
Abstract
Background:
Noninferiority of the laparoscopic approach compared with open surgery for colon cancer treatment has remained controversial. In this study, we aimed to evaluate the long-term outcomes of laparoscopic surgery (LS) versus open surgery (OPS).
Methods:
A total of 418 patients with Stage I–III colon cancer, who received radical surgery at the Tokyo Medical University Hospital from 2000 to 2014 were included. Propensity score analysis with overall survival (OS) and relapse-free survival (RFS) as the primary endpoints was performed retrospectively to reduce the effects of confounding factors between groups, including age, sex, body mass index, tumor size, clinical T stage, and clinical N stage.
Results:
After case matching, the 5-year OS rate was 87.8% in the OPS group (n = 97) and 90.1% in the LS group (n = 97; P = .59), indicating no significant difference. The 5-year RFS rate was 79.0% in the OPS group (n = 97) and 84.1% in the LS group (n = 97; P = .29), indicating no significant difference. Five-year cumulative local recurrence (LR) rates were 7.6% and 0% in the OPS group and the LS group, respectively, indicating a significant difference (P = .007). Five-year cumulative distant metastasis rates were 9.2% and 12.7% in the OPS group and the LS group, respectively (P = .49).
Conclusion:
Laparoscopic surgery appears to be a reasonable option with similar long-term outcomes and to have low LR rate to open surgery in colon cancer patients.
Introduction
Laparoscopic surgery (LS) has been performed in an increasing number of patients as a surgical option for the treatment of colon cancer. Noninferiority of the laparoscopic approach compared with open surgery (OPS) for colon cancer treatment has not been clearly established. There are many randomized-controlled trials in the world that was analyzed short-term and long-term benefits of LS compared with OPS.1–5 However, these trials had a high proportion of patients with pathological Stage 0–I cancers and included rectal cancer in some studies. Although long-term survival outcomes were almost identical between laparoscopic and open surgeries, the results of the JCOG0404 study in Japan showed that noninferiority of the laparoscopic surgery could not be established in terms of overall survival (OS) with Stage II–III colon cancer patients. 6 The interpretation of this study was that laparoscopic surgery was the acceptable optional treatment. However, there are some reports that there are institutional disparities to the selection of surgical procedure.7,8 As a fact, the reason for the good prognosis in the JCOG0404 study was considered that many leading hospitals in colon cancer participated in this study. 6 Thus, it is important to evaluate the long-term oncologic outcomes in each institute to validate these results. To minimize selection bias as limitations of retrospective study and to increase the strength of the evidence, some researchers use a propensity score analysis. The aim of this study was to compare long-term survival outcomes of laparoscopic surgery versus open surgery for Stage II–III colon cancer at our institute using the propensity score analysis.
Materials and Methods
Patients
In total, 418 patients who underwent radical surgery for Stage II–III colon cancer between 2000 and 2014 at the Tokyo Medical University Hospital were reviewed retrospectively. Then, we divided 402 patients into two groups by surgical procedure, the OPS group and the LS group. We defined the colon as cecum to rectosigmoid colon. The study was reviewed and approved by the Institutional Review Board of Tokyo Medical University Hospital.
Surgical treatment
All patients underwent gross curative operations. Specimens were all opened up along the antimesenteric border by surgeons, and all harvested lymph nodes from the mesocolon. The specimens were then laid out on a board and were fixed in 10% formalin.
Postoperative systemic adjuvant chemotherapy
Postoperative systemic adjuvant chemotherapy is generally performed for pStage III colon cancer in our institute. In this study, adjuvant chemotherapy was performed for 19 of 216 patients (8.7%) in pStage II and 86 of 202 (42.6%) patients in pStage III.
Follow-up
The median follow-up period was 73.1 months (range, 0.2–225.2 months). The follow-up strategy was as follows. Patients who had Stage II or III tumors were examined for up to 5 years postoperatively for every 3 months for the first 2 years (tumor marker measurement only), and every 6 months (tumor marker measurement and computed tomography [CT] scans) for the next 3 years. When the first recurrence occurred, the recurrence site and date were recorded. Local recurrence (LR) was defined as any histological or clinical evidence of tumor regrowth near the primary site. The sites of LR were divided into four groups on the basis of established criteria: perianastomotic colon, mesenteric and paracolic lymph nodes, peritoneum (including serosal and omental implants), and retroperitoneum.9,10 Tumor recurrence at nonregional sites, such as the liver or lung, was recorded as distant metastasis (DM). LR was recorded regardless of the presence of metastatic disease.
Statistical analyses
The primary outcome was 5-year OS and 5-year relapse-free survival (RFS). OS was defined as the interval between the date of operation and the date of either death or the end of the observation period. Patients alive at the end of follow-up were censored. RFS was defined as the interval from the date of operation to date of recurrence, or death from underlying disease. Observations were censored when patients died as a result of noncolorectal cancer. Survival characteristics were described using the Kaplan–Meier method and were compared using the log-rank test. Propensity score analyses were performed to adjust for heterogeneity between the two groups by surgical procedure. Multivariate logistic regression was used to generate a propensity score predicting condition by surgical procedure (LS versus OPS). The following six covariates were included: age, sex, body mass index (BMI), tumor size, pathological T-stage, and pathological lymph node metastasis. Then, each patient was assigned an estimated propensity score, which represented the patient's predicted probability of the surgical procedure status. Propensity score matching was performed in which patients were paired by similarities in their characteristics. Each patient who had laparoscopic surgery was matched to a patient who had open surgery and had the closed propensity score on the logit scale with a caliper of 0.05. We also evaluated laparoscopic versus open surgery oncologic outcomes in terms of recurrence pattern, LR versus DM, and location of the tumor, left-side versus right-side colon. All statistical analyses were performed using SPSS version 25 (IBM® SPSS® Statistics 25.0 Windows® client version, IBM, Chicago, IL) software for Windows. The level for statistical significance was determined to be P < .05.
Results
Surgical procedure
There were 302 patients in the OPS group and 116 patients in LS group. There were both 97 patients in each group among matched groups.
Patient and tumor characteristics
The characteristics of patients in the two treatment groups are shown in Table 1. Patients in the OPS group were more likely to have deep (P = .007) and large (P = .002) advanced cancers before case matching. No significant differences were observed in other covariates. After case matching, clinical outcomes were similar between the LS group and the OPS group. The matched analysis was performed according to surgical procedure to adjust for heterogeneity in the OPS group and the LS group, with six covariates: age, sex, BMI, tumor size, pathological T-stage, and pathological lymph node metastasis. The distributions of propensity scores before and after case matching are shown in Figure 1A and B. The OPS group and LS group (97 matched pairs) showed a well-matched distribution with respect to patient and tumor characteristics in the adjusted analysis after case matching (Table 1). There was no significant difference between two groups, including tumor size and pathological T-stage.
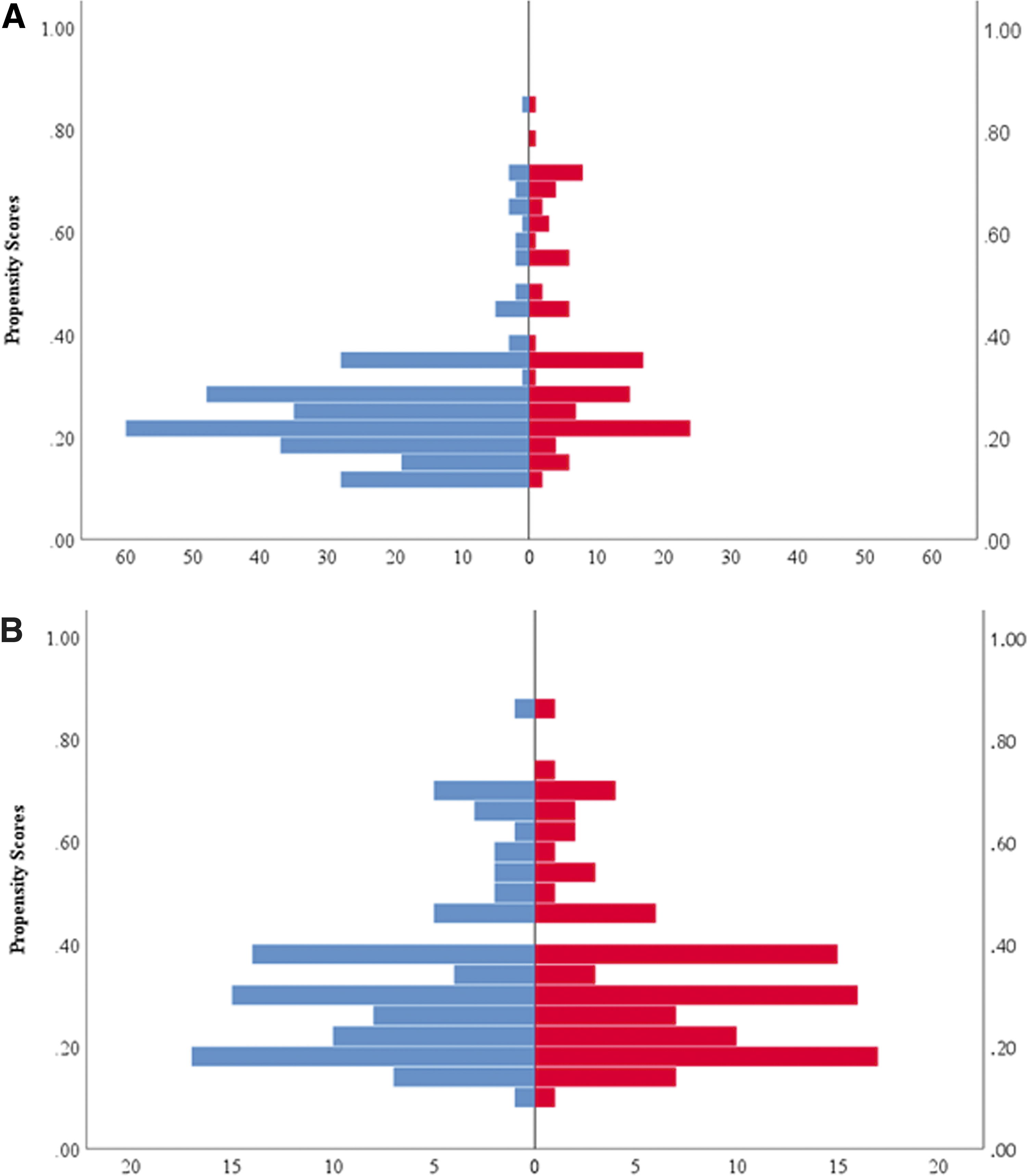
The distributions of propensity scores before and after case matching.
The Characteristics of Patients in the Two Treatment Groups
Data are expressed as median (range) or n (%).
Statistically significant at P < .05.
BMI, body mass index; LS, laparoscopic surgery; OPS, open surgery.
Pathological outcomes
Table 2 shows other pathological outcomes. There was no significant difference between the OPS group and the LS group both before case matching and after case matching.
Pathological Outcomes of Patients in the Two Treatment Groups
Data are expressed as median (range) or n (%).
Statistically significant at P < .05.
LS, laparoscopic surgery; OPS, open surgery.
OS and RFS
The 5-year OS rate was 89.9% and the 5-year RFS was 81.5% in the entire cohort. Before case matching for all stages, the 5-year OS rate was 89.8% in the OPS group (n = 302) and 89.8% in the LS group (n = 116; P = .58), indicating no significant difference (Fig. 2A). The 5-year RFS rate was 79.9% in the OPS group (n = 302) and 84.9% in the LS group (n = 116; P = .42), indicating no significant difference before case matching for all stages (Fig. 2B).
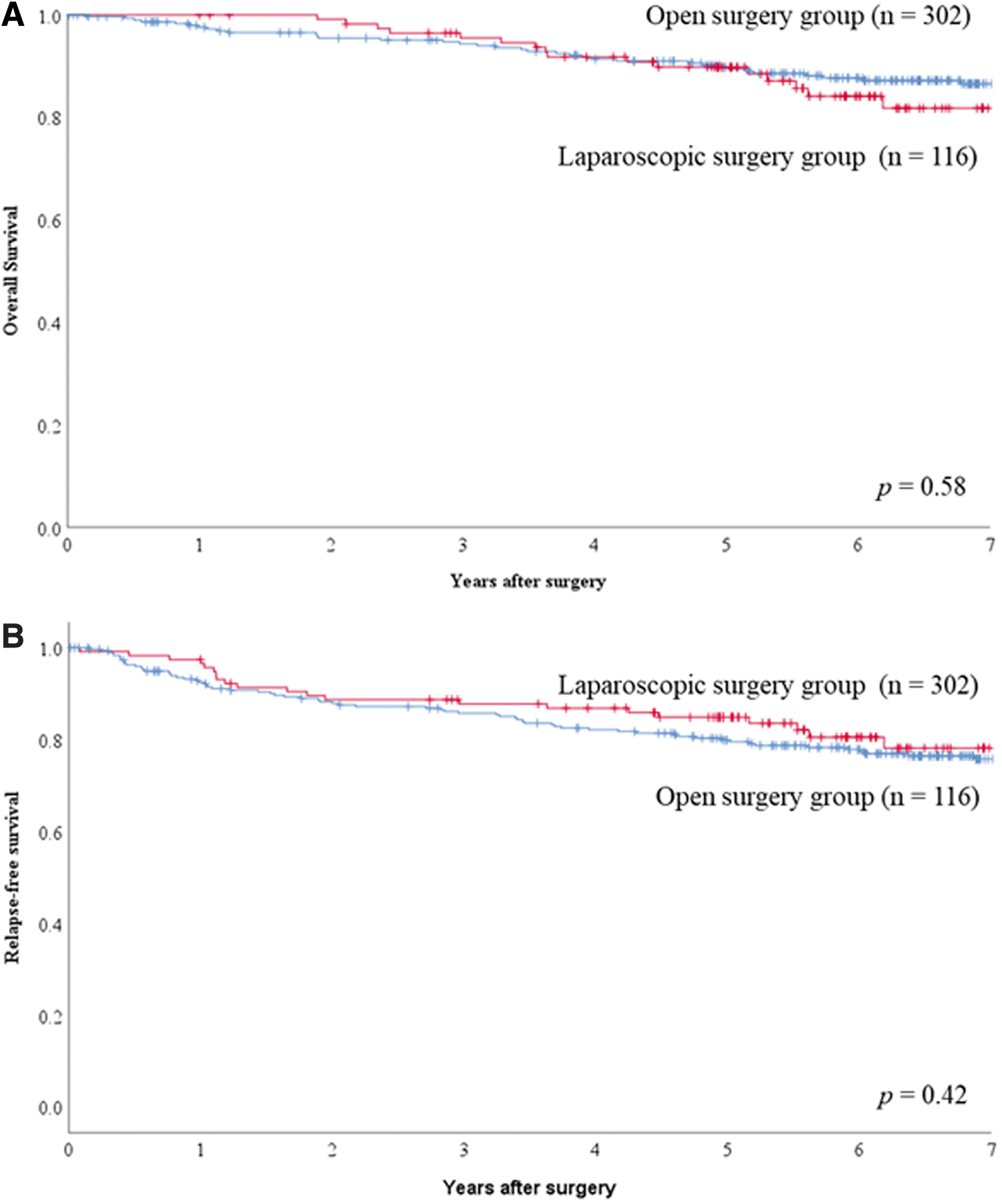
OS rates and RFS rates in the entire cohort based on surgical procedure.
We analyzed survival data for patients after case matching. After case matching, the 5-year OS rate was 87.8% in the OPS group (n = 97) and 90.1% in the LS group (n = 97; P = .59), indicating no significant difference (Fig. 3A). The 5-year RFS rate was 79.0% in the OPS group (n = 97) and 84.1% in the LS group (n = 97; P = .29), indicating no significant difference after case matching (Fig. 3B).

OS rates and RFS rates in the propensity score-matched population based on surgical procedure.
Overall patterns of recurrence
In the entire cohort, recurrence was observed in 65 patients (15.5%); 54 (12.9%) had DM and 11 (2.6%) had LR. In the matched cohort, 5 patients (26%) had LR and 28 (14.4%) patients had DM. Site of LR in the entire cohort and matched cohort are shown in Table 3. In the entire cohort, 5-year cumulative LR rates were 5.6% and 0% in the OPS group and the LS group, respectively, indicating significant difference (P = .02) (Fig. 4A). Five-year cumulative DM rates were 11.9% and 12.2% in the OPS group and the LS group, respectively (P = .99) (Fig. 4B). In the matched group, 5-year cumulative LR rates were 7.6% and 0% in the OPS group and the LS group, respectively, indicating a significant difference (P = .007) (Fig. 5A). Five-year cumulative DM rates were 9.2% and 12.7% in the OPS group and the LS group, respectively (P = .49) (Fig. 5B).
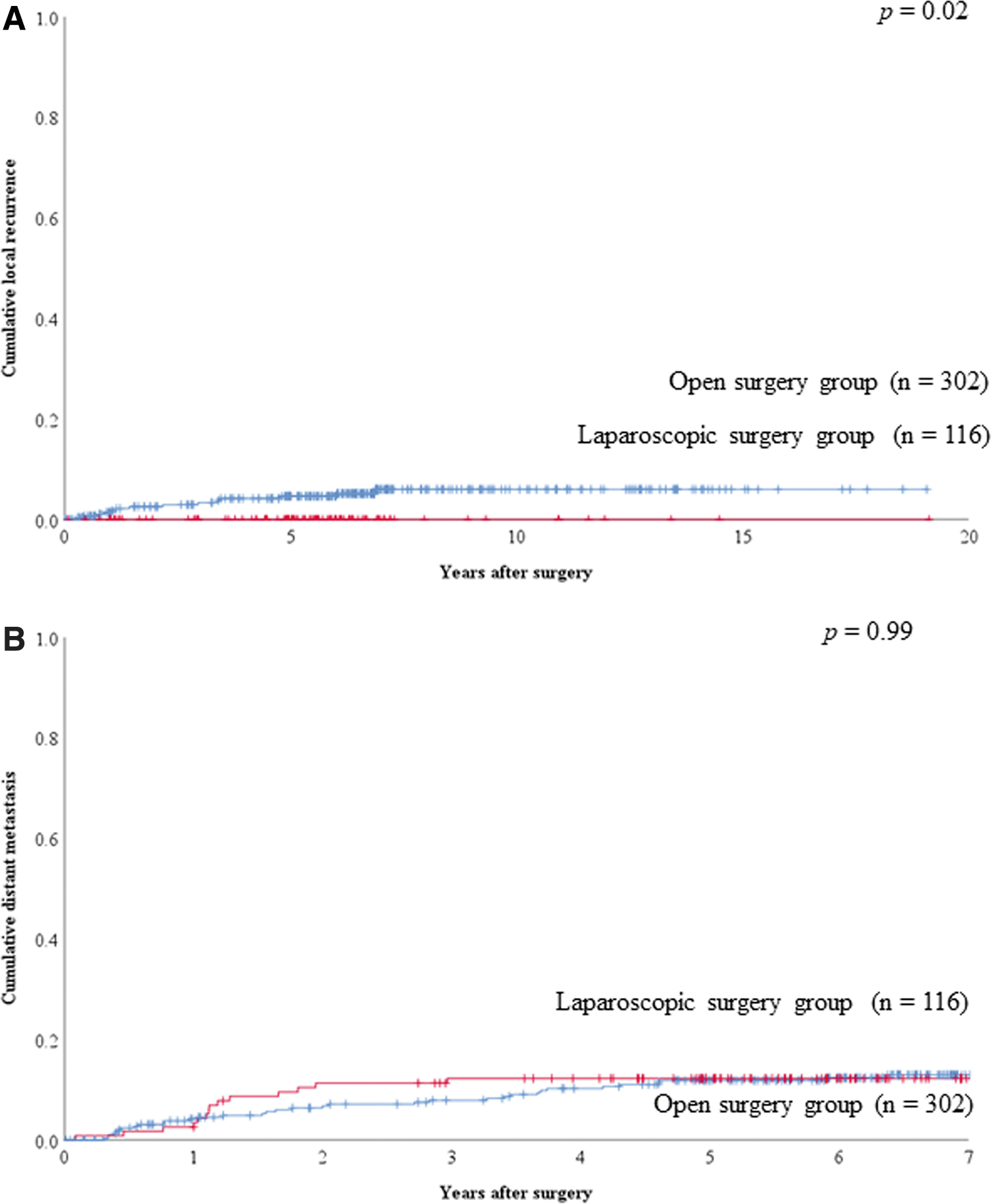
Cumulative LR and distant metastasis rates in the entire cohort based on surgical procedure.
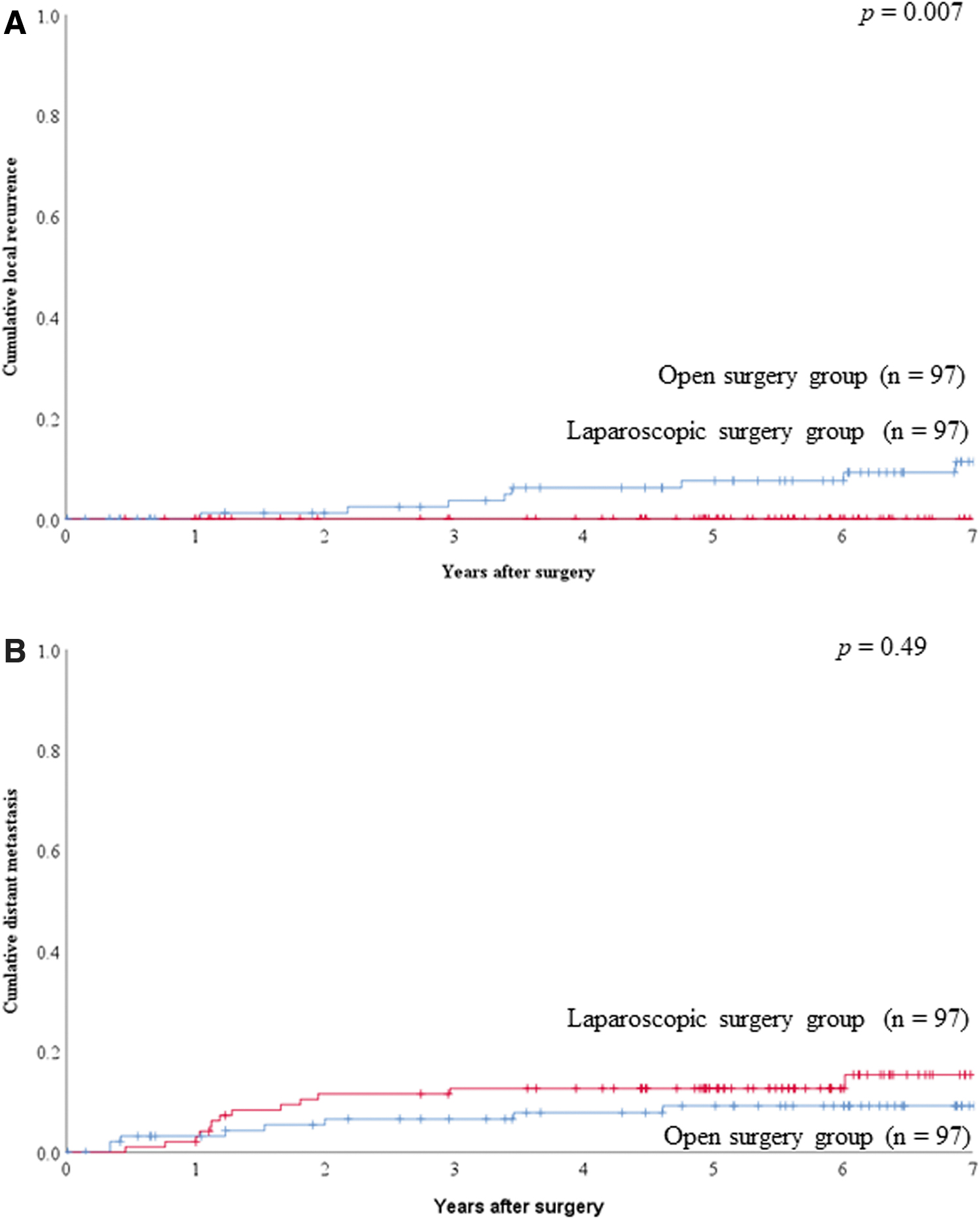
Cumulative LR and distant metastasis rates in the propensity score-matched population based on surgical procedure.
The Sites of Local Recurrence in the Entire Cohort and the Matched Group
Data are expressed as n (%).
Tumor sidedness
To evaluate the prognostic value of laparoscopic surgery versus open surgery by tumor sidedness, patients were divided into two groups according to tumor location in the colon (right-side colon: from cecum to transverse colon; left-side colon: from splenic flexure to rectosigmoid colon). Survival data were analyzed for case-matched patients. Among patients with right-sided colon cancer, 5-year OS and 5-year RFS rates were 85.0% and 75.4% in the OPS group (n = 44), respectively, and 87.9% and 87.9% in the LS group (n = 34), respectively, showing no significant difference (P = .62 and P = .21, respectively) (Fig. 6A, C). Among patients with left-sided colon cancer, 5-year OS and 5-year RFS rates were 90.0% and 81.9% in the OPS group (n = 53), respectively, and 91.4% and 82.0% in the LS group (n = 63), respectively, showing no significant difference (P = .96 and P = .77, respectively) (Figs. 6B, D).
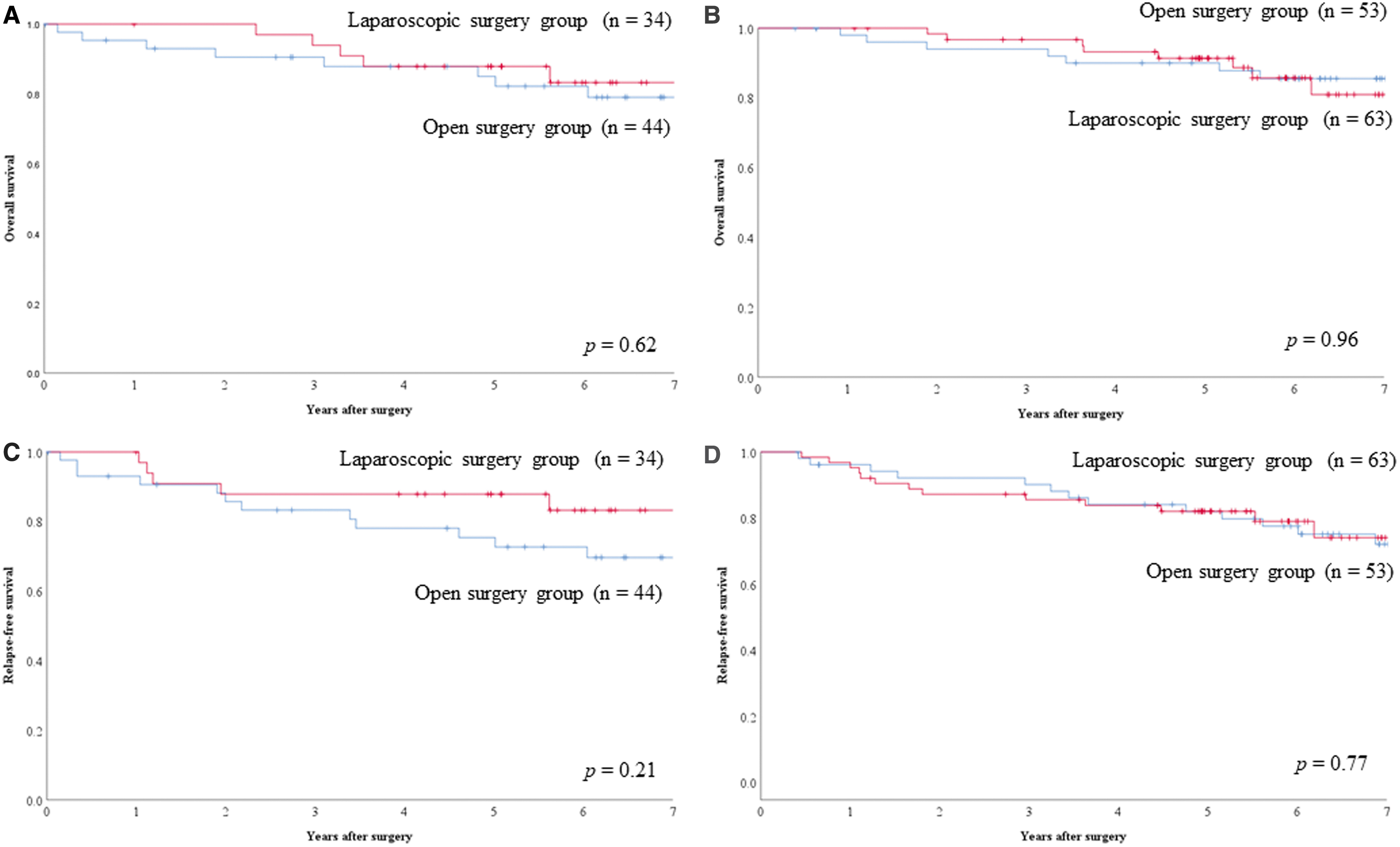
Survival rates in the propensity score-matched population based on tumor location.
Discussion
Colorectal cancer is the second cause of cancer death in Japan. Surgical resection of colorectal cancer remains the only curative modality. The laparoscopic approach is now increasingly being used for colorectal cancer. Evidence from randomized clinical trials has consistently shown comparable outcomes between open and laparoscopically assisted surgery in terms of safety, OS, and DFS.3,6,11 In contrast, there are some reports that there are institutional disparities to the surgical procedure and to the oncologic outcomes in laparoscopic colectomy.6–8 Our institute is defined as a university hospital, not a cancer-specific hospital and also not a regional general hospital. It is valuable to evaluate and to report the survival outcomes for open surgery versus laparoscopic surgery in our institute or a similar role institute to continue laparoscopic surgery in the future.
Propensity score analyses were used to adjust for covariates before circulation of the treatment effect (matching analysis). 12 Our results of OS and RFS for Stage II–III colon cancer were better than or as good as other previous reports in both open and laparoscopic surgery.1,2,4,6,13 Although our institute is a university hospital, LR and distant metastasis rate were also as good as other previous reports in both open and laparoscopic surgery.2,4,13 As the same with other previous reports, there were no significant differences for OS and RFS between open and laparoscopic surgery in our institute. Although many other previous reports showed no significant difference for local and distant metastasis rate between open and laparoscopic surgery,2,13 our results showed significant difference for cumulative(Cum.) LR between open and laparoscopic surgery. The OPS group showed worse LR rate than the LS group both before and after case matching. There were no patients who had LR in the LS group.
Both the National Comprehensive Cancer Network (NCCN) guidelines for colon cancer and the European consensus conference colon and rectum do not recommend laparoscopic surgery for locally advanced caner such as T4 cancer.14,15 Previous reports also showed that there is some caution to perform laparoscopic surgery for T4 cancer.6,16 In contrast, there are many reports that the laparoscopic approach is safe and feasible for T4 cancer.17,18 It is controversial to perform laparoscopic surgery for locally advanced colon cancer. In the present study, before case matching, the OPS group had deeper tumor (T3 & T4) than the LS group, but after case matching there was no significant difference. This result suggested that laparoscopic surgery for locally advanced cancer did not lead the worse prognosis than open surgery. The reason for the good prognosis for all-stage cancer, including deeper cancer, may be the existence of 3 surgeons who had certification from the Endoscopic Surgical Skill Qualification System (ESSQS) at our institute. When we have laparoscopic surgeries, at least 1 surgeon who has certification from the ESSQS performs or instructs the laparoscopic surgeries. It may lead to good prognosis, especially for LR.
The colon originates from the midgut and hindgut during embryonic development and differentiates into the right-side colon and left-side colon. Tumors in the cecum, ascending colon, and the proximal part of the transverse colon are defined as midgut tumors, while those in the distal transverse, descending, and sigmoid colon and the rectum are defined as hindgut tumors. Differences have been reported between right-sided and left-sided colon tumors in terms of clinical symptoms, incidence, molecular pathways involved, and oncologic outcomes, as well as embryologic origin.18–23 While such characteristics existed in the sidedness of the colon, there are no significant differences for OS and RFS between open and laparoscopic surgery in the tumor location in this study.
This study has some limitations. First, this study is a single-center retrospective study in design. Second, although we analyzed by propensity analysis to minimize this limitation, it is still limited by the richness of the available data and it might not be possible to make inferences due to hidden confounding. Six covariates were included in the model for calculating propensity scores, but other covariates were not included. Second, the sample size was relatively small. Third, there were no short-term outcomes such as blood loss, operating time, complications, and length of hospital stay in this study. We focused on long-term oncologic outcomes only in this study. More prospective surveys are needed for confounders and prognostic outcomes in our institute.
In conclusion, laparoscopic surgery appears to be a reasonable option with similar long-term outcomes to open surgery in colon cancer patients.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.