
Abstract
Background and Objectives:
There are two operative approaches for adenocarcinomas of the esophagogastric junction: thoracoabdominal esophagectomy or transhiatal extended gastrectomy. Both procedures can be performed minimally invasively. Dependent on the exact localization of the tumor, both approaches are feasible. Aim of this study was to compare the health-related quality of life (HRQOL) of patients after minimally invasive esophagectomy (MIE) with patients who underwent minimally invasive gastrectomy (MIG).
Methods:
All patients who underwent MIE or gastrectomy for malignoma since 2014 were identified from our clinical database. The identified patients were contacted and asked to fill out a quality of life questionnaire (QLQ) for general and gastrointestinal QOL (European Organization for Research and Treatment of Cancer QLQ-C30 and QLQ-OG25).
Results:
Global HRQOL scores were higher in patients after MIE than after MIG. After MIE, global HRQOL scores were close to the control population. In cancer-specific syndromes, patients after MIE reported lower symptom scores for financial problems, eating, reflux, and eating with others than patients after MIG.
Conclusion:
In terms of HRQOL, MIE proved superior to MIG in long-term follow-up in this study. Patients after MIE reported a HRQOL close to that of a healthy reference population.
Introduction
The incidence of adenocarcinomas of the esophagogastric junction (AEG tumors) is rising steadily. 1 AEG tumors can be divided in types I–III depending on the tumor site, type I marking the tumors of the distal esophagus, type II marking the “true” carcinoma of the esophagogastric junction, and type III being subcardial gastric carcinomas infiltrating the esophagogastric junction. 2 While thoracoabdominal esophagectomy (TAE) with gastric tube reconstruction is usually performed in AEG I tumors, transhiatal extended gastrectomy (TEG) with Roux-en-Y reconstruction is mainly performed in AEG III tumors. However, in AEG II tumors, both procedures appear to be feasible due to their location between the esophagus and stomach.2–8 Aim of both operation techniques is R0 resection. Perioperative mortality is usually below 10% in experienced centers, but can go up as far as 23% in low-volume centers.3,5,6,9,10 In terms of oncological benefits, TAE has been described to offer the advantage of a more complete lymphadenectomy. 5 Overall survival has been described similar, while some studies suggest a survival benefit after TAE when compared to TEG.3,5 Recently, operation technique evolved from open procedure to minimally invasive approach, resulting in equal to lower mortality rates and a shorter hospital stay.7,11 There have been few studies addressing the question of health-related quality of life (HRQOL) after TAE and TEG.8,12–16 Even if minimally invasive esophagectomy (MIE) and minimally invasive gastrectomy (MIG) are comparable in terms of R0 resection and perioperative mortality, HRQOL in survivors should also be taken into account when selecting the adequate operation technique. The aim of this study was to compare the long-term HRQOL after MIE and MIG.
Materials and Methods
Study design
Patients who underwent MIE and MIG between March 2014 and November 2018 were identified from our clinical database. Informed consent was obtained from all patients and procedures were in accordance with the Declaration of Helsinki 1975, as revised in 1983. This study was approved by our Ethics Committee (EK175/19). Patients who underwent operation due to other criteria but malignoma were excluded. Other exclusion criteria were diagnosis of a second tumor and tumor recurrence. Choice of the surgical approach had been made based on the exact site of the tumor and patients' individual cofactors. Patients were contacted from May 2019 to November 2019 and then asked to fill out the health-related quality of life survey published by the European Organization for Research and Treatment of Cancer (EORTC surveys quality of life questionnaire [QLQ]-C30 and QLQ-OG25).17,18 A minimum of 6 months was ensured between operation and follow-up. QLQ-C30 includes 30 general questions about HRQOL and cancer-specific syndromes (CSS), while QLQ-OG25 includes 25 questions regarding gastrointestinal CSS. Data were transformed into scores ranging from 0 to 100 according to the EORTC manual. 19 The surveys were done in German language. Data were compared to general population normative data for Germany in general symptoms 20 and to reference values obtained in a healthy Swedish population for esophagogastric symptoms. 21
Operation procedures
Minimally invasive esophagectomy
The laparoscopic part was operated in reverse Trendelenburg position. After establishing a pneumoperitoneum with a minilaparotomy, five 5–10 mm ports were placed. Then the gastrocolic and gastrosplenic ligament were dissected using an ultrasonic scissor preserving the right gastroepiploic arcade. After dissection of the omentum minus, the abdominal part of the esophagus and the hiatus were mobilized. The left gastric artery and vein were divided and standard lymphadenectomy was performed. A 3–4 cm wide gastric conduit was constructed by using an endoscopic linear stapler (Endo-GIA, 60 mm; Medtronic) starting at crow's foot at the lesser curvature. The patient was then turned to the left side and the right lung was excluded from ventilation, and five 10.5–11.5 mm trocars were inserted. The arch of the azygos vein was divided using an Endo-GIA stapler, and mediastinal pleura was incised. The esophagus was completely mobilized and en-bloc lymphadenectomy was carried out. After removal of the specimen an end-to-side esophagogastric anastomosis was performed (EEA circular stapler, 28 mm; Medtronic). Finally, the excess stomach was transected with a linear stapler.
Minimally invasive gastrectomy
After positioning of the patients in reverse Trendelenburg position, pneumoperitoneum was established via minilaparotomy. Five ports were placed in the upper abdomen. First, the greater omentum was dissected from the transverse colon and the stomach was lifted. Then the omentum minus was dissected and the abdominal part of the esophagus mobilized from the hiatus. The right gastroepiploic vessels were clipped and the stomach was resected 2 cm distal to the pylorus using a linear stapler (Endo-GIA, 45 mm; Medtronic). The left gastric artery and vein were divided and a standard D2-lymphadenectomy was performed. Then the abdominal part of the esophagus was divided (Endo-GIA, 45 mm; Medtronic). The stomach was extracted through a widened port incision. For restoring of intestinal continuity, an antecolic Roux-en-Y esophagojejunostomy was performed. End-to-side esophagojejunal anastomosis was created with a circular stapler (EEA circular stapler, 25 mm; Medtronic). Finally, the side-to-side jejunojejunostomy was performed 30–40 cm distal to the esophagojejunostomy using a linear stapler (Endo-GIA, 45 mm; Medtronic).
Statistical analysis
Data were compared according to Global health scores, CSS and gastrointestinal CSS by two-way analysis of variance. To assess statistical effects of single items, Tukey's multiple comparisons test was used. For statistical analysis, Microsoft Excel and GraphPad Prism version 7.04 were used.
Results
A follow-up was possible for 48 patients. Most patients included in this study were male (75%). Mean age was 63 years (standard deviation [SD] 7.6) and mean time to follow-up was 790 days (SD 492). There was no difference between groups either for age (P = .07) or for time to follow-up (P = .95). Neoadjuvant therapy had been administered in 33 cases (69%). Histological examination revealed adenocarcinoma in 84% after MIE and 96% after MIG. Sixteen percent of patients (n = 4) after MIE had a squamous cell carcinoma and one patient after MIG had a neuroendocrine carcinoma. For further information on the study population see Table 1.
Information on Study Population
AEG, adenocarcinomas of the esophagogastric junction; CTx, chemotherapy; MIE, minimally invasive esophagectomy; MIG, minimally invasive gastrectomy; RTx, radio-chemotherapy; SD, standard deviation.
In general, patients after MIE scored higher in QOL than patients after MIG. Indicated scores after MIE were higher for role function (80.7 versus 57.3, P < .01) and social function (93 versus 76, P < .05) than in patients after MIG.
When comparing to the normative data for Germany, patients after MIE scored higher than the control population for emotional function (89 versus 74, P < .01), and there was a significantly lower score in role function after MIG (57 versus 84, P < .001) (Fig. 1). For the other items, there was no statistical difference between the operation types and the normative population. For further information concerning the Global Health Scale see Table 2.

Global quality of life. MIE, minimally invasive esophagectomy; MIG, minimally invasive gastrectomy; Norm_GER, normal values for German reference population.
Global Health Scale
ns, not significant.
Concerning CSS, patients after MIE indicated lower symptom scores for problems with finances (8 versus 31.9, P < .01). Scores for fatigue, nausea, appetite, diarrhea, insomnia, and pain symptoms were similar after MIE compared with MIG. Patients after MIE reported lower scores for pain than the control population (12 versus 27.6, P < .01) (Fig. 2).
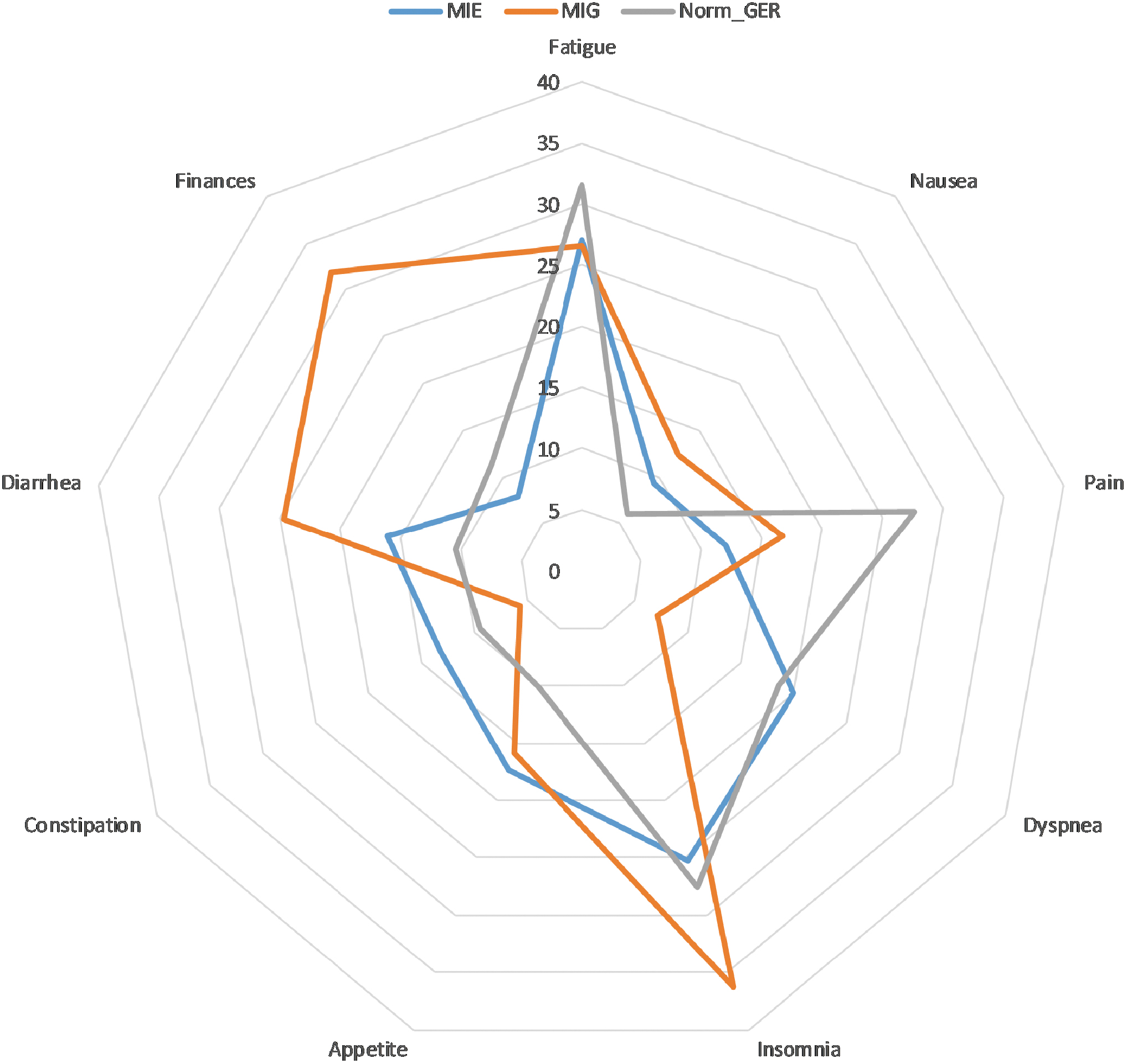
Cancer-specific symptoms. MIE, minimally invasive esophagectomy; MIG, minimally invasive gastrectomy; Norm_GER, normal values for German reference population.
In esophagogastric CSS, patients after MIE reported lower scores than patients after MIG in problems with eating (13 versus 25.3, P < .01), reflux (14 versus 25, P < .05), and eating with others (4 versus 15.2, P < .05). All general CSS and gastrointestinal specific CSS for both types of operation are listed in Tables 3 and 4. In comparison to the Swedish normal cohort, both groups reported higher scores in problems with eating (13 and 25.3 versus 2.9, P < .001 and P < .0001 respectively), reflux (14 and 25 versus 6.7 P < .05 and P < .0001 respectively), and problems with weight loss (18 and 25 versus 1.8, P < .0001 and P < .0001 respectively), while scores in odynophagia and dysphagia were only higher in patients after MIG (14.7 versus 1.5 and 11.6 versus 0.8, P < .0001 and P < .001, respectively) (Fig. 3).
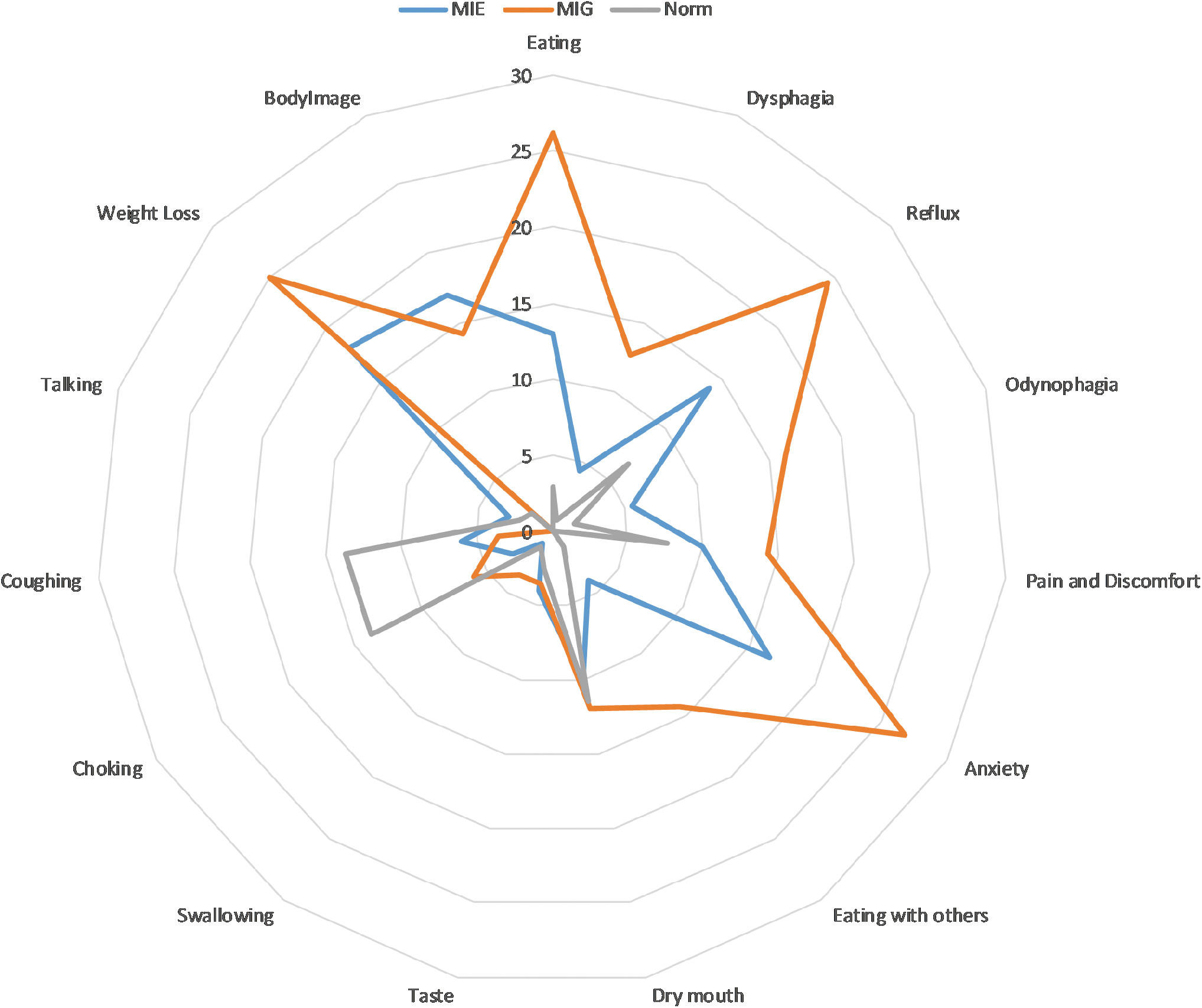
Gastrointestinal cancer-specific symptoms. MIE, minimally invasive esophagectomy; MIG, minimally invasive gastrectomy.
Cancer-Specific Symptom Scale
Gastrointestinal Cancer-Specific Symptom Scale
na, not available.
Discussion
Despite the rising incidence of tumors of the esophagogastric junction, the selection of the appropriate operation technique is subject to current research. 3 While transthoracic esophagectomy (TAE) and TEG appear to be equivalent in terms of R0 resection, morbidity, and mortality, the question of the postoperative QOL has rarely been addressed.2–8,16,22 Aim of this study was to compare the QOL in patients after TAE and TEG were performed minimally invasively (MIE versus MIG). Postoperative QOL was excellent in patients who underwent MIE in this study of long-term QOL. In terms of short-term QOL (6 months after operation), a similar QOL after TAE and TEG has been reported before.22,23 However, a recent study comparing the two approaches TEG and TAE by Fuchs et al. 12 reported a superior QOL after TEG, compared with TAE, mainly due to fewer pulmonary and reflux-related symptoms. Nevertheless, in that study, patients underwent the classical, open approach in 30% and hybrid approach with laparoscopy and thoracotomy in 70%. 12 Another study that included patients after minimally invasive approach found a comparable QOL after >1 year between both operation techniques with the exception of the symptoms “coughing” and “choking when swallowing,” which were more frequently observed after MIE. 16 In this study, we could not confirm a higher prevalence of pulmonary symptoms such as coughing and dyspnea after MIE. Time point of follow-up might be crucial, as other studies also suggest a restored QOL 6–12 months after surgery.22,23 In similar manner, another study by Johansson et al. 8 also reported global health scores similar to the normal population in their long-term follow-up of patients after TEG and TAE. However, a comparison between the surgical procedures was not possible due to the small number of included patients. 8
In our study, patients after MIE had significantly higher scores in role function and social function when compared to patients after MIG (80.7 versus 57.3, P value <.01 and 93 versus 76, P value <.05, respectively). Furthermore, in emotional function, patients after MIE even scored higher than the general population in Germany (89 versus 74, P value <.01). In line with our results, Headrick et al. also found better higher emotional and physical performance in patients after esophagectomy for high-grade dysplasia than in healthy controls. 15 There are several possible reasons for this. One study by Arndt et al. found a comparable QOL in cancer survivors when compared to healthy controls. 24 However, an inferior QOL was noted in younger patients (<50 years). In this study, the mean age of patients was higher (63 years, SD 7.6), possibly explaining a higher emotional stability. Another possible explanation might be the linkage of depression in cancer survivors to household income. 25 Likewise, patients after MIE rarely suffered from financial problems in this study (CSS 8 versus 11.3 in German reference population). On the contrary, patients after MIG reported lower scores in role function and higher scores for financial problems when compared to the German reference population (57.2 versus 65 P value <.0001, 31.9 versus 11.3, P value <.001, respectively).
In line with these results, gastrointestinal symptoms such as problems with eating, reflux, and eating with others were more common in patients after MIG than after MIE. In comparison to the control population, there was an impairment in symptoms such as dysphagia and odynophagia after MIG, but not after MIE. In the recent study by Jezerskyte et al., CSS for eating and odynophagia were also higher in patients after gastrectomy, but did not reach statistical significance due to a low chosen P value. 16 Nevertheless, taking in mind the high clinical importance of CSS such as financial problems, eating, reflux, and eating with others, we could find significant advantages of MIE in comparison to MIG in this study.
There are several limitations to this study. First, we describe the compared QOL after the different surgical procedures MIE and MIG and not solely after resection of AEG II tumors. Furthermore, we in this study, present a retrospective evaluation of a prospectively kept database. Finally, due to the lack of reliable data on CSS of the upper gastrointestinal for Germany, we had to compare our findings to reference data from a Swedish population. As HRQOL scores of the healthy population have been reported to differ significantly between European states, 20 baseline CSS data for Germany might actually be lower than the values used in this study. Furthermore, no conclusions of oncologic outcome can be drawn.
Nevertheless, taking in mind the scarcity of reliable data on the HRQOL after esophagectomy and gastrectomy, we hereby approve the superiority of MIE over MIG in terms of long-term HRQOL. These findings support the application of MIE in patients with AEG type II tumors and should be confirmed by randomized controlled trials.
Conclusion
This is the first study to compare the QOL after MIE and MIG. MIE proved to be superior to MIG in terms of role function and emotional function. For CSS, we could also see an advantage in MIE in terms of problems with finances, eating, reflux, and eating with others. There was no general significant difference in QOL in our patients in comparison to normative data of a healthy population in MIE with the exception of emotional function, where patients after MIE scored better than the normative population. In contrast, patients after MIG scored worse in comparison with the normative population in role function and showed more CSS than a healthy control population in diarrhea, finances, eating, dysphagia, odynophagia, and eating with others. In terms of long-term QOL, MIE could therefore be favored over MIG.
Ethical Approval and Consent to Participate
Informed consent was obtained from all patients and procedures were done in accordance with the Declaration of Helsinki 1975, as revised in 1983. This study was approved by our Ethics Committee (EK175/19).
Consent for Publication
All authors provide consent for publication of this work.
Availability of Supporting Data
The authors declare that they have full control of all primary data and agree to allow the journal to review their data if requested.
Footnotes
Authors' Contributions
S.M.S. together with C.D.K. designed the study. S.M.S. wrote the article. L.S., A.K., and A.A.R. obtained data. S.M.S., P.H.A., R.M.E., A.K., and A.A.R. analyzed the data. U.P.N. supervised the project. All authors discussed the results and revised the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.