
Abstract
Background:
At the end of a laparoscopic major hepatectomy, an incision wide enough for specimen retrieval is required. Classically, Pfannenstiel (PF) incision is the type of access favored as service incision in laparoscopy. However, in specific settings the use of a midline (ML) incision can be favorable, with doubtful impaction on the outcomes of a purely laparoscopic operation. The aim of this study was to investigate on clinical outcomes after laparoscopic hemihepatectomies using PF/ML incisions in comparison with open.
Methods:
The institutional clinical database of the Hepatobiliary Division at San Raffaele Hospital (Milan, Italy) was retrospectively reviewed identifying cases of laparoscopic and open hemihepatectomies. Three analyses were performed: whole laparoscopic versus open; ML versus open; PF versus ML. Clinical outcomes such as intraoperative blood loss, operative time, postoperative morbidity, motility resumption, perceived pain, and length of stay (LOS) were used for comparisons.
Results:
Laparoscopy was confirmed to be superior to open approach also in the present series in terms of lower blood loss (300 versus 400 mL, P = .041), fewer complications (14.2% versus 25.9%, P = .024), shorter hospitalization (5 versus 7 days, P = .033), and enhanced recovery in terms of better pain control (P = .035) and mobility resumption (P = .047). Similar outcomes were observed comparing ML alone with open (estimated blood loss 300 mL versus 400 mL, P = .039; complications 13.1% versus 25.9%, P = .037; LOS 5 days versus 7 days, P = .04; lower pain perception, P = .048 and faster mobility resumption, P = .046). No significant differences were observed in postoperative outcomes of PF versus ML.
Conclusions:
Suprapubic and ML incisions at the end of a pure laparoscopic case lead to comparable outcomes between each other. The adoption of ML incision for specimen retrieval does not affect outcomes of minimal invasiveness.
Introduction
Laparoscopic liver surgery has greatly expanded and developed during the last 25 years and is now a daily practice in many institutions, because its benefits are well known and proven in terms of reduced intraoperative bleeding, fewer postoperative morbidities, and enhanced recovery.1–22
Whereas the topic of retrieval incision is almost insignificant in minor liver resections, in major resections it acquires more importance. Actually, when a bulky specimen has to be retrieved from the abdominal cavity, an incision wide enough is required to avoid specimen's squeezing and morcellation, especially in procedures performed for malignant disease.
However, one wonders whether the efforts of performing challenging procedures like laparoscopic hemihepatectomies may be jeopardized by the need of a huge retrieval incision potentially leading to reduced clinical benefits. Furthermore, the best site for specimen extraction is another open issue. In the decision-making process more items are to be taken into account: several patients undergoing liver resection might already present with a previous laparotomy (i.e., after the resection of primary tumor)23,24; others may have portosystemic shunts owing to portal hypertension; others with very fragile lesions may have a risk of lesion rupture while the specimen is retrieved. In this scenario, the surgeon mainly has two choices at the end of a laparoscopic major liver resection, by performing a suprapubic incision or going through a short midline (ML) incision.
The aim of this study was to investigate on this topic, to understand whether the type of retrieval incisions required for major hepatectomies can affect the outcomes of laparoscopy having an impact on the benefits associated with minimally invasive technique.
Methods
Study population
The prospectively collected clinical database at the Hepatobiliary Surgery Division of San Raffaele Hospital, Milan, was retrospectively reviewed. The study period ranged from the beginning of the program in 2004 to June 2019. Written informed consent was signed by participants. To obtain a homogeneous population with extraction sites comparable for similar dimensions, only hemihepatectomies (left and right) were considered for this study. All cases completed in a pure laparoscopy fashion (PLAP) were included, whereas converted to open were excluded. The control group was consistent with a cohort of open hepatectomies chosen from the pool of total hemihepatectomies, after applying the following exclusion criteria: associated liver partition and portal vein ligation for staged hepatectomy procedures, staged hepatectomies, previous liver surgery and procedures requiring vascular resection and/or biliary reconstruction.
The following outcomes were considered for comparison: intraoperative estimated blood loss (EBL) and operative time; postoperative minor and major complications according to Dindo–Clavien classification 25 ; liver-specific (such as bile leakage, ascites, transient partial liver failure) and wound-related complications; and time of hospitalization and 30- and 90-day mortality. Furthermore, a visual analogue scale (VAS) ranging from 1 to 5 (slight to worst pain) was implemented in the immediate postoperative period and a mobility score (from 1 to 10, ranging from lying in bed to being fully independent in every daily activity) was collected for the first five postoperative days (PODs) from patients subjected to laparoscopic hemihepatectomies.
Statistical analysis was performed by comparison of:
PLAP versus open series; ML group versus open series; ML group versus Pfannenstiel (PF) group.
Operative setup
The patient was placed in a “modified” French position for both open and laparoscopic approaches. Inferior and superior limbs were abducted. Furthermore, a slight flexion of ankles and knees was applied to achieve more stability in case of extreme tilting. During surgery, the operative table was tilted to the left and reverse Trendelenburg was applied.
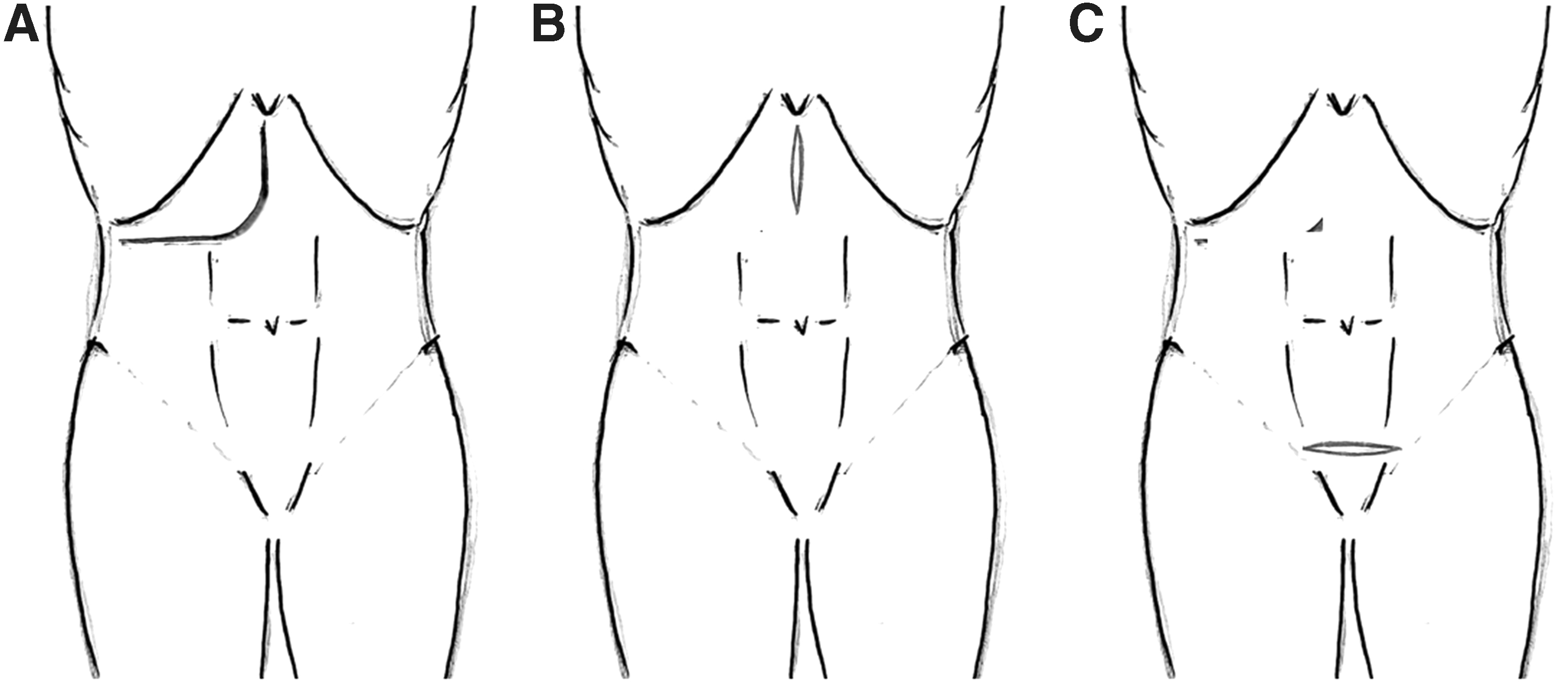
The J-shaped incision is the type of access to the abdominal cavity was performed in open procedures (Fig. 1A).
For laparoscopic procedures, a standardized setup of five 12 mm ports was used for all liver resection types. Liver resection was performed during temporary inflow interruption through the application of the Pringle maneuver (extracorporeal technique was applied in laparoscopic cases). The parenchymal transection was performed by alternating an energy device based on ultrasonic and radiofrequency energies, and an ultrasonic aspirator for parenchymal fragmentation. Vascular structures were sealed by wet bipolar forceps or clips according to dimension. In accordance with the local ERAS protocol,12,13 an abdominal drain was left in place if biliostasis was not satisfying at the end of the procedure or in case of previous liver surgery.
The extraction site for laparoscopic procedures was either with a short ML incision or through a suprapubic incision (Fig. 1B, C).
The algorithm followed for the choice of the extraction site is given in Figure 2. In particular, for specimens whose size was inferior to 3 cm, a site port enlargement was considered sufficient for the extraction. For intermediate size specimens, either a PF incision in naive abdomens or an ML incision in the presence of a previous laparotomy can be chosen. Bulky specimens requiring bigger incisions can either be extracted from an ML (if not obese) or alternatively through a PF. However, for patients who already had upper ML incisions, the same ML incisional scar could be used for subsequent operations.
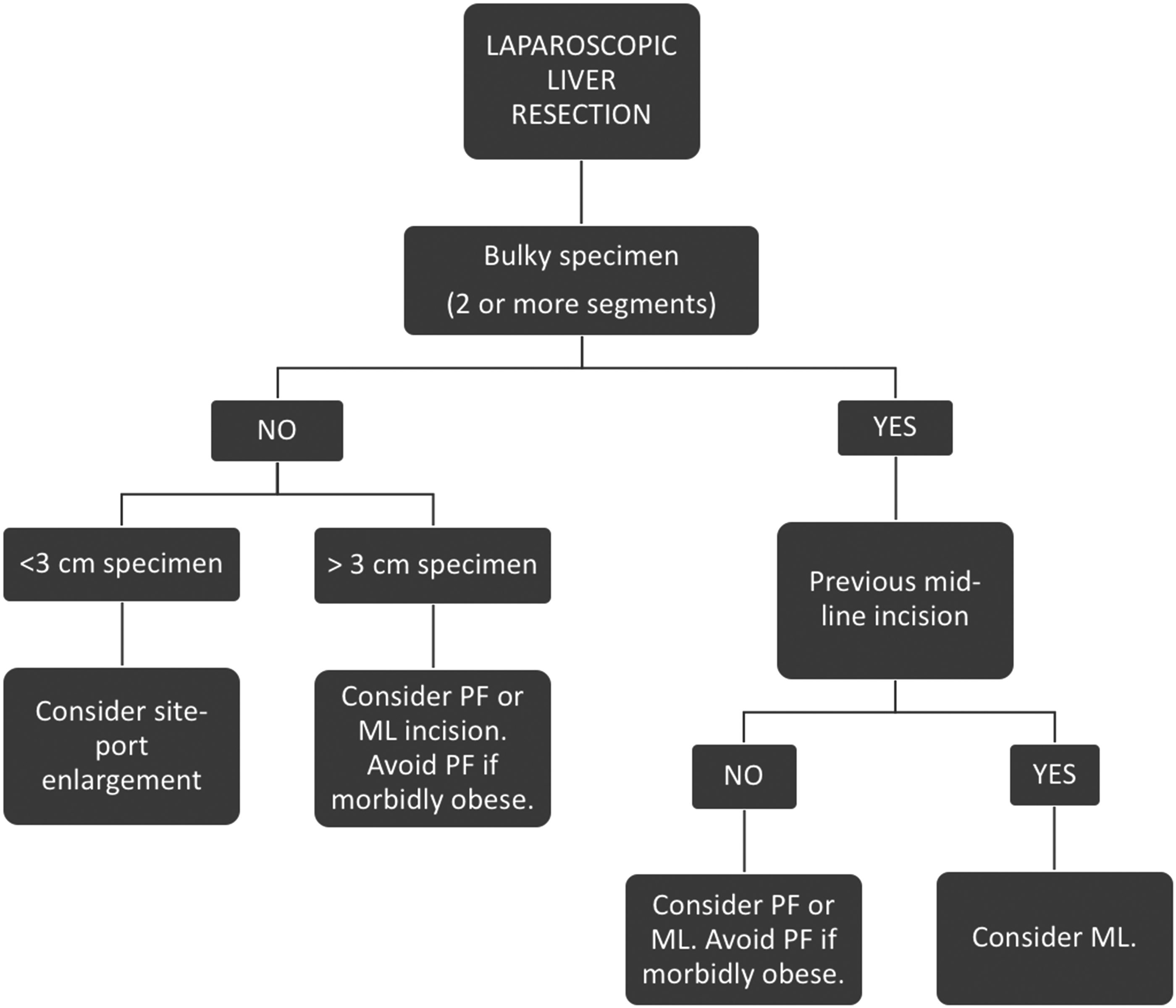
Flowchart for the choice of the extraction site.
When a suprapubic access was required, a properly said PF was performed.
Postoperative management
For pain management, a right paravertebral catheter for the continuous administration of naropine and sufentanil was placed in patients who are candidate to right hemihepatectomy.
Postoperatively, all patients received 1 g paracetamol every 8 hours, initially intravenous (i.v.) and then per os (p.o.) since POD-1. A mild opioid analgesic, tapentadol, was administered p.o. since POD-1 (50 mg, twice a day). Finally, 30 mg of ketorolac was used as rescue therapy in case of pain, either i.v. or p.o.
The institutional ERAS protocol required early mobilization of all patients. On POD-1, patients were prompted to move from the bed to the chair and, in the afternoon, they were incited to take small walks in their room or in the hallways. Oral feeding was restored the same evening of the operation or the following morning. Infusions were discontinued and the urine catheter was removed on POD-2. The application of the same perioperative management protocols for all patients' cohorts is fundamental to drastically reduce any risk of potential bias.
Statistical analysis
Comparisons were performed using the χ 2 test or Fisher's exact test for categorical data, and the Mann–Whitney U-test for ordinal data. Nonparametric data analysis was performed using the χ 2 or Fisher's exact test when appropriate. All data were expressed as mean plus standard deviation or as median and range when appropriate. Significance was defined as P < .05. All analyses were performed using the Statistical Package SPSS 18.0 (SPSS, Chicago, IL).
Results
Study population
During the study period 205 laparoscopic hemihepatectomies were performed; 36 cases were converted to open (17.5%) and were excluded from the comparison with the open series. Open hemihepatectomies were 603; after discarding per the exclusion criteria, 81 open hemihepatectomies were available for the comparison.
Table 1 shows the series of hemihepatectomies during the study period. No significant differences were observed between the two cohorts in terms of gender distribution, age, BMI, American Society of Anesthesiologists Classification score, presence of chronic liver disease/steatohepatitis. Right and left hepatectomies were equally distributed (right hepatectomies were 50.2% and 60.5%, P = NS) and there were no differences for tumor type (operations were performed for malignancy in 82.2% and in 87.7%, P = NS).
Comparison of Pure Laparoscopic (Pfannenstiel + Midline) Versus Open Hemihepatectomies
ASA, American Society of Anesthesiologists Classification; BMI, body mass index; CRLM, colo-rectal cancer liver metastases; EBL, estimated blood loss; HCC, hepatocellular carcinoma; IQR, interquartile range; LOS, length of stay; NS, not significant; OR, operative room time.
As no significant differences were outlined in the baseline characteristics of the two cohorts, the following analyses were implemented.
Laparoscopy versus open
Comparing laparoscopy and open, lower intraoperative bleeding was observed in PLAP (300 versus 400 mL, P = .041). Laparoscopy had fewer major and minor complications (14.2% versus 25.9%, P = .024) encompassing liver-specific (9.5% versus 22%, P = .006) and wound-related complications (1.8% versus 9.9%, P = .003). Postoperatively, length of stay (LOS) was shorter in PLAP (5 versus 7 days, P = .033). PLAP series was also associated with less postoperative pain since returning to ward to POD-5 (P = .035) and with a faster mobility resumption (P = .047) (Fig. 3A).

VAS and mobility scale.
ML versus open
Subgroup analysis was performed comparing ML group alone and open, to address the question whether a short ML incision for specimen retrieval at the end of a laparoscopic case could affect the benefits of laparoscopy (Table 2). ML group was characterized by lower EBL (300 versus 400 mL, P = .039), lower morbidity rate (13.1% versus 25.9%, P = .037), fewer liver-specific complications (10.6% versus 22.2%, P = .046), and shorter LOS (5 versus 7 days, P = .04). There was one wound-related complication in the ML cohort (1.2% versus 9.9%, P = .014). Furthermore, patients in ML group experienced lower pain (P = .048) and a quicker recovery in terms of mobility in comparison with open (P = .046) (Fig. 3B).
Comparison of Midline Versus Open
ASA, American Society of Anesthesiologists Classification; BMI, body mass index; CRLM, colo-rectal cancer liver metastases; EBL, estimated blood loss; HCC, hepatocellular carcinoma; IQR, interquartile range; LOS, length of stay; NS, not significant; OR, operative room time.
PF versus ML
Comparing the subgroups of the laparoscopic series between each other (PF and ML), no significant differences were found (Table 3). Intraoperative bleeding (300 versus 300 mL, P = NS), operative room time (330 versus 308 minutes, P = NS), postoperative complications (15.3% versus 13.1%, P = NS), liver-specific complications (8.3% versus 10.6%, P = NS), and wound-related complications (2.4% versus 1.2%, P = NS) were similar. No difference in LOS (5 versus 5 days, P = NS) was observed. Finally, no difference was observed in the comparison of the postoperative pain assessment (P = NS) and the postoperative mobility score (P = NS) (Fig. 3C).
Comparison of Pfannenstiel versus Midline Incision
ASA, American Society of Anesthesiologists Classification; BMI, body mass index; CRLM, colo-rectal cancer liver metastases; EBL, estimated blood loss; HCC, hepatocellular carcinoma; IQR, interquartile range; LOS, length of stay; NC, not calculated; NS, not significant; OR, operative room time.
Discussion
The results of this study confirm that the advantages of laparoscopy versus open are detectable in patients undergoing major hepatectomies regardless of the extraction site (ML incision or PF incision) chosen for specimen retrieval.
The study was designed providing three separate analyses to specifically rule out any possible negative impact on the outcomes of a laparoscopic procedure secondary to ML service incision.
The first analysis was aimed to compare the pure laparoscopic series of hemihepatectomies to open, confirming the acknowledged benefits conferred by laparoscopy in terms of lower blood losses, fewer complications, and enhanced recovery.
The second analysis was focused to verify whether the adoption of a ML incision as extraction site in a purely laparoscopic operation could somehow jeopardize the efforts of laparoscopy. Results from the present series allow to confer the same advantages reported in the literature when comparing open and laparoscopic major hepatectomies.
The purpose of the third analysis was to evaluate whether some differences exist between the choice of PF and ML; no significant differences were observed.
Performing an ML incision rather than a suprapubic one can be advantageous in some scenarios, such as in patients with severe adhesions whose interruption might increase the risk of visceral injury and to elongate the operative time, and also in patients with diabetes and suffer from severe obesity who are more prone to surgical site infections, 26 and in cases of fragile bulky lesions, whose transit inside the abdominal cavity to reach the pelvis could determine a risk of rupture.
Concerning intraoperative blood loss, it was confirmed in this study that PLAP is associated with lower bleeding. The same difference was seen between ML alone and open. Furthermore, ML and PF were associated with similar EBL, indicating that the choice of the extraction site does not have any impact on it. In addition, complication rate and LOS were lower in PLAP and in ML in comparison with open, whereas no difference was observed between ML and PF. The latter results confirm once more that the choice of an ML incision does not affect outcomes of laparoscopy.
Liver-specific complications were significantly lower in PLAP and in ML-alone series in comparison with open. Considering the types of complications in this category, only one bile leakage out of the five registered in the PLAP cohort was seen in the ML series. It might be speculated that on certain occasions the possibility to check directly the transection plane through an ML incision used as extraction site might reduce the possibility of not discerning a bile leak during the pneumoperitoneum, giving an additional opportunity to verify the biliostasis. However, such difference was not significant in the comparison between PF and ML, and accounts only for a different distribution of bile leakage rate in the two groups.
An inferior rate of ascites was seen in PLAP versus open, which is in line with previous studies where patients with chronic liver disease were shown benefitting more from laparoscopy, whereas no difference was observed between ML and PF. Hence, the choice of an ML incision does not impact on this parameter.
Concerning the wound-related complication rate, this was statistically inferior in the PLAP series in comparison with open. The only complications encountered in the laparoscopic series were one dehiscence in ML group and one surgical site infection in PF and one rectus muscle hematoma in PF group that required vascular embolization. However, no statistically significant difference was seen between PF and ML.
Guilbaud et al. 27 have recently investigated on the topic of the extraction site applied to laparoscopic major hepatectomies. In their series, focused to compare outcomes of laparoscopic liver resections with subcostal, ML, or suprapubic incisions, the authors found ML was harbinger of a higher rate of postincisional hernia in comparison with suprapubic incisions (ML versus PF, 26.6% versus 10.1%, P = .030). However, 85.7% of patients in the ML group had had a previous abdominal surgery, which is likely an element that has greatly contributed to such a high rate of postincisional hernia.
Despite suprapubic incisions being known for their safety, some studies of gynecological derivation have reported morbidity rates as high as 8% encompassing wound disruption, tissue necrosis, and rectus hematoma.28–33 Obese patients are more prone to wound-specific complications, such as infection and dehiscence, as was previously assessed in a series of obese women after abdominal hysterectomy, where infection rate was between 4% and 12%. 26 Therefore, suprapubic incisions in the setting of morbid obesity should be carefully evaluated in the presence of valid alternatives such as ML incision. In addition, differently from gynecological series, patients with liver tumors are more likely to suffer from chronic liver disease and cirrhosis, which is itself an independent risk factor for surgical site infection after hepatic resection. 34
From these considerations it was conceived that the algorithm presented in Figure 2 aimed to guide our choice of the surgical extraction site in liver resections and that was on the basis of this study.
Concerning pain perception, PLAP patients experienced statistically significant less pain in comparison with open. Furthermore, ML alone resulted in less pain in comparison with open, despite the same protocol for pain management being followed. Possible mechanisms to explain this observation are as follows: the ML incision is definitely shorter in comparison with the J-shaped incision and muscular impairment is reduced; the period of traction on the abdominal wall during specimen extraction at the end of a laparoscopic procedure is brief in comparison with the retraction time required during an entirely open operation, where traumatism on ribs is likely superior. Of note, the protocol for pain management is the same in the two groups (ML and open), thus reducing the risk of confounders. No difference was observed in pain perception between ML and PF.
Similarly, mobility resumption was faster and easier in PLAP in comparison with open. The same was observed also in ML versus open, whereas there was no significant difference in ML versus PF.
PF and ML were not associated with differences in operative times. In certain situations, the choice of ML is motivated also from the presence of severe adhesions in the lower abdomen (i.e., as a consequence of previous colorectal surgery), whose interruption would be time consuming, other than harbinger of possible visceral injury. Based on this, the choice of ML is likely a time saver, which possibly contributes to the lack of different duration between the two approaches.
To our knowledge this is the first technical report in the field of minimally invasive liver surgery specifically addressing the topic of extraction site in laparoscopic hemihepatectomies. Some similar studies were previously reported in the field of colorectal surgery. Santoro et al. 35 in their systematic review compared transverse and ML skin incision in laparoscopic right colectomy; no significant differences were found in terms of morbidity, motility resumption, postoperative pain and analgesia, occurrence of incisional hernia, wound infection, and LOS among the adoption of the two approaches.
A final topic worthy of mention regards the type of transverse suprapubic incision that differ for the orientation of the dissection (Fig. 4). Although the Kustner and the Cherney incisions are suprapubic accesses commonly used in gynecology for pelvic surgery, the properly said PF incision offers adequate exposure in liver surgery through transverse incision of the fascia and lateral spread of muscles, even for bulky specimens.
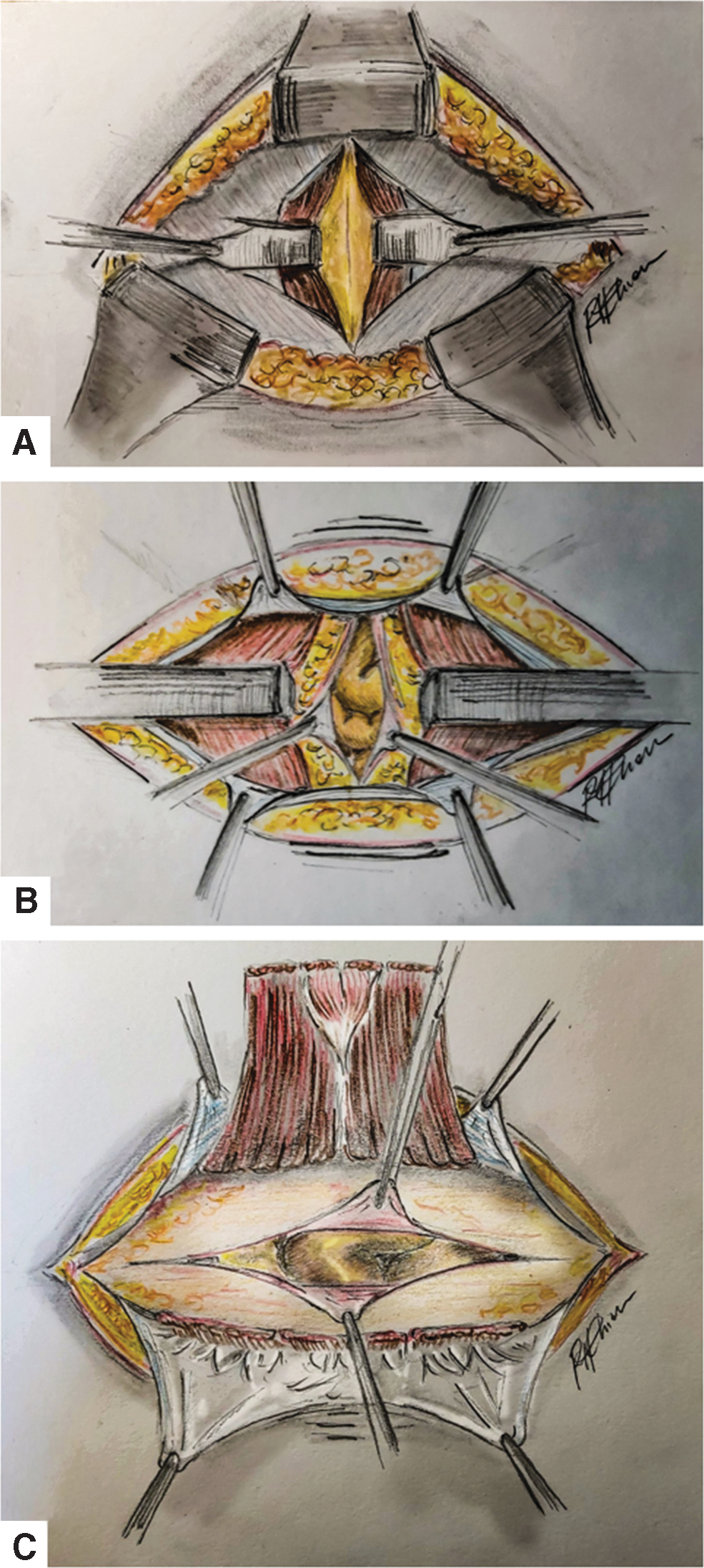
Different suprapubic incisions.
This study has few limitations, first of all for its retrospective nature and for the relatively small numbers of the cohorts considered. However, although great part of the literature concerning suprapubic accesses to the abdominal cavity were conducted in the field of gynecology (with the possible additional bias of muscular diastases secondary to pregnancy, also), this study is specifically for laparoscopic liver surgery.
Conclusion
In conclusion, there are several ways to accomplish a minimally invasive liver resection. The specimen extraction, according to its dimensions, can be obtained through site port enlargement, upper ML and PF incisions.
No differences in postoperative recovery from hemihepatectomies were observed between those patients whose specimen was retrieved through a PF or an ML incision at the end of a laparoscopic procedure. Therefore, both accesses can be used alternatively in laparoscopic liver surgery.
Footnotes
Authors' Contribution
Conception and design: L.A. and G.F.; Acquisition of data: F.C., F.R., G.F., and R.M.; Data analysis and interpretation: G.F. and F.R.; Article writing: G.F., R.M., and R.C.; Critical review for intellectual content: L.A., M.P., and M.C.; Final approval: all authors; All authors are accountable for all aspects of the work and ensure proper investigation and resolution on any question related to the accuracy or the integrity of the article.
Disclosure Statement
The material has not been previously published or submitted elsewhere for publication and will not be sent to another journal until a decision is made concerning publication. All listed authors have participated in the study and have approved the final version of the article. There are no personal conflicts of interest or financial disclosure for any of the authors. This study is not based on any previous communication to a society or a meeting.
Funding Information
No fundings were associated with the present study.