
Abstract
Background:
The management of primary liver tumors requires the involvement of multiple specialist skills and the best possible treatment in terms of cost, risk, and benefit that could be provided by hepatobiliary or transplant surgeon, interventional radiologist, hepatologist, radiotherapist, or oncologist is needed to be chosen for each patient. This is particularly relevant for hepatocellular carcinoma (HCC), that is the most common primary liver tumor, and it occurs in more than 90% of cases in the setting of cirrhosis.
Methods:
To address the increasing complexity of cancer care, multidisciplinary tumor boards (MDTBs) have evolved to offer patients appropriate and tailored cancer treatments. In Sicily (Italy), MDTBs have been organized in a Regional Network, the Sicily Network for Liver Cancer, that answers to the need for an equal and fair access to cancer care, to improve the diagnostic and therapeutic appropriateness, to ease patients care, to improve the efficacy of cancer treatments, and finally to optimize the risk-cost-benefit ratio of therapies and follow-up.
Results:
It has been shown that multidisciplinary management is associated with significantly improved survival in patients with liver cancer. In this study, we present the aims, the organization, and the current and future activities of the Sicily Network for Liver Cancer, an integrated health care multidisciplinary network for the management of patients with primary liver tumors in Sicily.
Conclusions:
The coexistence of two diseases (HCC and cirrhosis) requires the expertise of many physicians to provide optimal care to patients with HCC. Treatment decisions should be discussed in multidisciplinary meetings, as no single treatment strategy can be applied to all patients, and treatment must be individualized to improve overall survival of patients with liver tumors.
Introduction
Primary liver tumors have a worldwide incidence of more than 500,000 cases each year, and they are characterized by clinical and biological heterogeneity.1,2 Their management requires the involvement of multiple specialist skills, and for each patient, the best possible treatment in terms of cost, risk, and benefit that could be provided by hepatobiliary or transplant surgeon, interventional radiologist, hepatologist, radiotherapist, or oncologist is needed to be chosen. Among primary liver tumors, hepatocellular carcinoma (HCC) occurs in more than 90% of cases in the setting of cirrhosis, and it is related primarily to chronic infection with hepatitis B or hepatitis C virus (HCV), to alcohol abuse or to metabolic syndrome. Although hepatitis B viral suppression and hepatitis C eradication could reduce the risk of HCC, it persists in patients with cirrhosis and advanced fibrosis, especially when etiology of liver disease is not treated and when risk cofactors are present. The coexistence of two diseases (HCC and cirrhosis) requires a careful evaluation of the severity of liver impairment, the risk of liver decompensation associated with active treatments for HCC, and the potential impact of coexisting illnesses. The management of such a clinical complexity needs the active involvement of hepatologists for the diagnosis and treatment of the complications of cirrhosis and for the choice of etiologic treatments for chronic liver disease.3–6
The multidisciplinary approach for liver cancer
Given the complexity of the disease (in particular for the presence of chronic liver disease) and the large number of potentially useful therapies, it is not surprising that the expertise of many physicians is required to provide optimal care to patients with HCC. 7 Patients diagnosed with liver cancer should be referred to multidisciplinary teams, including hepatologists, gastroenterologists, surgical oncologists, transplant surgeons, medical oncologists, radiation oncologists, diagnostic radiologists, interventional radiologists, primary care physicians, palliative care physicians, and allied health professionals, all of whom should play an active role in the care of these patients (Fig. 1). Treatment decisions should be discussed in multidisciplinary meetings, as no single treatment strategy can be applied to all patients, and treatment must be individualized.
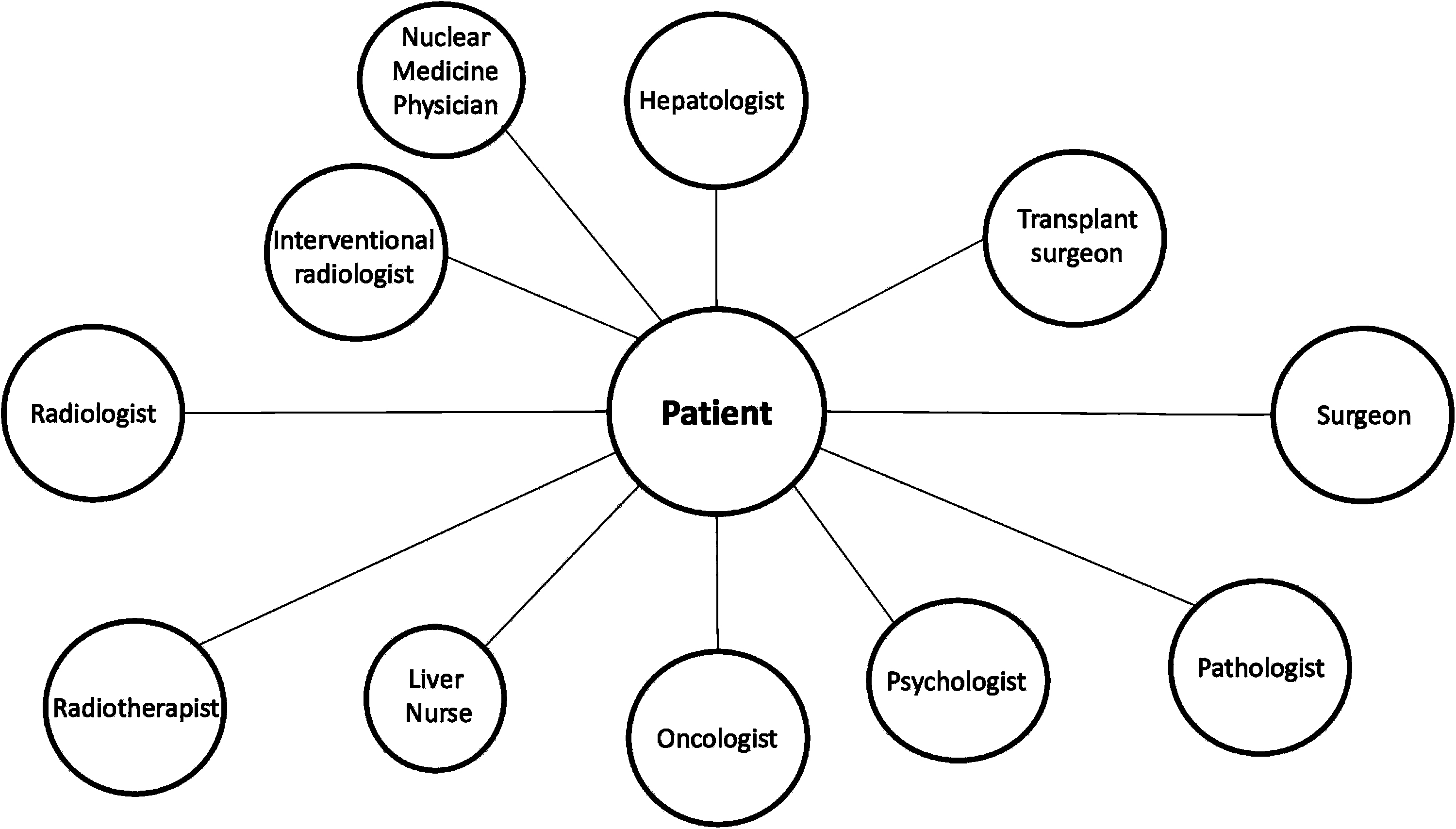
The multidisciplinary approach to the treatment of hepatocellular carcinoma.
If one considers the relevance of etiologic treatment of underlying chronic liver disease and the global evaluation of residual liver function in patients with cirrhosis, with or without portal hypertension clinically relevant, before any kind of treatment for HCC, then it clearly emerges the driving role of hepatologists in the multidisciplinary management of patients with HCC. In fact, the hepatologist represents the figure of reference and connection between all involved specialist professional figures, in all phases of the patient's clinical history, while the other members of the management group will assume, at different time, fundamental interventional roles, depending on the stage of the tumor and the choice shared therapy. This is particularly relevant considering that effective etiologic treatment is now available, especially in the setting of viral chronic liver diseases. Particularly, the use of direct-acting antiviral agents (DAAs) for the treatment of HCV infection is associated with a decrease of the risk of HCC occurrence and with an improvement in overall survival in patients with previous successfully treated early HCC.8,9
On the contrary, transplant surgeon plays a fundamental role in the management of patients with HCC, especially in transplantable patients, to identify the correct timing point for the inclusion in the transplant list, considering that liver transplant remains the most effective treatment for HCC and cirrhosis. As the number of available effective systemic treatments for HCC recently increased, including the advent of immunotherapy, the role of the clinical oncologist will be increasingly relevant, although it should be considered that cancer-related morbidity is frequently overshadowed by the complications of cirrhosis.
Obviously, the radiologist plays a relevant role in each phase of the patient's clinical history, both in the phase of the first diagnosis, as well as after the various treatments in the assessment of tumor response, and also considering the importance of the interventional radiologist in the management of many of the percutaneous and endovascular treatments.
Moreover, the multidisciplinary approach also more easily leads to multimodal cancer management.
Multimodal treatment for HCC can involve different modalities and treatment durations, and can be tailored according to the degree of liver function, the presence or absence of portal hypertension and the availability of different techniques. The number, location and size of lesions, the presence or absence of vascular invasion or extrahepatic spread, and tumor aggressiveness are also important factors to consider. Combination therapies can be categorized as either concomitant, meaning that the different treatments are carried out during the same session or at essentially the same time, or sequential, meaning that the elements of the combined treatment are carried out one after another. Either strategy aims to increase the efficacy of treatment compared with monotherapy, for example to prevent tumor recurrence, or (in the case of sequential therapy) to slow tumor progression and reduce tumor size in patients who are awaiting liver transplantation 7 (Table 1). In the setting of systemic therapy for advanced HCC, the combination therapy Atezolizumab plus Bevacizumab recently showed a significant survival benefit in comparison with monotherapy with Sorafenib in first-line. However, future studies are needed to assess whether a sequencing strategy rather than upfront combination could provide similar benefit. 10
The Proposed Purpose of Combination Therapy
To address the increasing complexity of cancer care, multidisciplinary tumor boards (MDTBs) have evolved to offer patients appropriate and tailored cancer treatments. It has been shown that the management of HCC patients with MDTBs was associated with a significantly higher 5-year survival rate compared to that of the patients who were not managed with MDTBs. 11
The implementation of MDTBs is also associated with increased referrals to surgery and to liver-directed therapy. 12 In Sicily (about 5 millions of inhabitants), Italy, 800–1000 new cases of HCC for each year are estimated using the data of Italian Association of Cancer Registry 13 and it should be considered that the estimates for cholangiocarcinoma, another primary liver tumor also requiring a multidisciplinary approach, should be added to these conservative estimates of incidence. In this setting of high clinical complexity, MDTBs identified as “liver oncology groups” have been created in Sicily and they have been organized in a Regional Network, the Sicily Network for Liver Cancer. The aim of this article is to profile the model of this Regional Cancer Network, focusing on purposes, expected results, and future perspectives.
Purposes and General Organization
The organization of the Sicily Network for Liver Cancer answers to the need for an equal and fair access to cancer care, to improve the diagnostic and therapeutic appropriateness, to ease patients care, to improve the efficacy of cancer treatments, and finally to optimize the risk-cost-benefit ratio of therapies and follow-up. The Regional Network is organized in multidisciplinary teams, called Liver Oncology Groups, which include physicians experienced in the management of chronic liver diseases and primary liver tumors (and professional figures such as psychologists, nutritionists, and nurses). A multidisciplinary approach is expected to offer the best from diagnostic-therapeutic possible options, directly or through the collaborations among the multidisciplinary groups, to standardize the management of more complex patients. In Sicily, the Regional Health Plan has planned Integrated Care Networks for oncological diseases to reduce inequalities in cancer care. One of the main advantages of these networks lies on the extensive use of information and communication technology 14 to overcome the care fragmentation and to provide patients and National Health Service more efficiency and a reduced waste of economic resources.
The “Hub-and-spoke” model has been chosen for this purpose. The hub-and-spoke organization model is designed to arrange delivery assets into a network consisting of anchor establishments (Hubs), which offer a full array of services, complemented by secondary establishments (Spokes) that offer more limited service arrays, routing patients needing more intensive services to the Hub for treatment. 15
This model is characterized by low congestion in referral facilities; increasing expertise among participant centers; the improvement in cooperation between physicians; minimal redundancy of health care services; uniformity in diagnosis, and treatment and in the measurement of results.
Finally, the aims of a health care network should be:
to allow the application of evidence-based medicine to clinical decision-making and to the stakeholders; to provide a level of care that is appropriate for the health care needs of a population; to allow to Regional Health Service the assessment of the quality of health outcomes in relationship with economic structures and health care delivery systems and the cost-effectiveness analysis of planned health care program, in a setting of Value Based Medicine.
16
In this line, a regionally shared Assisted Diagnostic and Therapeutic Pathway (PDTA) has been organized to improve diagnostic and therapeutic appropriateness for all the physicians involved in the management of primary liver tumors in Sicily. A regional PDTA should overcome the heterogeneity related to the different organizations of hospitals, with variable volumes of patients and different specialist skills available in each structure. This PDTA will be continuously updated based on current evidence to guarantee a uniform access to care for patients and reduce direct and indirect costs for the Regional Health System. In the short term, this approach could favor the access to therapy for all patients with primary liver tumors in Sicily through the correct allocation of health resources.
The Sicily Network for Liver Cancer will be organized in 5 Hub Centers and 30 Spoke Centers (Fig. 2). The Hub centers are equipped with a MDTB that can offer all the therapeutic options for patients with primary liver cancer and they are located in the three main Sicilian cities: Palermo (three centers, including the transplant center), Messina and Catania (one center for each city). The 30 Spoke centers are able to start a diagnostic and clinical workup and they can manage clinical and oncological follow-up of patients who underwent cancer treatment. They will be represented by Sicilian Oncology community centers and by the centers belonging to RESIST-HCV (Rete Sicilia Selezione Terapia—HCV), a web-based regional database that includes data on all patients with HCV liver disease treated with DAAs at Gastroenterology, Hepatology, Internal Medicine and Infectious Diseases community centers of Sicily. 17
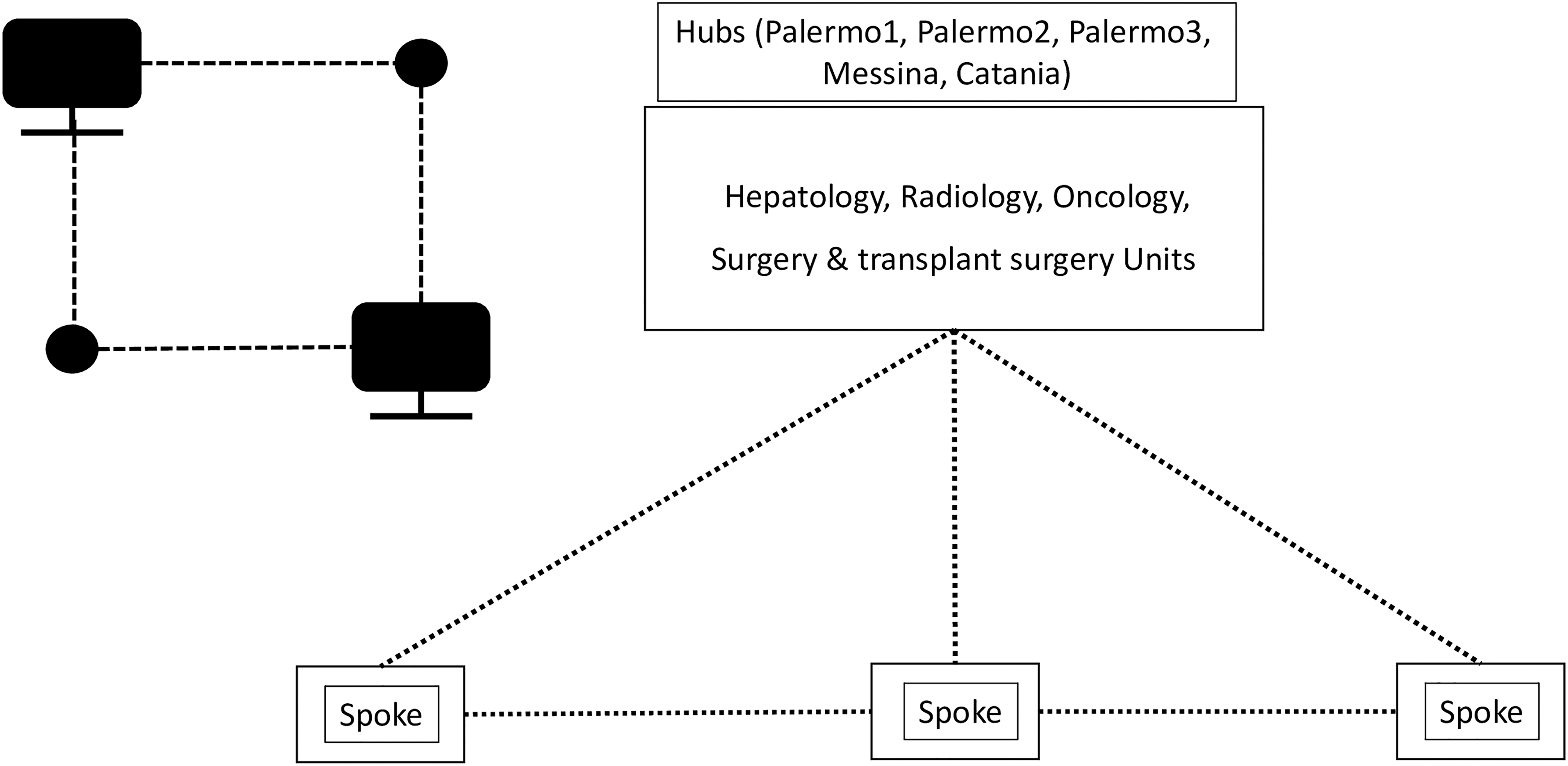
The Hub and Spoke centers of the Sicily Network for Liver Cancer.
Medical records of the patients with primary liver cancer will be registered in a web-based platform to assess the regional incidence during the first 3 years of study, the decision-making processes for diagnosis and treatment, the clinical outcomes related to cancer and to chronic liver disease, if present. A shared PDTA will be organized, shared, and implemented by physicians participating to the Network. It will include: the assessment of the stage and etiology of the liver disease, in terms of evaluation of the severity of liver impairment and portal hypertension; the radiological and histological assessment of the liver tumor; the assessment of coexisting illnesses; the choice of etiological therapies for underlying liver disease; the shared choice of cancer treatment, including liver transplantation; the assessment of the efficacy of the performed treatments; and the definition of the follow-up criteria. Telehealth technologies will be organized to reduce geographic barriers to access with liver cancer specific virtual tumor boards among the Hub centers and to plan the best treatment in the nearest center to the patient's residence. This is particularly relevant at this moment, in which, due to the COVID-19 pandemic, telemedicine by video call should be preferred to face-to-face meeting. 18
A picture archiving and communication system will be used to store the imaging at the diagnosis and during the follow-up of the patients included in the platform and to share radiological data among Hub Centers and the transplant center. This imaging-network will allow rapid access to imaging, maintaining appropriate quality standards and respect for health care privacy and it will be used for clinical research. Periodic reports on the efficiency of the network and on the diagnostic-therapeutic appropriateness of the interventions will be produced by designated working groups and a Steering Committee will be organized to process data and write scientific articles. The Steering Committee will be coordinated by scientific and management heads and each Hub center will appoint a representative. This committee will have scientific responsibility of the project and it will promote interaction protocols within the Hub centers and among the Hub and Spoke centers.
Network Activities
To improve the efficiency of the Network model and the ability to cooperate within working groups and among Hub and Spoke centers, team building and team working activities have been performed with the aim of realizing a multidisciplinary team coaching during the project development phase. The other main objective of these activities is to introduce and to spread the culture for a successful team, based on empathy, ongoing dialogue, and awareness of the team itself. Therefore, the introduction of a “network culture” is considered a priority for a successful team building. Multidisciplinary teams need to be guided by a managerial thinking that could favor an innovative leadership model. This kind of model is characterized by the transition from an early situational leadership to a subsequent empowering leadership phase. A psychosocial approach has been adopted, with the analysis and the discussion of the communication process within the team, focus groups, brainstorming, role play, and circle time. As a result, these teams require more resources, also time-consuming, than traditional teams, but they produce better results. The models used included multistakeholder approach, 19 plan-do-check-act PDCA models, 20 Ishikawa diagram, 21 and the “process effectiveness and efficiency” model. 22
To improve the cooperation among and within Hub centers, patients will be managed by the team coordinator of the Hub center, who will take care of the different diagnostic and therapeutic phases that the patient will encounter in the home center or in another center. At the same time, the Spoke centers will have the possibility to book visits or therapeutic procedures at the Hub centers through a web-based platform that will simplify and speed up the diagnostic and therapeutic workups of patients.
To implement and manage the flows of information, all the Network Centers will register medical records of their patients in a web-based platform. At the time of the registration, each patient will give its informed consent to allow the use for health purposes of personal and clinical data, which will then be encrypted in the registry. The physicians of each center will report personal and clinic data of the patients, including etiology and stage of liver disease, severity of portal hypertension and of liver impairment, radiological and histological diagnostic definition of the liver tumor, the indications for different treatments, the procedures needed for assessment and listing for liver transplantation, and finally the outcomes after treatment and during the follow-up. Flows of information will be analyzed every year to assess efficacy and appropriateness of performed treatments.
Expected Results
Through the registration of data of all the patients with primary liver cancer, the Sicily Network for Liver Cancer will allow to elaborate epidemiological data and to provide a geolocation report of liver cancer in Sicily. The application of a regionally shared PDTA will allow improving diagnostic and therapeutic appropriateness, rationalizing professional and economic resources. This model will avoid the redundancy of health services and it will speed up diagnostic and therapeutic processes. The network will facilitate the access to care in the nearest center to the patient's residence, with the aim of reducing intra- end interregional health tourism and its related costs. A more rationale choice of the therapy, which should be based on evidence, will allow reducing the overall costs of cancer treatment.
Finally, the model will provide the opportunity to spread the scientific activities of the network to citizenship. This could increase confidence in regional health structures and the publication of real-world evidence studies as a result of an institutional research project of cooperation among high specialization centers will lead to the production of new scientific evidence. 23
Final Considerations
The multidisciplinary approach can provide patients with liver cancer the benefit of different specialties actively involved in the treatment planning and it is definitively recognized as the standard of care for the treatment of cancer patients. 24
It can be done through multidisciplinary clinical centers, where all the potential treatment available are feasible, and through network models connecting these centers to each other and to the peripheral centers. Mounting evidence showed that multidisciplinary management is associated with a higher likelihood of receiving an active cancer treatment and with significantly improved survival in patients with liver cancer, both in western25,26 and in eastern world. 11
It has been demonstrated that the multidisciplinary team approach could be more beneficial in patients with more complex clinical conditions, such as poorer liver function or aggressive tumor pattern, and it is not surprising as multidisciplinary approach seems to be more beneficial when things are more complicated. 27
Furthermore, this kind of approach is particularly requested for the management of liver cancer, as multiple treatments are available and offered by a host of different providers. At the same time, web-based platforms connecting Hub and Spoke centers have been already developed in the Sicilian context, particularly the RESIST-HCV that was designed to improve the management and the treatment of HCV chronic hepatitis and cirrhosis and to manage DAA treatment prescriptions in accordance with guidelines and therapeutic appropriateness. This network still represents an excellent system to provide Regional Department of Health a real estimation of patients that received efficacy, high-cost therapies, and finally to improve patient care. In conclusion, we presented the aims, the organization, and the current and future activities of the Sicily Network for Liver Cancer, a newly established integrated health care multidisciplinary network for the management of patients with primary liver tumors in Sicily. The results of the upcoming network activities and the results of the periodical efficacy analyses will be reported in future publications.
Footnotes
Disclosure Statement
This article has not been published and is not under consideration elsewhere. We declare that all authors are in agreement on the content of the article and have no potential conflicts of interest.
Funding Information
No funding was received for this article.