
Abstract
Background:
Colectomies performed according to complete mesocolic excision with central vascular ligation (CME-CVL) principles have been associated with enhanced oncologic outcomes. Nonetheless, laparoscopic CME-CVL right hemicolectomy has not been widely adopted. We aimed to compare the perioperative and pathology outcomes of laparoscopic and open CME-CVL right hemicolectomy.
Materials and Methods:
We compared data from a prospectively collected database regarding patients who underwent either laparoscopic or open CME-CVL right hemicolectomy for nonmetastatic right colon cancer in a University Hospital, between January 2012 and December 2018.
Results:
A total of 130 consecutive patients were included in the study. Of them, 73 patients underwent laparoscopic and 57 patients open right colectomy, following the CME-CVL principles. The laparoscopic approach was associated with less hospital stay (6.6 versus 9.1 days; P < .001) and septic complications (P = .046), at a cost of an increased operative time (180 versus 125.1 minutes; P < .001). Patients treated with either open or laparoscopic approach presented similar outcomes regarding pathology endpoints. In fact, both groups demonstrated similar R0 resection rate (P = .202), number of harvested and positive lymph nodes (P = .751 and P = .734, respectively), number of harvested lymph nodes at the level of D1 and D2 lymph node dissection (P > .05), rate of vascular (P = .501), and perineural infiltration (P = .956). Furthermore, no difference was found regarding the rate of intact mesocolic plane (P = .799), along with the tumor diameter (P = .154) and the length of specimen (P = .163).
Conclusion:
Laparoscopic CME-CVL right hemicolectomy appears to offer certain advantages in short-term outcomes compared to open procedure. Pathology outcomes did not differ between the two approaches. Future studies should further evaluate their long-term outcomes.
Introduction
Colorectal cancer is very common and one of the leading cancer-related causes of death worldwide. 1 Despite the advances in multimodal treatment, the disease is still associated with moderate prognosis. 2 Within this context, the standardization of the surgical management of colon cancer (CC), along with the evaluation of feasibility and safety issues, remains a matter of great importance.
Right hemicolectomy represents the standard surgical strategy regarding right-sided colonic tumors, and it may be performed through an open, laparoscopic or robotic approach. In the past, both open and laparoscopic techniques seem to provide comparable long-term and oncologic outcomes.3–5 Nonetheless, there is certain evidence indicating that the laparoscopic technique is associated with enhanced short-term outcomes in terms of perioperative blood loss and length of hospital stay (LOS) despite the higher technical difficulty level.6,7 However, the introduction and implementation in several centers during the last decade of complete mesocolic excision (CME) with central vascular ligation (CVL) raised another debate in the surgical management of CC, especially for the right colon.8–10 Two are the main components of the CME-CVL strategy: (i) the surgical dissection along the embryological planes, thereby preserving the integrity of the mesocolon and (ii) the central ligation of the supplying vessels at their origin, through an extensive colonic mobilization.11,12 The CME-CVL principles allow an extensive, oncologic bowel resection, an adequate mesocolic excision, along with an increased number of harvested lymph nodes relevant to the lesion.10,13
Despite the growing adoption of the CME-CVL principles in CC surgery, there is only limited evidence regarding its implementation in western centers.14,15 In addition to that, the increased technical difficulty that CME-CVL concept poses in the open technique, is anticipated to be even more exaggerated in laparoscopy. As there is lack of solid evidence regarding the comparison between open and laparoscopic right colectomy in the CME-CVL era, we analyzed our short-term and pathology outcomes of our experience with this concept to evaluate if we can safely reproduce the open CME technique with laparoscopy.
Materials and Methods
Patients selection
Ethical approval was obtained by the Scientific Committee of the University Hospital of Larissa, protocol number: 33606/16-07-19.
The present study is a single-center, retrospective study conducted according to STROBE checklist (Supplementary Data), incorporating patient data from a prospectively collected database regarding consecutive laparoscopic and open CME-CVL hemicolectomies for CC located between cecum and hepatic flexure. All the procedures were performed by the same surgical team leading by the senior author (G.A.T.) at the Department of Surgery, University Hospital of Larissa, Greece, between January 2012 and December 2018. Patients with preoperative evidence of metastatic disease or T4 lesions were excluded from the study. All the procedures, either open or laparoscopic, were performed following the CME-CVL principles. The choice between open or laparoscopic approach was depended either upon patient's preference (many people in Greece believe that laparoscopic colectomy is still somewhat “experimental”) or logistics (time/theater space, availability of disposables etc.).
Surgical technique
Both techniques were performed following the CME-CVL principles. 9 For the open technique, a lateral to medial approach was used to separate the dorsal mesocolic fascia from the retroperitoneal one at Toldt's fused fascia, entering into the so called embryological avascular plane of dissection. The Gerota's fascia, duodenum, and pancreatic head were fully exposed and the dissection was completed by revealing the outer/anterior aspect of the superior mesenteric vein. The ileocolic and right colic vessels were ligated at their origin, so the whole fatty lymphovascular tissue of mesocolon to the right of the superior mesenteric vein was removed intact.
For the laparoscopic technique, we adopted the medial to lateral approach, entering the aforementioned embryological avascular plane by opening the mesocolic fascia below the ileocolic trunk. The dissection into this plane was advanced cranially, laterally, and medially exposing fully again Gerota's fascia, duodenum, and pancreatic head and ending at the lateral/anterior aspect of the superior mesenteric vein. The vessels were again ligated at their origin and the specimen was removed through a small extension of the umbilical trocar site up to 5 cm with the assistance of a wound protector. A side to side isoperistaltic ileotransverse anastomosis was performed either intracorporeally or (more often) extracorporeally through the small transumbilical incision, which was used for the specimen extraction.
Primary and secondary endpoints
All data regarding baseline characteristics, pathologic characteristics, and perioperative outcomes were prospectively collected in an electronic dataset by a member of the surgical team. The parameters evaluated for comparison between the two groups included mortality, 30-day postoperative morbidity, and the pathology outcomes (quality of mesocolic dissection and integrity of the mesocolon, rate of R0 resections, number of harvested and positive lymph nodes, vascular and perineural infiltration). R0 resection was considered when a negative circumferential resection margin of more than 1 mm was achieved. Complications were graded according to the Clavien–Dindo classification 16 accounted for all adverse events occurring in-hospital or within 30 days after surgery. Finally, the learning curve regarding the laparoscopic approach was also evaluated.
Statistical analysis
The results were analyzed using GraphPad Prism 8.0 for Mac (GraphPad Software, San Diego, CA). Normal distribution of the data was performed by application of the D'Agostino and Pearson Omnibus normality test. Comparisons of continuous variables were performed with two-tailed unpaired t-test for parametric data and Mann–Whitney U-test for nonparametric data. The categorical outcomes were tabulated in 2 x 2 tables and were assessed by performing the chi-square test. The learning curve regarding the laparoscopic CME-CVL right colectomy was evaluated by performing the Kruskal–Wallis test. Differences were deemed significant with a P ≤ .05.
Results
Baseline characteristics
The Trial Flow regarding the data extraction strategy is demonstrated in Figure 1. A total of 130 patients were included (laparoscopic group: 73 patients; open group: 57 patients). Patients' baseline characteristics are presented in Table 1. Notably, the study population in both groups was homogeneous, without any significant difference regarding the demographic and clinical characteristics being detected.
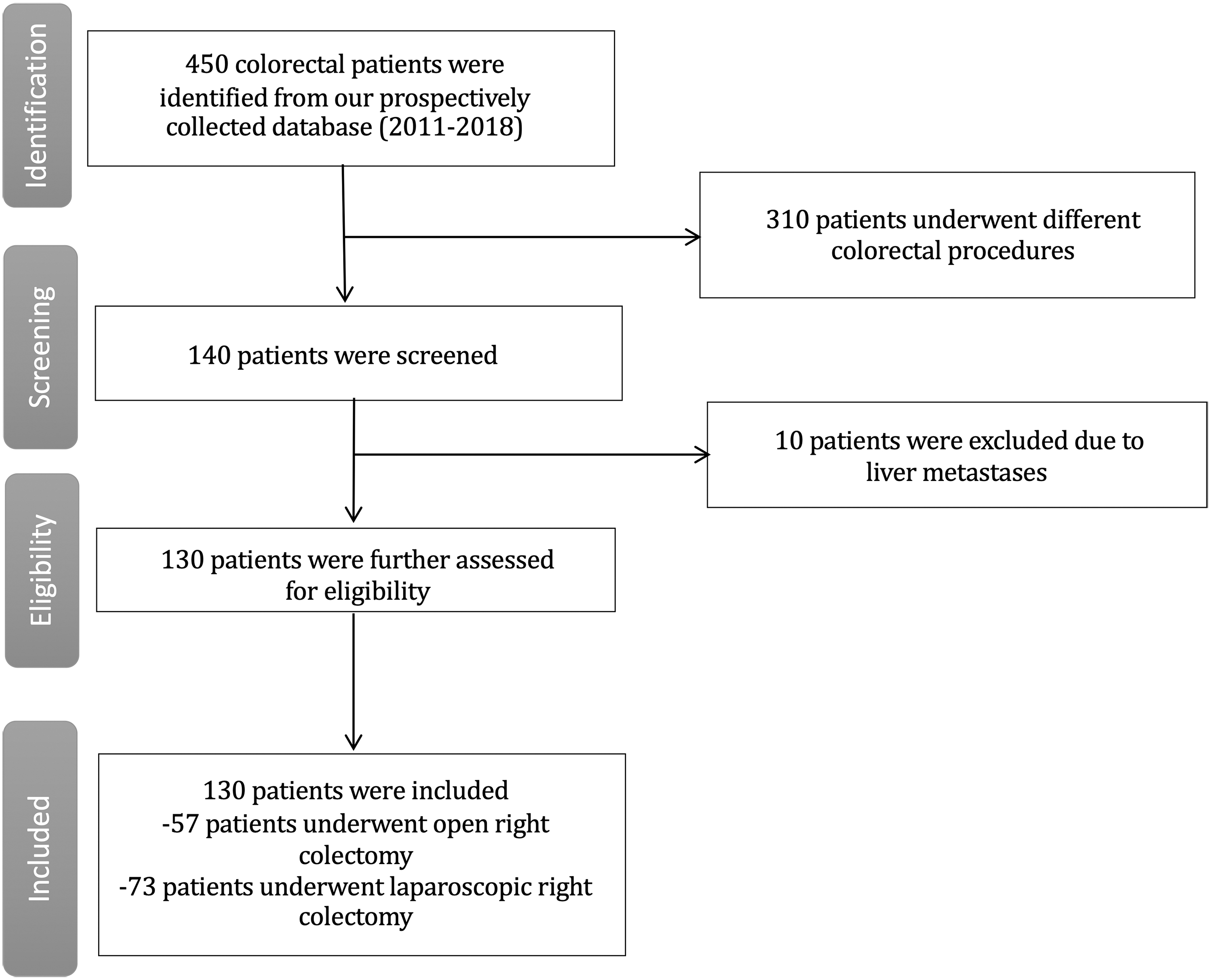
Trial flow of the present study.
Patient Baseline Characteristics
AF, atrial fibrillation; AH, arterial hypertension; ASA, American Society of Anesthesiologists; BMI, body mass index; COPD: chronic obstructive pulmonary disease; DM, diabetes mellitus; SD, standard deviation.
Perioperative outcomes
Perioperative parameters and outcomes are presented in Table 2. The mean operative time (MOT) was 125.1 (standard deviation [SD] = 23.9) minutes for the open group and 180 (SD = 33.4) minutes for the laparoscopic group (P < .01) (Fig. 2). In contrast, the LOS was significantly higher in the open group (P < .01) (Fig. 2). No significant difference was detected regarding the red blood cell transfusions and the number of patients required intensive care unit (ICU) stay. The open group presented a higher rate of surgical site infections (SSIs) (P = .046). No significant difference between the two groups was found regarding each one of the other complications as well as the total complication rate.

Violin plots regarding
Perioperative Parameters and Outcomes
ICU, intensive care unit; LOS, length of stay; MOT, mean operative time; SD, standard deviation; SSI, surgical site infection.
There were no conversions from laparoscopy to open procedure. The mean length of the incision for the extraction of the specimen was 5.420 cm (SD = 1.181). No significant difference was found regarding the reoperation rate. One reoperation (explorative laparotomy) was performed in the open group at postoperative day 13 due to persistent postoperative ileus. Two cases in the laparoscopic group required a reoperation due to anastomotic leaks.
There was no mortality in the open group, while two deaths were noted in the laparoscopic group: In the first case, the patient presented anastomotic leak postoperatively, underwent reoperation, and was transferred to the ICU where the patient developed multi-organ failure and died. The second patient presented massive pulmonary embolism on postoperative day 2.
Pathology outcomes and learning curve
Pathology outcomes are presented in Table 3. No significant difference was detected between the two groups regarding the quality of specimen (mesorectal plane of dissection), rate of R0 resections, number of harvested lymph nodes, number of positive lymph nodes, along with the incidence of vascular and perineural infiltration, tumor size, and length of specimen.
Pathology Outcomes
SD, standard deviation.
The learning curve of the laparoscopic CME-CVL for right-sided CC was also evaluated in the present study and is demonstrated in Figure 3. We found a statistically significant decrease of the operative time (P = .024), which was inversely proportional to the number of consecutive cases. We also calculated the equation which describes the linear correlation between the MOT and the number of consecutive patients: MOT = −0.4131 × (number of consecutive patients) +193.3.
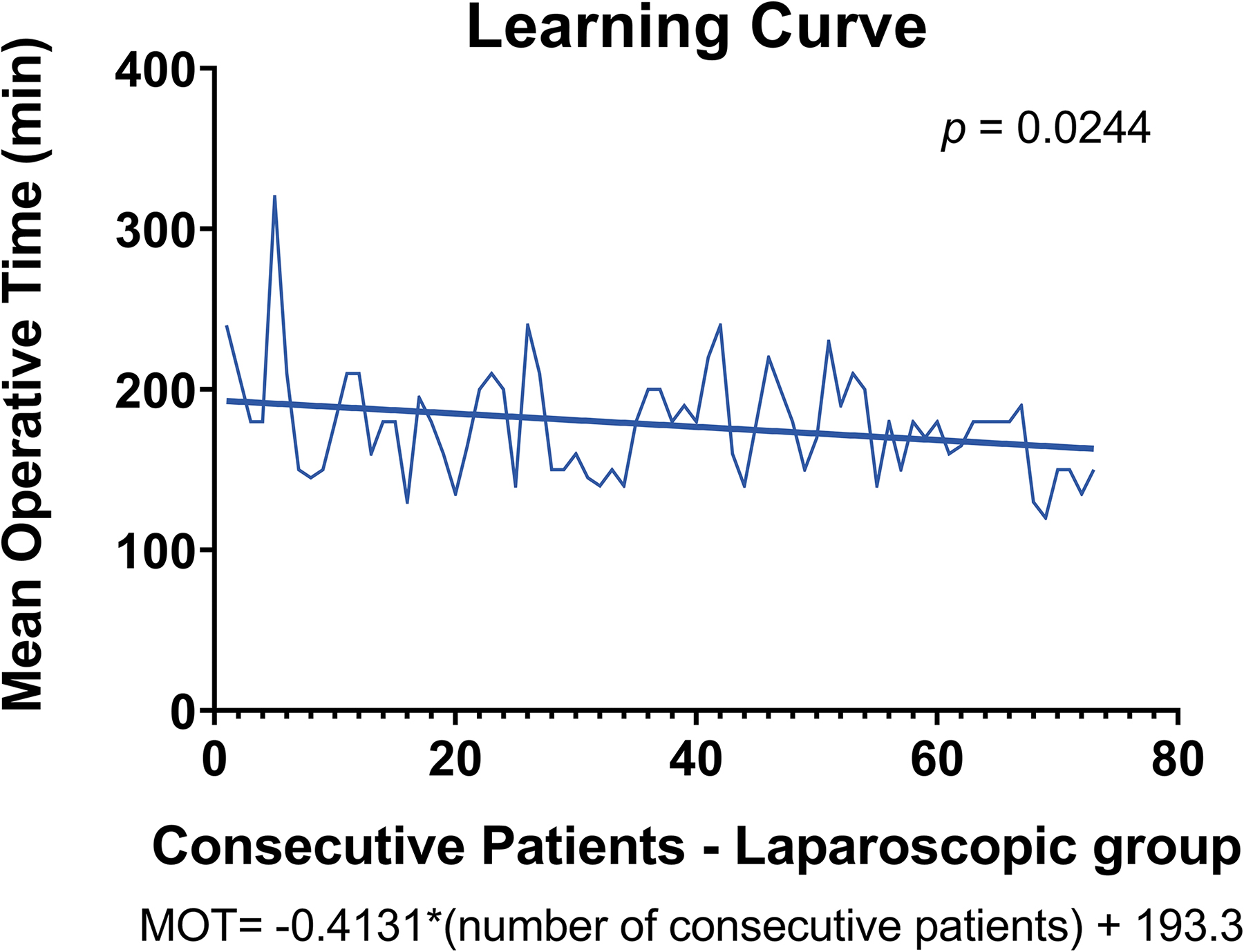
Learning curve regarding the laparoscopic right colectomy group. MOT, mean operative time. Color images are available online.
Discussion
The implementation of the CME-CVL principles in colon surgery remains a highly debatable topic in colorectal surgery, especially for the right CCs.10,11,17 There is clear evidence that colectomies performed according to the CME-CVL principles provide an improvement in the quality of surgical specimen (integrity of the mesocolon, margins, number of harvested lymph nodes), thus offering a potential benefit in long-term oncologic outcomes.18,19 However, this approach is technically more challenging compared to a conventional right colectomy, and this fact is even more exaggerated when it comes to laparoscopy. Most of the trials comparing open with laparoscopic right colectomy were performed during the past decade where the CME concept was not popularized. Our team has adopted the CME-CVL concept regardless of the type of approach and analyzed prospectively collected data from consecutive operations performed either open or laparoscopically, with the view to detect differences in the short-term and pathology outcomes.
In the present study, the laparoscopic group demonstrated a significantly higher operative time, which is attributed to the greater difficulty of the operation, and, consequently, learning curve effect. Nonetheless, we identified the existence of a significant linear reduction of the operative time during the course of the 73 consecutive cases that we included in the present study. Laparoscopic right colectomy was associated with decreased septic complications, as well as hospital stay compared to the open group. Despite the higher technical complexity of the laparoscopic CME-CVL right hemicolectomy, the incidence of reoperations and perioperative mortality were comparable to the open procedure.
The impact of the quality of the specimen—especially the integrity of the mesocolon and the number of harvested lymph nodes—on oncological outcomes is of paramount importance. Certain trials have demonstrated the impact of increased lymph node removal on survival rates for patients with stage II and III CC.20,21 The total number of harvested lymph nodes, along with the ratio of positive lymph nodes have been proposed as prognostic factors in patients with CC, with the optimum number of nodes ranging between 15 and 28.9,22 Within this context, the plane of mesocolic excision plays a pivotal role in the oncologic outcome. In fact, it has been classified into three categories: (i) a muscular plane that is a poor surgical plane, (ii) an intramesocolic plane which is a moderate surgical plane, and (iii) a mesocolic plane which is the surgical plane we should aim to. 23 A mesocolic surgical plane provides a high-quality specimen with no or only minor visceral fascia defects and the primary tumor with its vasculatures and lymphatics is removed intact. There is solid evidence 24 that the mesocolic plane is associated with increased survival in CC surgery. In contrast, a muscular plane produces a poor-quality specimen and probably results in tumor cell spillage or even residual disease. In the present study, a mesocolic plane was achieved in the vast majority of the specimens, and there were no cases of muscular plane. No difference between the type of approach was found regarding the plane of mesocolic dissection. We also demonstrated a comparable rate of R0 resection between the two groups. Furthermore, the number of harvested lymph nodes was within the optimum ranges reported in the literature in both groups, without any difference between open and laparoscopic approach.
A certain limitation of the present study has to do with the design, as it does not represent a prospective randomized trial, thus posing a certain selection bias. Nonetheless, the data are prospectively collected, the patients are consecutive, the surgical team is the same and the surgeon's bias regarding patient/approach selection was minimized, as this was mostly depending on patients' preference and operation room logistics.
The current outcomes demonstrate that the laparoscopic approach offers the same previously reported in “conventional” right colectomy short-term advantages at a cost of an increased operative time over the open right colectomy, even in the era of CME-CVL concept. In addition, it seems that it does not put in danger the oncologic outcome as the pathology characteristics of the specimens are at least as good as in the open approach. However, long-term oncologic outcomes (disease-free survival, 5-year survival etc.) are necessary to confirm the latter, and this represents our next step of analysis of the present series.
Conclusion
In this study, we compared the open and laparoscopic CME-CVL right hemicolectomy. The laparoscopic approach is superior compared to the open approach in terms of LOS and SSI rate. Both approaches provided similar pathology outcomes. Despite the increased operative time in laparoscopy group, this is gradually reduced following the learning curve that we demonstrated. Future studies should further evaluate their long-term oncologic outcomes.
Footnotes
Authors' Contributions
D.E.M. and G.A.T. contributed to conception and design, acquisition of data, analysis and interpretation of data, drafting the article or revising it critically for important intellectual content, and final approval of the version to be published. I.B. contributed to conception and design, acquisition of data, interpretation of data, revising the article critically for important intellectual content, and final approval of the version to be published. I.M. and C.P. contributed to acquisition of data, interpretation of data, revising the article critically for important intellectual content, and final approval of the version to be published. E.B. contributed to acquisition of data, drafting the article, and final approval of the version to be published.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.