscopic repair of CDH, the SeP was introduced into the thorax by rolling through the trocar. After the abdominal viscera were carefully reduced into the abdomen, the SeP was placed in the abdominal surface of the diaphragmatic rim to isolate the viscera. Once the SeP was adequately positioned, the central suture was pulled through one of the trocars to keep the patch stable during the suturing process. The suturing could be done using an intracorporeal or extracorporeal knot-tying technique. In our model, the goal was to place at least eight equidistant interrupted stitches with at least three throws per knot in the 5-cm diameter patches for closure of the 4-cm CDH-created defects. When the suturing process was completed, the central suture could be cut away.
Variables compared for both patches (SeP vs. CP)
Surgical time for patch placement was assessed in minutes from its introduction through the port until its complete suture.
Quality of the suturing process was evaluated by quantifying the number of good quality knots (with at least three throws per knot, tight enough for the patch and the diaphragmatic rim) and the occurrence of adverse events during the suturing process such as bowel injury, diaphragmatic rips, or big gaps between knots (when the gap is >2 cm between knots).
Level of difficulty of the procedure was assessed using a five-point Likert scale (very easy, easy, intermediate, difficult, and very difficult).
Statistical analysis
Quantitative and qualitative data results are expressed as mean ± standard deviation. For comparison of non-normally distributed groups, differences between means were compared using the Mann–Whitney test. Statistical analysis and figures were performed using the Prism 8 package (GraphPad Software, Inc., La Jolla, CA) and P value <0.05 was considered statistically significant.
Results
Nine CDH cases were repaired with each type of patch (n = 18 CDH cases) in an inanimate model of the disease by experienced pediatric surgeons.
The surgical time taken for SeP placement was significantly lower (29.3 ± 5.6 minutes) compared with 33.2 ± 5.9 minutes for the CP (*P ≤ .05, Mann–Whitney) (Fig. 4a). The differences in time taken to place and suture the patch can be observed in the heat map (Fig. 4b).
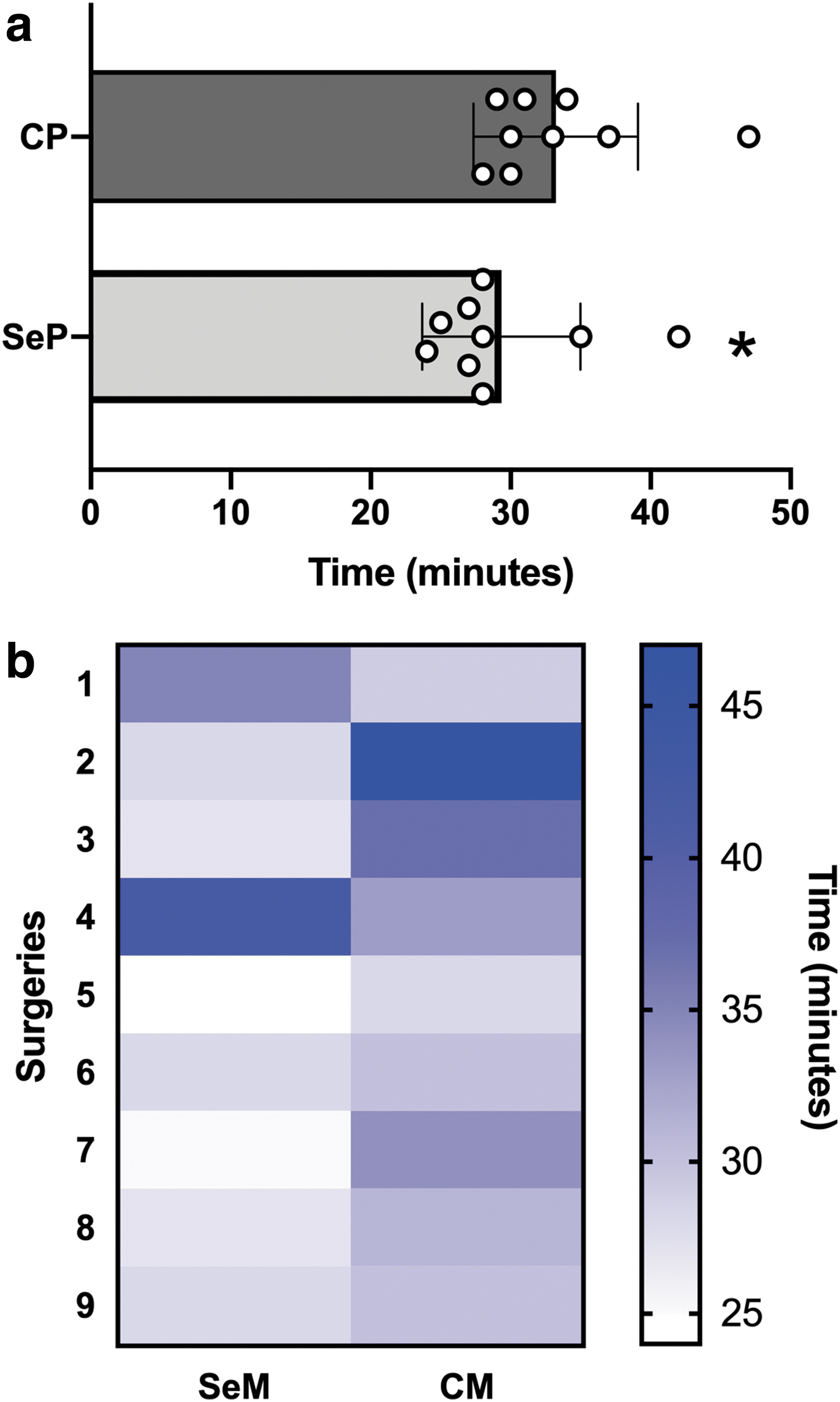
Surgical time for patch placement.
The number of good quality stitches/knots per patch was 7.9 ± 0.3 for SeP and 7.3 ± 1 for CP, considering that the number of stitches placed per mesh was eight in our model (Fig. 5a). The percentage of surgeries in which all knots were of good quality (scoring 8 of 8) was 55.6% for CP and 88.8% for SeP, this difference not being statistically significant.
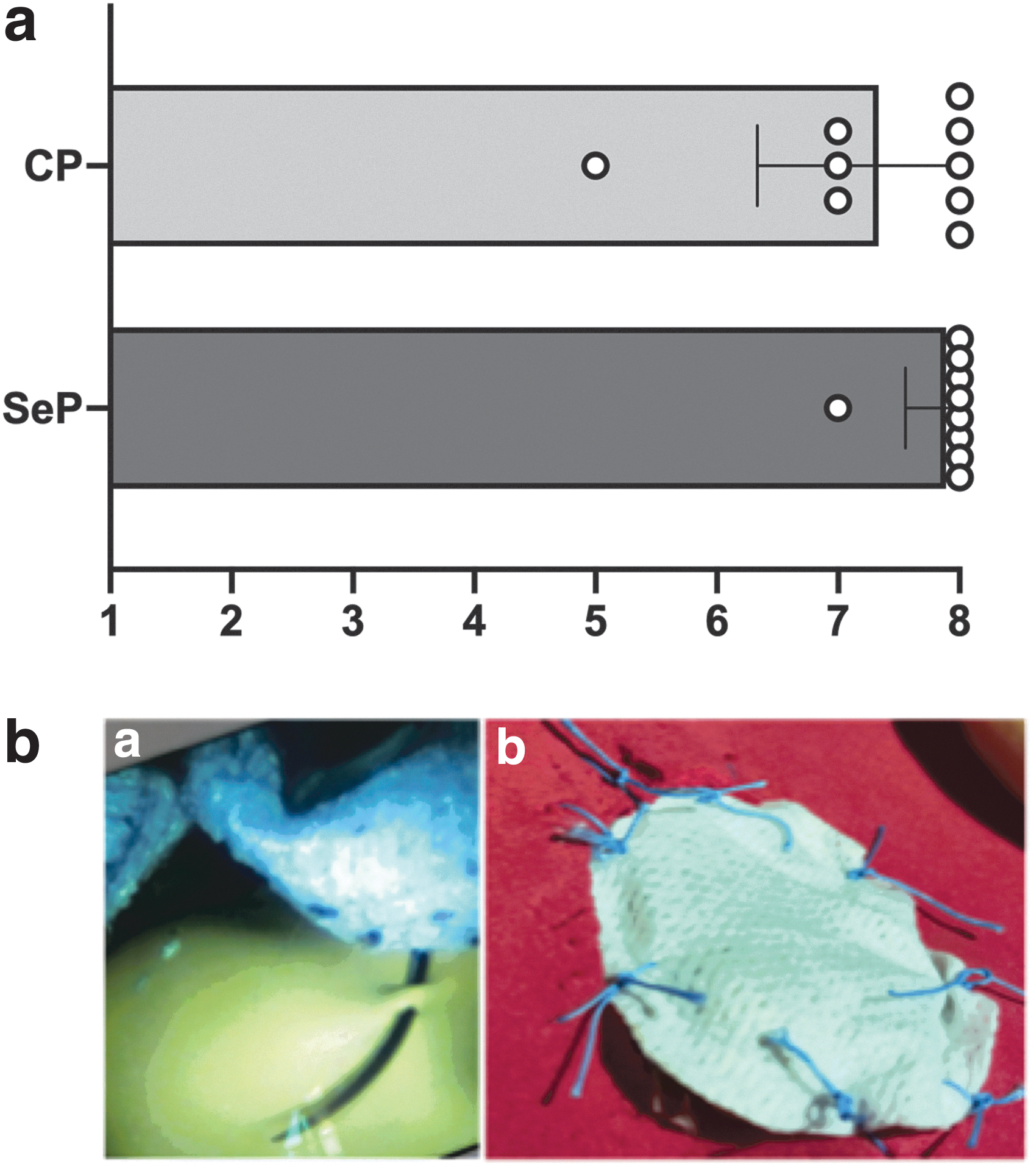
Analysis of the quality of stitches and knots.
The number of adverse events that occurred during the suturing process was one for the SeP (diaphragmatic rip n = 1) and seven for the CP (bowel injury n = 2, diaphragmatic rip n = 2, and big gaps between knots n = 3) (Fig. 5b).
The level of difficulty reported for each procedure using a five-point Likert scale was 4.8 ± 0.3 and 4.0 ± 0.5 for SeP and CP, respectively (**P ≤ 0.001, Mann–Whitney) (Fig. 6a). SeP placement was reported to be very easy (n = 8) and easy (n = 1) and for the CP, it was very easy (n = 1), easy (n = 7), and intermediate (n = 1) (Fig. 6b).
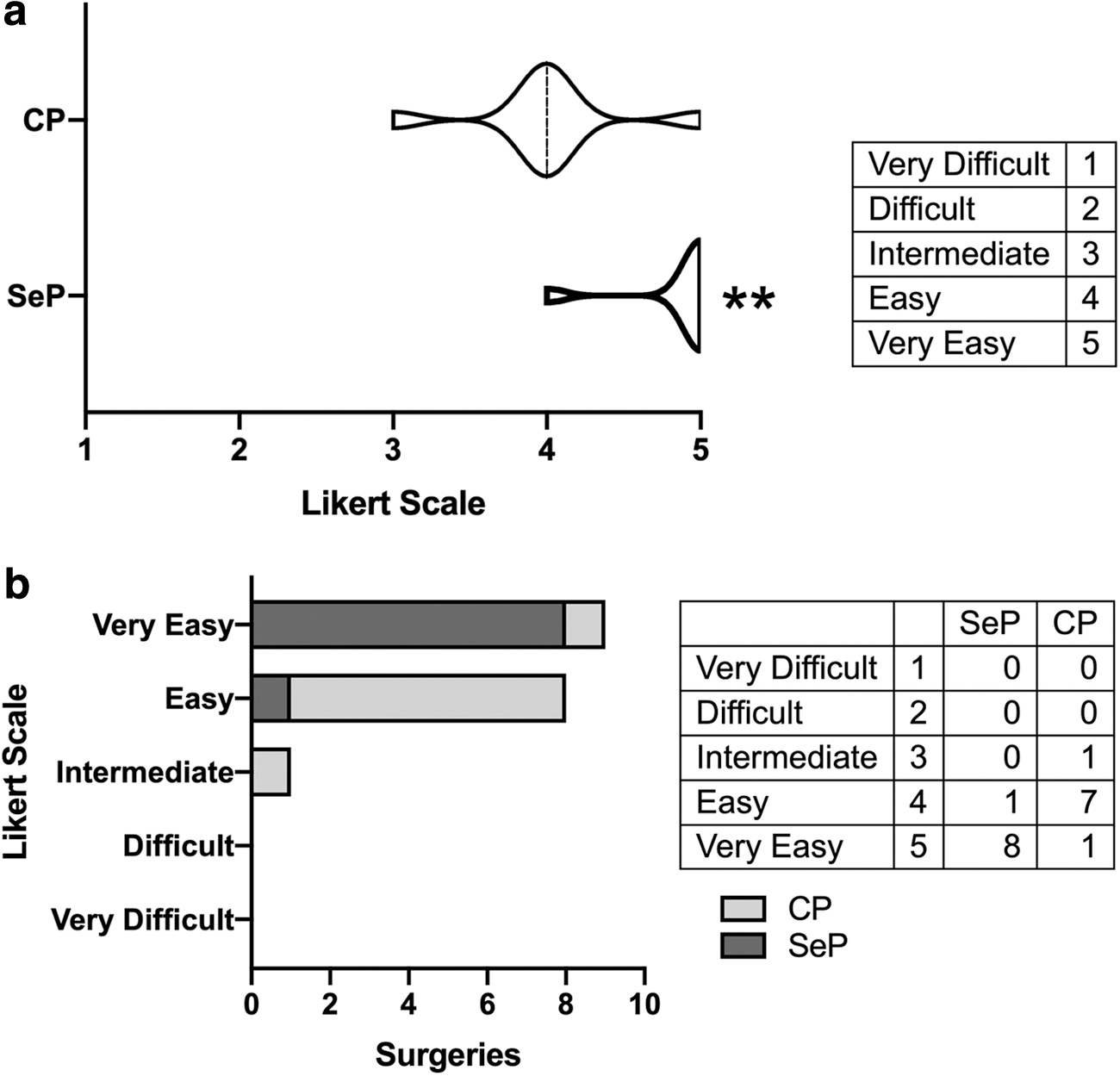
Level of difficulty reported for each patch placement.
Discussion
The thoracoscopic approach for CDH repair has plenty of benefits9–15,34 and it is currently being used routinely by many pediatric surgeons all over the world.17,35 However, higher recurrences, longer operation times, and technical difficulties are increasingly reported.9,10,19 Furthermore, few advances in the surgical technique have been released since the implementation of thoracoscopy for CDH. 36
One of the main obstacles during the surgery is that once herniated organs are placed in the abdomen, they tend to go back to the thorax, blocking the surgical field and adding a risk of visceral injury.8,21,37 The ergonomics of the surgical procedure still has room for improvement, especially for cases where the defect is large enough to require mesh placement.21,22 Many surgeons who experience difficulties closing the defect or suturing the patch tend to convert the surgery to an open approach, dramatically increasing the surgical time and the magnitude of the procedure.21,35 In more impactful cases, primary closure with tight sutures is pursued, which increases the risk of recurrence.21,34,38
Placing a patch is not an infrequent event. According to the Congenital Diaphragmatic Hernia Registry 1995–2009, 48.3% of the CDH repair cases required a mesh. 39 Furthermore, although there are several biological and synthetic (absorbable and nonabsorbable) patch types available and a great number of publications comparing them,23–28 the ideal mesh remains elusive.27,40
In this study, we have developed a surgical innovation to remove the technical barriers described for thoracoscopic repair of big, congenital diaphragmatic defects.
The stabilizing SeP offers safe and ergonomic performance, facilitating the surgical technique. The main advantages of this system are that it keeps the viscera isolated into the abdomen while offering a flap adjacent to the diaphragmatic rim for suturing in a comfortable and practical manner, minimizing the risk of visceral injury and saving surgical time, which especially benefits patients with pulmonary hypertension.
The quality of the suturing process is superior with this novel patch, and although in this surgical model it is not possible to follow-up for the analysis of long-term results, it would be interesting to study (in animal models) if these immediate benefits observed have some impact on the recurrence of the disease. The patch developed in this study is synthetic, but it is customizable, and as the material is not the focus of the proposed system, it could be made with biological materials as well.
Regarding the main limitations of our study, low-experience pediatric surgeons should have also participated in the patch assessment. This fact would allow us to see if there are even bigger differences between both mesh performances due to the previous learning curve reached with the CP. Moreover, the number of surgeries should have been greater to generate sufficient statistical power, and the population of surgeons evaluating the quality of the surgical result should have been blinded to avoid any expectancy bias.
Footnotes
Disclosure Statement
The authors, C.A. and J.L.P., declare that the patch system (self-expandable surgical implant for correction of congenital diaphragmatic hernia) was under provisional patent 62/821,504, and is currently under a U.S. Non-provisional Patent No. 16/824,057, filed on 03/19/2020. M.O. and M.F.V. have no conflicts of interest.
Consent for Publication
All authors read and approved the final manuscript.
Data Availability
Data supporting the findings of this study are available within the article and its supplementary information.
Authors' Contributions
Study concept and design were performed by C.A. and J.L.P.; acquisition of data was performed by C.A. and T.M.; analysis and interpretation of data were performed by M.O., J.L.P., C.A., and M.F.V.; drafting of the manuscript was performed by C.A., M.F.V., M.O., and J.L.P.; critical revision of the manuscript for important intellectual content was performed by M.O., M.F.V., and J.L.P.; statistical analysis was performed by M.O. and M.F.V.; funding was obtained by C.A. and J.L.P., Pediatric Surgery Division internal funding support at their respective institutions; technical or material support was provided by M.O. and M.F.V.; and study supervision was performed by C.A. and J.L.P.
Funding Information
Pediatric Surgery Division internal funding support was provided by CCHMC and CMI Pediátrica.