
Abstract
Background:
Gallbladder stones are a very common disease, with a prevalence of 21.9% in Argentina. The incidence of common bile duct stones (CBDS) varies with age and with the clinical presentation; ∼3%–10% of patients with gallbladder lithiasis have concomitant choledocholithiasis. In the past decades, the development of ultrasound and magnetic resonance cholangiography and endoscopic ultrasound has expanded for the preoperative diagnosis of gallbladder lithiasis.
Materials and Methods:
We describe the step-by-step technique using the single-operator cholangioscope (pSOC) (SpyGlass™ Discover; Boston Scientific, Natick, MA) under laparoscopic guidance, in a patient with huge stones in the bile duct that was treated with a choledocotomy.
Results:
The patient underwent the procedure well and the closure of the bile duct was with a primary suture. The current devices, standard cholangioscopes or bronchoscopes, only have a two-way deflection. This problem might be solved with the introduction of a new pSOC device (SpyGlass Discover; Boston Scientific).
Conclusion:
In conclusion, the combination of laparoscopy and pSOC is a feasible, safe, and effective technique for the treatment of CBDS, and may be considered as an alternative approach in clinical cases where gastrointestinal anatomy is altered or when endoscopic retrograde cholangio-pancreatography (ERCP) failed. pSOC has the potential to reduce peri-procedural adverse events and costs.
Background
Gallbladder stones is a very common disease, with a prevalence of 21.9% in Argentina. 1 This has led to constant progress in the implementation of new techniques for its resolution to have less complications regarding to it. Among the most frequent complications of this entity, ∼3%–10% of patients with gallbladder lithiasis have concomitant choledocholithiasis.2,3
In the past decades, the development of ultrasound and magnetic resonance cholangiography and endoscopic ultrasound has expanded for the preoperative diagnosis of gallbladder lithiasis. Likewise, with the advent of laparoscopic and endoscopic techniques for their treatment, it is clear that laparoscopic cholecystectomy is the treatment of choice. However, there is still no consensus on the best strategy for the treatment of gallbladder stones associated with common bile duct stones (CBDS). 4
Epidemiology
The incidence of CBDS varies with age and with the clinical presentation. The older you are and the presence of complications of the underlying gallbladder lithiasis, the greater the probability of suffering from a coexisting CBDS. For example, in carriers of symptomatic gallbladder lithiasis and in those <50 years of age, the probability of associated choledochal lithiasis is not >5%.3,5 However, if a patient presents with an acute cholecystitis, that probability rises from 15% to 20% if it arises as biliary pancreatitis. This figure increases up to 40% in the elderly with biliodigestive fistulas.3,6,7
Materials and Methods
Step-by-step technique
This is a 68 year-old man, with previous surgeries in the abdomen and typical history of biliary disease. An ultrasound was performed showing gallstones, intrahepatic bile duct dilatation, CBD of 11 mm, and a stone of 28 mm. Multiple ERCPs were done with no success to remove the stone. The laparoscopic surgical approach was chosen. We entered the abdomen with an open technique due to its previous surgeries and placed a 10 mm trocar at the umbilicus to insufflate the abdomen up to 14 mmHg. Then three more trocars were placed as described in Figure 1 (Two 10 mm and two 5 mm trocars).

Trocar placement (two 10 mm and two 5 mm).
Once the abdomen was entered the adhesions were freed with scissors and hook. Cholecystectomy was performed as usual. An intraoperative cholangiogram (IOC) was then performed and a stone bigger than the bile duct was demonstrated (Fig. 2). Owing to the size of the stone a choledocotomy was done and the first step was to remove the stones with a Dormia Basquet (Fig. 3). The choledocotomy was enlarged because of the size of the stone (Fig. 4). In the IOC more bile duct stones were demonstrated and a papillary dilatation with balloon was also performed (Fig. 5). The papilla can be seen (black arrow).

Intraoperative cholangiogram demonstrating common bile duct stones. A 28 mm stone.
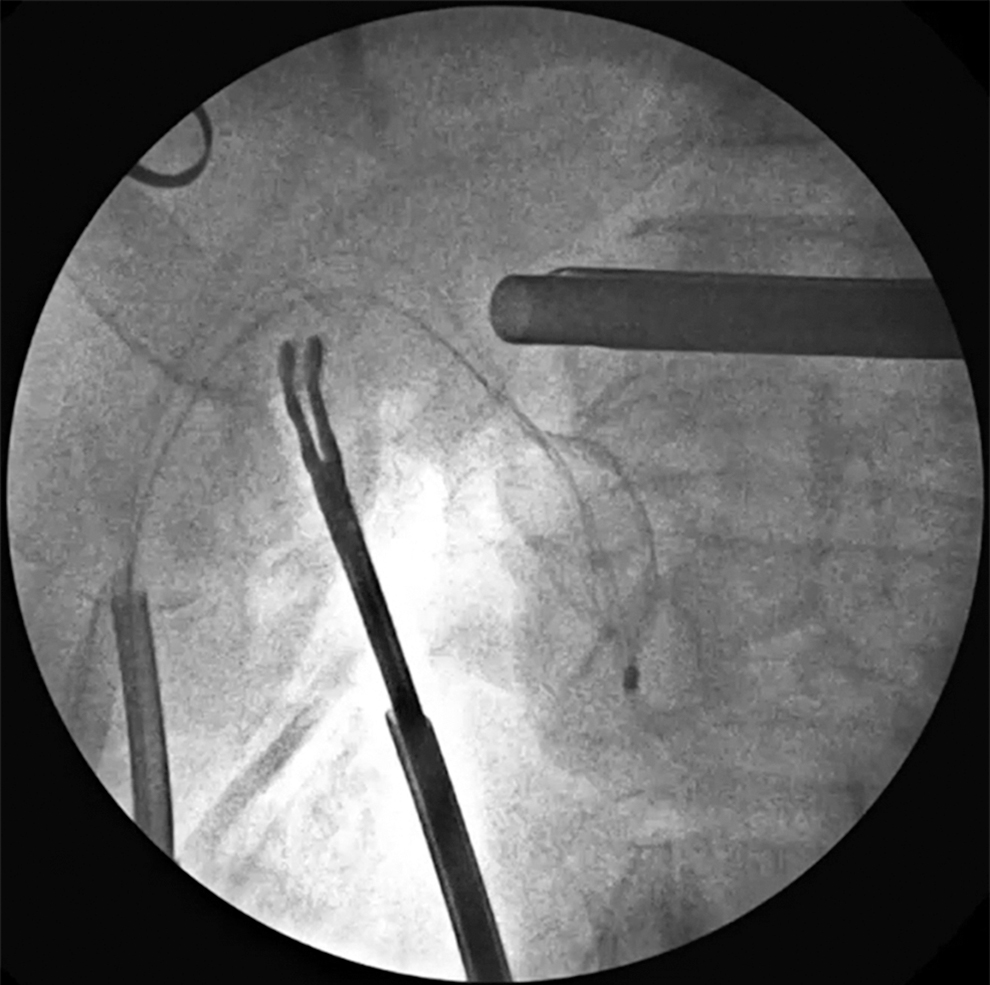
Stones removal by using a Dormia Basquet.
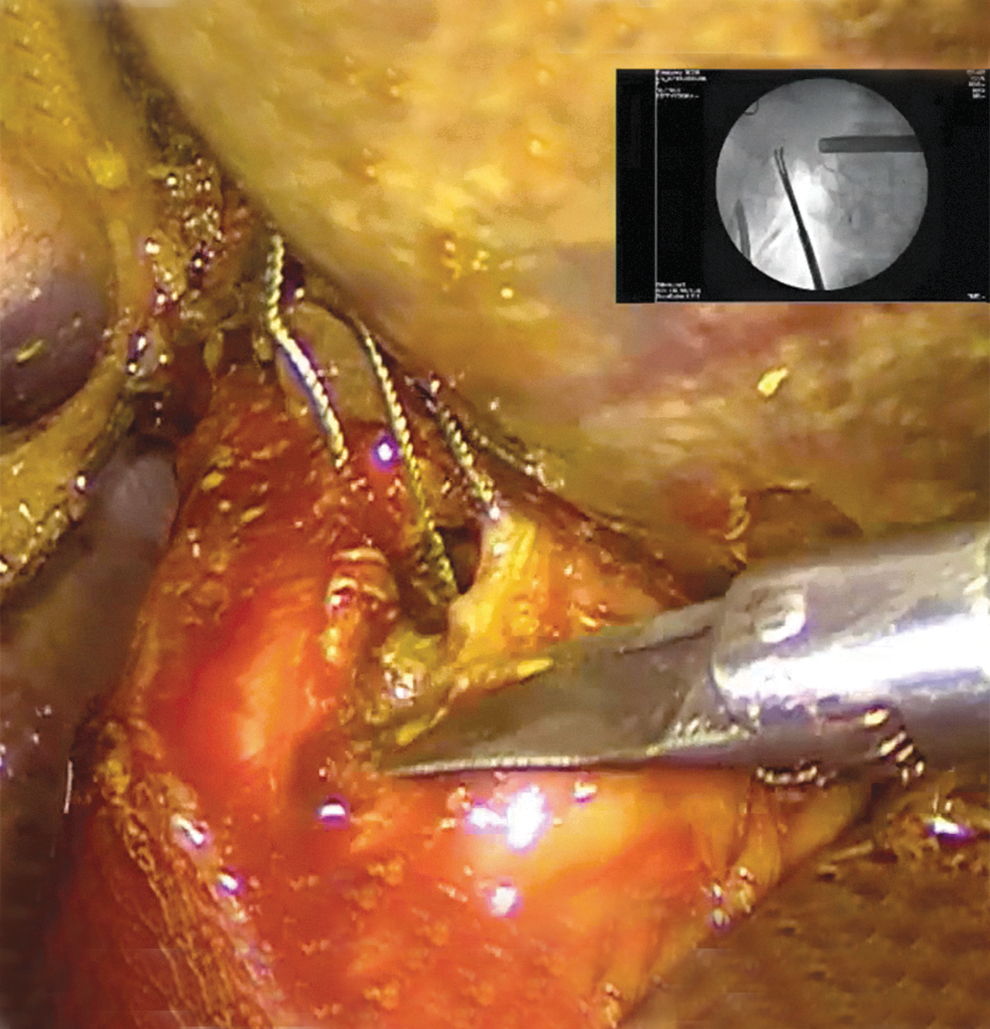
Choledocotomy is enlarged with scissors.
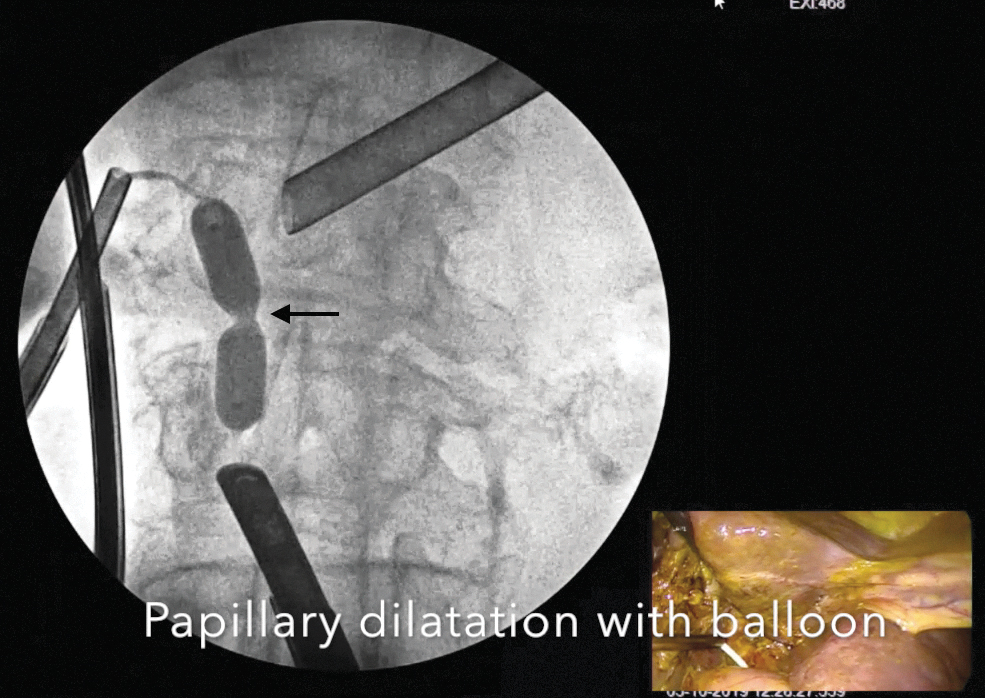
Papillary dilatation with balloon.
Owing to that multiple CBDS were observed, we decided to combine the laparoscopic approach with the single-operator cholangioscope (pSOC) (SpyGlass™ Discover; Boston Scientific, Natick, MA), it entered through one of the 5 mm trocar. In Figure 6, the device probe was inserted in the bile duct through the choledocotomy. With this device we finish the CBD cleaning and under direct vision we saw that the bile duct was free of stones on its proximal part (Fig. 7) and also in its distal part, where we can observe the duodenal mucosal after passing through the papilla with the device (Fig. 8). A final IOC was then performed (Fig. 9). To end the procedure a primary closure of the bile duct was done. And a JP drain was placed to the suture.
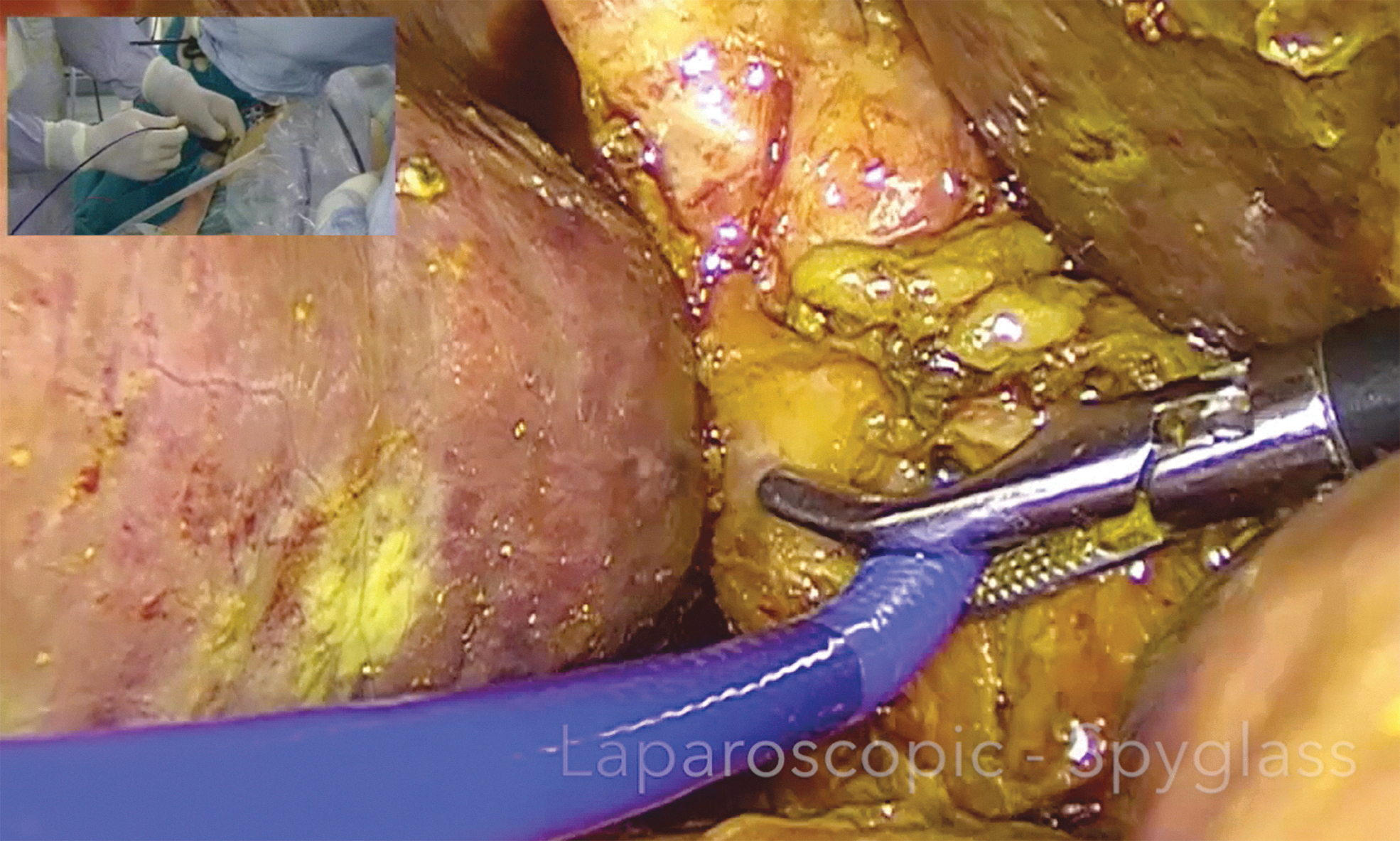
Insertion of the single-operator cholangioscope through the choledocotomy.
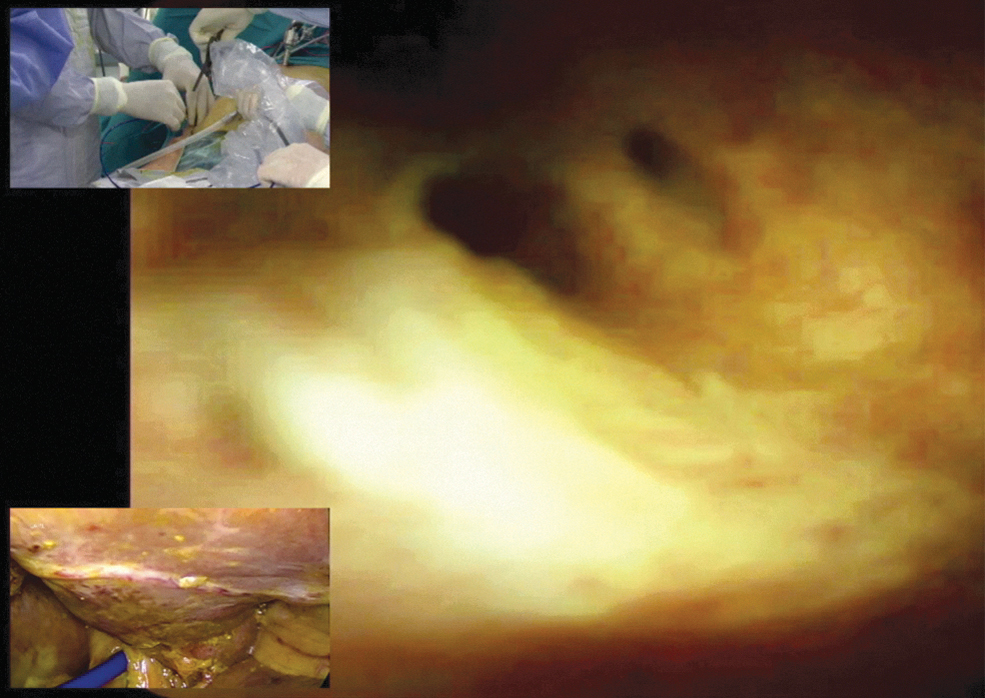
Single-operator cholangioscope view: proximal part of the common bile duct.

Single-operator cholangioscope view: distal part of the common bile duct and the duodenum.

Final intraoperative cholangiogram.
The patient underwent well, and was discharged uneventfully on postoperative day number 3.
Results
In the laparoscopic era, many developments or new materials and techniques allow us to treat these patients in a minimally invasive way. But in some places, the lack of training and practice with the laparoscopic technique, the lack of specific instruments, the absence fluoroscopy in operating rooms, the low financial remuneration on the part of health payers, and the lack of conviction make this disease nonequal worldwide.8–10
Nowadays, two main approaches are proposed:
One-stage treatment: It consists of carrying out, under a single anesthesia, the treatment of gallbladder and gallbladder lithiasis by laparoscopy. In these cases, the transcystic route represents a technique of high effectiveness and applicability with low morbidity and mortality. As an alternative, choledochotomy is an option in cases where the transcystic route is not advisable or fails (Dormia Basquets, Baloon, and Randall Forceps can be used).3,11 Treatment in two stages: It consists of the association of laparoscopic cholecystectomy with ERCP; it can be performed a preoperative or even a postoperative papillotomy with stone extraction.
3
The one-stage treatment has the following advantages:
(A) Given that the surgeon is trained to perform Intraoperative cholangiogram (IOC) and laparoscopic resolution of gallstones, few diagnostic preoperative resources are invested for choledochal lithiasis (ERCP and ERCP), with which they avoid the excessive costs caused by the sum of normal preoperative studies (index conditioned by the predictive factors of choledocian lithiasis used).3,12
(B) It has high applicability and effectiveness and low morbidity and mortality since many institutional and personal series confirm this statement.
(C) Finally, the patient receives a single anesthesia and the case is completely resolved in the operating room, not requiring subsequent treatments in another area performed by another team.3,12
When we analyze the current devices, standard cholangioscopes or bronchoscopes only have a two-way deflection that contrasts with the SOC system, with its two wheels enabling a four-way deflection of the device. The 2.14 m length of the device did not seem to have a negative impact on the success of the performed procedures. However, it may affect procedure duration, as it is more difficult to handle. This problem might be solved with the introduction of a new pSOC device (SpyGlass Discover; Boston Scientific). The digital SOC mini scope with a length of 2.14 m (SpyGlass Discover; Boston Scientific) is capable of a four-way deflection and uses a dedicated irrigation channel with an additional suction channel. It has a 3.46 mm outer diameter and a 1.2 mm working channel. For diagnostic procedures, SOC-guided biopsy was performed with a purpose-designed biopsy forceps that can be passed through the SOC mini scope (SpyBite™ Biopsy Forceps; Boston Scientific Corporation, Marlborough, MA). Lithotripsy was performed using a Holmium:YAG-laser (Auriga® XL, StarMedTec GmbH; 270 mm optical fiber 8 Hz, 2400 mJ) (Lumenis VersaPulse P20; 300 mm optical fiber 10 Hz, 2500 mJ) or using either a Lithotron EL27 electrohydraulic shockwave generator with a 2.4 French probe (Walz Elektronik GmbH, Rohrdorf, Germany) or an Autolith™ Touch Biliary EHL system with a 1.9F probe (Northgate Technologies, Inc./Boston Scientific) with power and number of pulses at the endoscopist's discretion. Intermittent irrigation with saline facilitated target stone visualization and lithotripsy.
Conclusion
In conclusion, the combination of laparoscopy and pSOC is a feasible, safe, and effective technique for the treatment of CBDS, and may be considered as an alternative approach in clinical cases where gastrointestinal anatomy is altered or when ERCP failed. pSOC has the potential to reduce peri-procedural adverse events and costs.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding were received for this investigation.