
Abstract
Introduction:
Laparoscopic treatment of gastric cancer in elderly patients is still controversial. The aim of this retrospective study is to evaluate the safety and feasibility of laparoscopic gastrectomy in elderly gastric cancer patients based on the long- and short-term results of laparoscopic surgery.
Materials and Methods:
The data of 163 patients who underwent laparoscopic gastrectomy for gastric cancer. Patients were categorized into two groups by age based on World Health Organization (WHO) criteria: elderly (≥65 years, 80 cases) and nonelderly (<65 years, 83 cases). Patient characteristics and clinicopathological findings, surgical findings, short- and long-term results were compared between the two groups.
Results:
The patients in the study group were in the age range of 22–87 years and 80 (49%) patients were found out to be 65 years old or older. When all complications were categorized according to Clavien–Dindo (C-D) classification, >3 serious complication rates were similar between groups (P = .421). Although the length of hospital stay and the need for intensive care were higher in the elderly group, the difference was not significant (P = .066; P = .072). There was no significant difference between the two in terms of in-hospital mortality (P = .364). No statistically significant differences were found in the rates of overall survival (nonelderly group; 61.17 ± 3.34, 95% confidence interval [CI]: 54.61–67.74 versus elderly group; 56.48 ± 3.80, 95% CI: 49.03–63.93; P = .176) and disease-specific survival (nonelderly group; 64.24 ± 3.15, 95% CI: 58.06–70.40 versus elderly group; 61.93 ± 3.57, 95% CI: 54.93–68.93; P = .363) between the age groups.
Conclusion:
In conclusion, although laparoscopic gastrectomy is a feasible and safe method in elderly gastric cancer patients, further randomized prospective studies are needed.
Introduction
Gastric cancer is one of the most common causes of cancer deaths in the world. 1 The rapid aging of the global population causes ∼60% of cancer cases and 70% of cancer-related deaths in individuals over the age of 65. 2 The risk of developing gastric cancer rises in line with increasing age. Although there are several criteria for identifying a patient as an elderly person, the World Health Organization (WHO) defines individuals at the age of 65 or over as elderly.3,4 Elderly patients constitute a population at a high risk of perioperative morbidity and death because of low functional reserves and a high number of comorbidities.5–7 Previous studies have reported high postoperative morbidity and mortality in elderly gastric cancer patients, who underwent open gastrectomy.8–11 Therefore, it is important to determine the optimal surgical technique for the treatment of gastric cancer in elderly patients.
After its first use by Kitano et al. in 1994, 12 laparoscopic gastrectomy has become the standard technique for operating early gastric cancers and an increasingly preferred technique for advanced gastric cancers in recent years. Many studies have reported several advantages of laparoscopic surgery over conventional open surgery such as less postoperative pain, less blood loss, shorter hospital stays, and rapid normalization of bowel movements.13–17 These advantages have brought forward the use of laparoscopic gastrectomy more frequently in elderly patients, leading several studies to investigate this subject matter.18–20 In the literature, the number of studies arguing that laparoscopic distal gastrectomy should be the preferred technique in elderly gastric cancer patients has been increasing.21–24 However, comprehensive studies investigating the feasibility of laparoscopic total gastrectomy in elderly patients are less common. On the other hand, the use of the laparoscopic technique in elderly patients with multimorbidity continues to be a question of debate because of several reasons such as long operative times and circulatory and respiratory system disorders induced by the CO2 pneumoperitoneum in laparoscopic gastrectomy. 25
This study aimed to discuss the usability and safety of laparoscopic gastrectomy in elderly patients and to assess the short and long-term postoperative outcomes.
Materials and Methods
Our study was carried out in compliance with the ethical principles of the Declaration of Helsinki. This retrospective study was approved by the Ethics Committee of Ankara University Medical Faculty (Decision no: İ4-248-20). The data of 163 patients, who underwent laparoscopic gastrectomy for gastric cancer in the Surgical Oncology Clinic of Ankara University Medical Facultyin the period between January 2014 and January 2020, were retrospectively studied. The operations were performed by 4 surgeons.
We categorized patients into two groups by age based on the WHO criteria: elderly patients (≥65 years old, 80 cases) and nonelderly patients (<65 years old, 83 cases). The criteria for inclusion in the study were as follows: patients with a preoperative diagnosis of histologically proven gastric adenocarcinoma; there was no missing patient data; the type of the operation, including conversion to intraoperative laparotomy was laparoscopic gastroscopy; D2 lymph node dissection was performed; absence of distant metastases; and R0 resection was performed depending on surgical and pathological findings. On the other hand, the exclusion criteria were as follows: patients diagnosed with other malignant tumors such as gastric lymphoma, neuroendocrine tumors, squamous cell carcinoma, stromal tumors in the preoperative or postoperative pathological examination; patients who underwent combined organ resection; having a history of comorbid malignant tumors; and missing data.
Patient characteristics, clinicopathological findings, surgical findings, and the short-term and long-term outcomes were compared between the two patient groups. The clinicopathological findings of the patients were evaluated according to the Japanese Classification of Gastric Carcinoma (3rd English edition) published by the Japanese Gastric Cancer Association (JGCA). 26 The evaluation of patient characteristics and clinicopathological findings included the analysis of age, gender, body mass index (BMI), albumin levels, American Society of Anesthesiologists (ASA) scores, comorbidities, preoperative diagnoses of early or locally advanced gastric cancers, and pathological stages. In this study, comorbidities were evaluated in the following four different categories: cardiovascular diseases, diabetes mellitus (DM), chronic obstructive pulmonary disease (COPD), and other diseases (cerebrovascular events, chronic kidney failure, chronic liver disease).
The following surgical findings were evaluated: the surgical technique (total or distal gastrectomy), conversion to open surgery, operative time (minutes), blood loss, the requirement for blood transfusions, and the total number of dissected and metastatic lymph nodes. On the other hand, the short-term outcomes were evaluated using the following findings: 30-day postoperative morbidity, mortality, the overall length of hospital stay, the length of stay in the intensive care unit (ICU), and the time to start oral intake.
Postoperative morbidity was classified under the following four categories: surgical complications, cardiovascular complications, pulmonary complications, and acute kidney failure (AKF). Anastomotic leaks, duodenal stump leakage, intraabdominal abscesses, hematoma, ileus, surgical site infection, intestinal ischemia, and trocar site hernia were included in surgical complications; atelectasis, pleural effusion, pneumothorax, pneumonia, and acute respiratory distress syndrome were included in lung complications; acute heart failure, myocardial infarction or cardiopulmonary arrest, and atrial fibrillation were included in cardiac complications, and they were categorized according to the Clavien–Dindo classification. 27 Moreover, overall survival and disease-specific survival findings were evaluated as long-term outcomes, and these findings were compared between the two groups.
Statistical analysis
All data were presented as mean ± standard deviation. Kolmogorov–Smirnov test and histograms were used to test the normality of the data. In the comparison of demographic characteristics, surgical findings, and postoperative outcomes between the two age groups, the χ 2 test and Fisher's exact test, were used for the categorical data whereas Student's t-test and Mann–Whitney U test were used for the numerical data. The Kaplan–Meier survival analysis was performed to compare overall and disease-specific survival among the age groups. All P values of <.05 were considered significant. We used IBM SPSS Statistics version 23.0 as the statistical software for data analysis.
Results
The ages of the patients in the study group ranged between 22 and 87 years, and 80 (49%) patients were found to be at the age of 65 or above. The patients were divided into two groups: patients below the age of 65 and those at the age of 65 and above. The comparison of the clinicopathological variables between the two groups revealed no significant differences in terms of gender, BMI, TNM stage, and preoperative disease stages. The group of elderly patients was observed to have statistically significantly higher ASA scores and lower preoperative albumin levels (P < .001; P < .001). Among the comorbid diseases, DM and cardiovascular diseases were observed to be significantly more common in the group of elderly patients (P < .001; P < .001). The relationship between the clinicopathological variables and the age groups is summarized in Table 1.
Comparison of Patient Characteristics in Elderly and Nonelderly Groups
Values are expressed as means ± standard deviation, or n (%).
ASA, American Society of Anesthesiologists; BMI, body mass index; COPD, Chronic obstructive pulmonary disease.
No significant differences were found between the groups in terms of the type of surgery, the number of positive lymph nodes, rates of conversion to laparotomy, intraoperative blood loss, and the requirement for blood transfusions. It was observed that the number of dissected lymph nodes was significantly lower in the group of elderly patients (P = .004). However, no significant difference was observed between the two groups in terms of the number of metastatic lymph nodes (P = .308). Although the operative times were longer in the group of elderly patients, the difference between the two groups was not statistically significant (P = .087). The relationship between the surgical findings and the age groups is summarized in Table 2.
Comparison of Operative Findings in Elderly and Nonelderly Groups
Values are expressed as mean ± standard deviation, or n (%).
The analysis of the overall postoperative complications under the surgical complications, cardiovascular complications, pulmonary complications, and AKF categories revealed no significant differences between the two age groups in terms of the incidence of complications. When all complications were categorized according to the Clavien–Dindo classification, the groups showed similar rates of severe complications with grade >3 (P = .421). In-hospital mortality of the patients was considered the postoperative 30-day mortality. The statistical analysis revealed no significant difference between the two groups in terms of in-hospital mortality (P = .364). Although the length of hospital stay and the requirement for intensive care were higher in the group of elderly patients, the difference between the two groups was not statistically significant (P = .066; P = .072). The relationship between the short-term postoperative outcomes and the age groups is summarized in Table 3.
Comparison of Postoperative and Short-Term Outcomes in Elderly and Nonelderly Groups
Values are expressed as mean ± standard deviation, or n (%).
ARDS, acute respiratory distress syndrome; CP, cardio pulmonary; ICU, intensive care unit.
The follow-up time in the study ranged between 0.1 and 75.7 months. The cumulative survival rates in the first, third, and fifth years were found to be 84.9%, 79.7%, and 72%, respectively. The overall survival and disease-specific survival rates in the study population were found to be 58.69 ± 2.58 (95% confidence interval [CI]: 53.63–63.76) and 62.93 ± 2.43 (95% CI: 58.16–67.71) months, respectively. No statistically significant differences were found between the age groups in the rates of overall survival (nonelderly group: 61.17 ± 3.34, 95% CI: 54.61–67.74 versus elderly group: 56.48 ± 3.80, 95% CI: 49.03–63.93; P = .176) and disease-specific survival (nonelderly group: 64.24 ± 3.15, 95% CI: 58.06–70.40 versus elderly group: 61.93 ± 3.57, 95% CI: 54.93–68.93; P = .363). The Kaplan–Meier curves comparing the overall and disease-specific survival in the two age groups are presented in Figures 1 and 2.
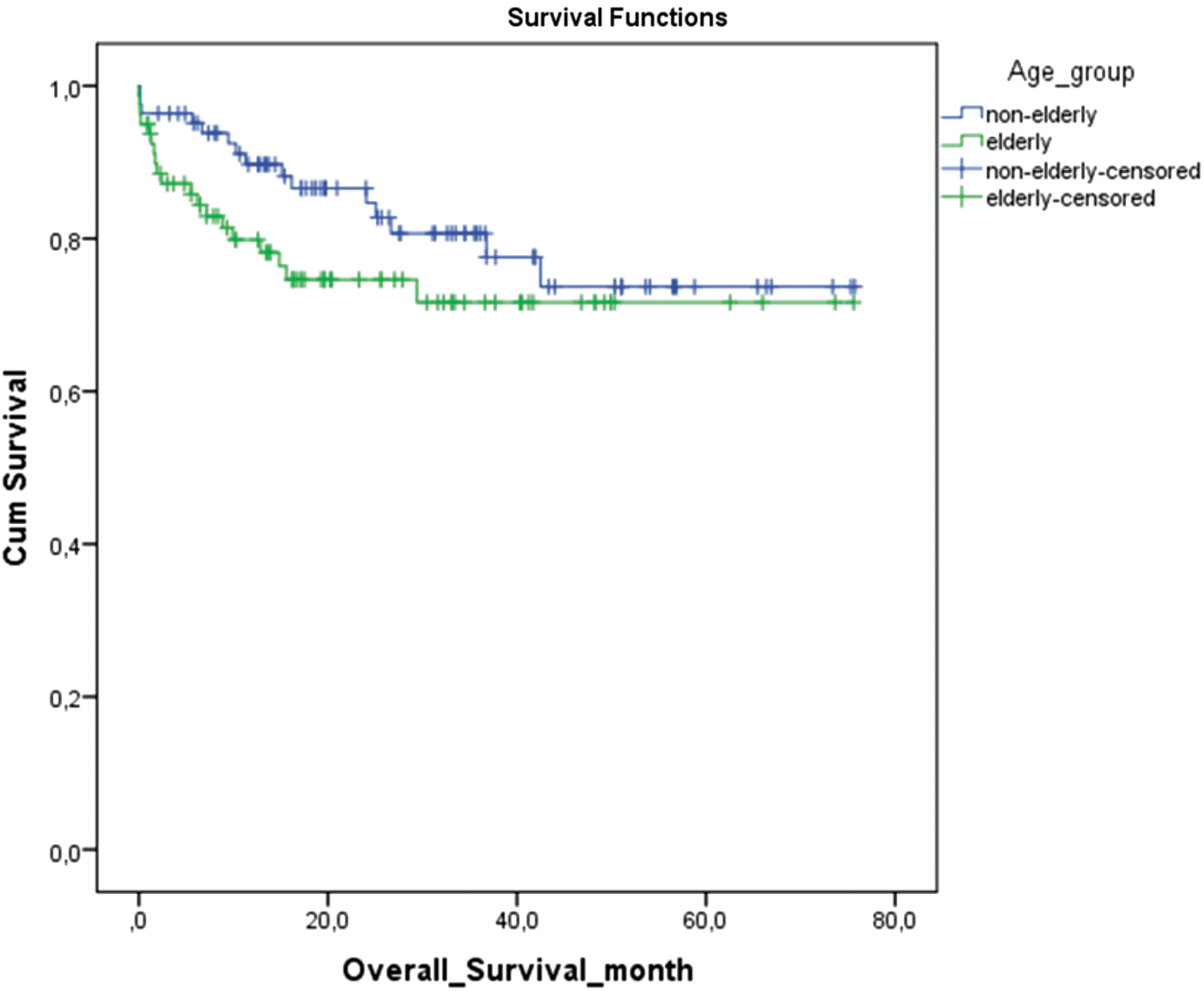
Comparison of overall survival rates after laparoscopic gastrectomy for gastric cancer between elderly group (≥65 years) and nonelderly group (<65 years) (P = .176).
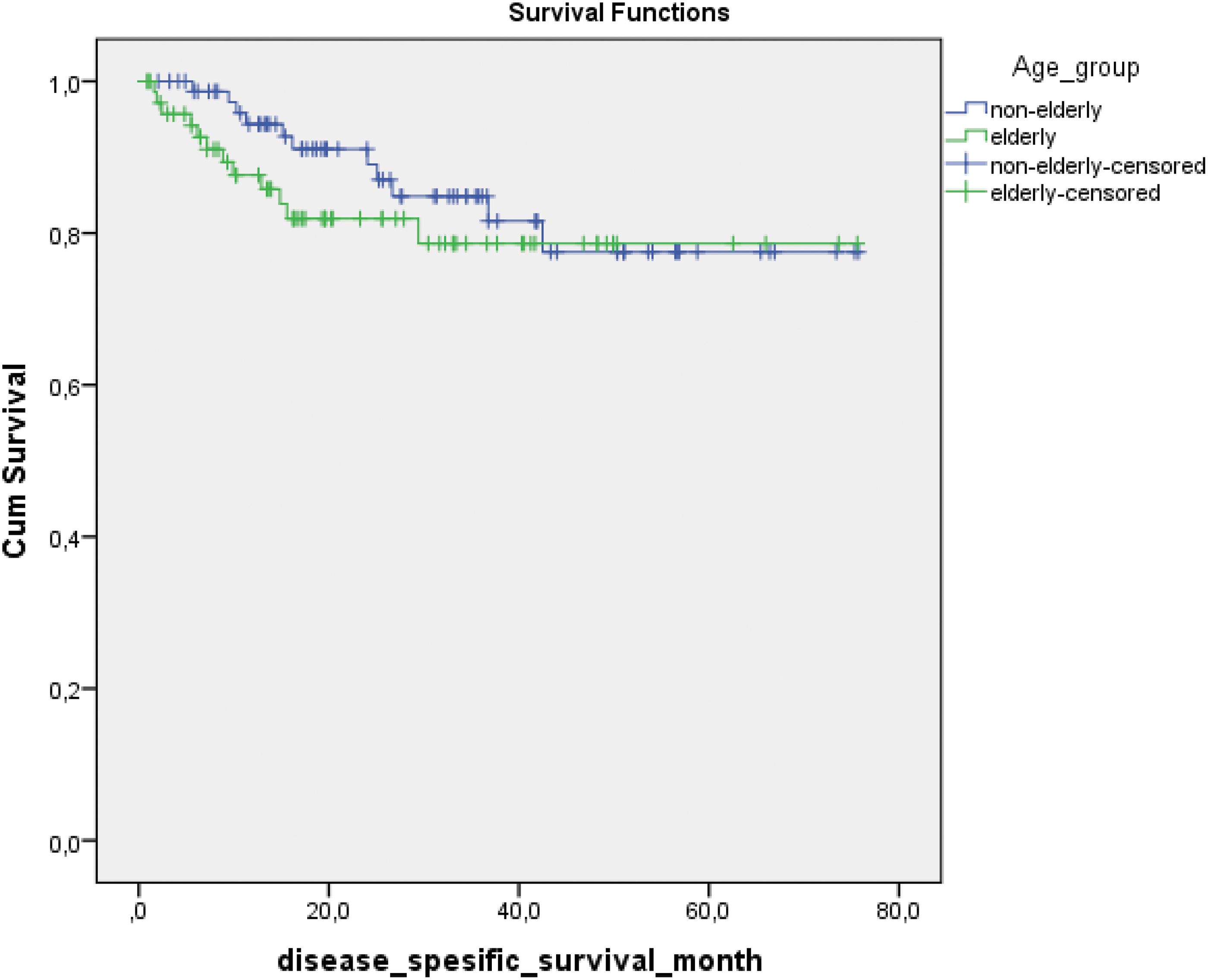
Comparison of overall survival rates after laparoscopic gastrectomy for gastric cancer between elderly group (≥65 years) and nonelderly group (<65 years) (P = .363).
Discussion
Today, old age is considered a risk factor for surgery.28–30 Surgeons tend to prefer safer and less traumatic surgery because of the limited functional reserve and high incidence of comorbidity in elderly patients. However, along with the recent improvements in surgical technology and perioperative nursing standards, elderly patients have become able to tolerate major surgical interventions better.31,32 Consequently, laparoscopic surgery has become a rapidly developing minimally invasive technique for gastric cancer operations, and its application to elderly patients has been increasing. The advantages of laparoscopic gastrectomy, including the use of a small incision, less postoperative pain, less blood loss, early start of oral intake, and short periods of inpatient hospital stay paved the way to the theoretical consideration that this technique is usable in elderly gastric cancer patients.14,16 Considering the trauma due to surgery, laparoscopic gastrectomy can be the optimal choice for the minimization of surgical trauma in elderly patients. Several studies have been conducted recently on laparoscopic subtotal gastrectomy and its short-term outcomes in elderly gastric cancer patients.33–35 There are few studies in the literature discussing laparoscopic total gastrectomy and its long-term outcomes in elderly patients with gastric cancer.36,37 The creation of CO2 pneumoperitoneum during laparoscopic surgery reduces the volume of the thoracic cavity and decreases pulmonary compliance. Furthermore, the long duration of high pressure in the abdominal cavity causes stasis and reflux in visceral veins and veins of body cavities. Consequently, this may lead to postoperative infectious complications by impairing liver function and the intestinal mucosal barrier. 38 Assuming that cardiac and respiratory comorbidities are more common in elderly patients, high rates of these negative effects of laparoscopy may be more frequently seen in these patients. Therefore, the safety and usability of laparoscopic gastrectomy, including cases with total gastrectomy, in elderly gastric cancer patients remains uncertain. In the present retrospective study, the elderly and nonelderly patient groups, who underwent laparoscopic gastrectomy for gastric cancer, were compared in terms of their clinicopathological and surgical findings, short-term and long-term outcomes.
In previous studies on gastric cancer surgery in elderly patients, several different age criteria were used, for example, Hwang et al. and Cho et al. used the age criteria of ≥70 years,33,34 Eguchi et al. and Orsenigo et al. used the age criteria of ≥75 years,39,40 and Mita et al. and Takeuchi et al. used the age criteria of ≥80 years.41,42 In the present study, we defined the elderly patient group as individuals ≥65 years old based on the WHO criteria.3,4 Elderly patients are usually more likely to have comorbidities that may be associated with postoperative morbidities, such as cardiovascular diseases, DM, or COPD. In the present study, no significant differences were detected between the elderly and nonelderly groups in terms of surgical complications other than hemorrhage (hematoma), despite the significantly higher ASA scores, comorbidity rates, and low albumin levels in the elderly group. The high rate of hemorrhage in the elderly group (P = .004) was attributed to the potentially more common use of anticoagulant drugs in these patients. Consistent with the results of this study, Shimada et al. also did not find any differences in surgical complication rates other than those of hemorrhage in their study. 43 In our study, pulmonary complications such as atelectasis and pleural effusion were found to be significantly higher in elderly patients (P = .003).
Several studies have shown old age as a risk factor for pulmonary complications.6,44 In our study, no significant differences were found between the two groups in terms of postoperative cardiac and renal complications. Although the frequency of postoperative morbidities in the elderly patients with Clavien–Dindo grade ≥3 is higher, no significant differences were found between the two groups (elderly group versus nonelderly group: 21.3% versus 15.7%; P = .421). Similar results have been found in previous studies. 43 In this study, a significant difference was not found between the two groups in terms of in-hospital mortality. Ciesielski et al. reported that the rate of in-hospital mortality was higher in elderly gastric cancer patients who underwent open radical gastrectomy. 30 Despite this high mortality rate reported for open gastrectomy, the results of several studies in the literature are consistent with the present study reporting no differences between elderly and nonelderly patients in terms of laparoscopic surgery-associated mortality.4,36,43
Despite longer hospital stays and ICU stays of the elderly patients in our study, this difference between the two groups was not found significant. These results are consistent with those reported by previous studies.36,43
Examining the surgical findings of the patients, no differences were found between the groups in terms of the type of surgery, the number of positive lymph nodes, rates of conversion to laparotomy, intraoperative blood loss, and the requirement for blood transfusions. The number of dissected lymph nodes was found to be significantly lower in the elderly patient group (P = .004). This result may be due to the tendency to perform limited lymph node dissection in elderly patients to not prolong the operative time considering the lower performance status and the functional reserves in elderly patients. In laparoscopic gastric cancer surgery, conversion to laparotomy is inevitable.45–47 In the literature, it is reported that the rate of conversion to laparotomy in laparoscopic total gastrectomyvaries between 3% and 15%.48–53 Similar to the results of previous studies, in this study, the rate of conversion to laparotomy was found to be 5% and 3% in the elderly and nonelderly groups, respectively. Most of the cases of conversion to laparotomy resulted from adhesions, bulky tumors, and uncontrolled bleeding.
The follow-up time was found to range between 0.1 and 75.7 months in this study. The overall survival and disease-specific survival were evaluated in terms of long-term outcomes. In this study, the overall survival (nonelderly group: 61.17 ± 3.34 versus elderly group: 56.48 ± 3.80; P = .167) and the disease-specific survival (nonelderly group: 64.24 ± 3.15, 95% CI: 58.06–70.40 versus elderly group: 61.93 ± 3.57; P = .363) values of the two groups were similar. This finding might have resulted from the fact that most patients in our study had early gastric cancer. In a multicenter retrospective study performed by Italian researchers, 5-year overall survival was reported to be low for the elderly patients, who underwent curative open gastric resection. 32 Lower rates of overall survival in elderly patients were associated with high rates of comorbidity-related mortality. 54 Today, there are still concerns about long-term outcomes of laparoscopic gastrectomy in elderly gastric cancer patients. Several previous studies reported that oncological outcomes of laparoscopic gastrectomy were as favorable as those of open gastrectomy. 55 In the studies by Mohri et al. and Shimada et al., disease-specific survival rates in elderly and young gastric cancer patients who underwent laparoscopic gastrectomy were similar.21,43 In the study by Sheng et al., the overall survival outcomes were consistent with the results of our study. 36
This study has some limitations. First, it is a single-center study with a retrospective design. Second, the sample size is small. Third, the operations were performed by different surgeons (by 4 surgeons). Therefore, the results might have been affected by such factors. It is necessary to consider all these factors when interpreting the results of this study.
Conclusions
In conclusion, laparoscopic gastrectomy was found to be a safe and usable technique in elderly gastric cancer patients based on the short-term and long-term outcomes observed in this study. The high perioperative mortality rates observed in conventional radical gastrectomy operations were not observed in laparoscopic gastrectomy patients. Although the approach of conventional surgeons is that laparoscopy is disadvantageous in elderly patients, the results of this study reveal the need to tend to laparoscopic methods for gastrectomy, particularly in elderly patients. However, despite the promising results obtained from the present study, larger-scale, randomized, prospective studies and reviews of these studies are needed.
Footnotes
Acknowledgment
We thank all members of the Turkish Surgical Oncology Association who supported the writing of this article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.