
Abstract
Background:
This study aimed to compare polypectomy during both insertion and withdrawal phase versus during withdrawal phase only.
Method:
We performed literature searching in PubMed and Ovid for randomized clinical trials (RCTs) that compared polypectomy during both insertion and withdrawal phase versus during withdrawal phase only on April 3, 2020. The primary outcome was adenoma detection rate (ADR).
Results:
Five RCTs published between 2012 and 2020 with a total of 2694 individuals were included in this meta-analysis. No significant difference was observed between the two groups for ADR (P = .99, odds ratio = 1.00, 95% confidence interval [CI] 0.84–1.19, I2 = 0%), or average number of adenomas per individuals (P = .53, weighted mean difference [WMD] = 0.04, 95% CI −0.09 to 0.17, I2 = 30%). Besides, polypectomy during both insertion and withdrawal group showed significantly longer time for insertion phase (P = .01, WMD = 2.16, 95% CI 0.47–3.84, I2 = 95%), and shorter time for withdrawal phase (P = .010, WMD = −2.32, 95% CI −4.09 to −0.56, I2 = 94%), although the total procedure time was not significantly different between the two groups.
Conclusion:
No obvious advantages were observed for polypectomy during both insertion and withdrawal phase. We are looking forward to the long-term outcomes of these studies. More studies are warranted in the future for further exploration, especially the detection rate of small lesions.
Introduction
Colorectal cancer (CRC) has become one of the most common carcinomas worldwide and brought great threat to human lives. 1 Up to now, colonoscopy is still regarded as the standard modality for CRC detection and the early screening of some precancerous lesions. 2 Previous studies have demonstrated that colonoscopy screening and surveillance could effectively prevent the risk for CRC, improve the prognosis, and further reduce the social burden. 3 However, we can see the incidence of CRC has been still high in the past decade. We think this could be related with the popularity of early screening program. Besides, the miss rate of polyp and adenoma during colonoscopy that has been pointed in previous literatures also should be of concern. 4
As we all know, colonoscopy examination is an unpleasant procedure when no anesthesia is given. 5 Successful colonoscopy should arrive at terminal cecum smoothly, which could base on adequate bowel preparation, skill of endoscopist, and individuals' tolerance as well. 6 In general practice, endoscopist would reach the terminal cecum as soon as possible in the insertion phase, without detecting or dealing with lesions in the bowel mucosa, which would be carefully performed in the following withdrawal phase. 7 However, several studies reported some lesions detected in the insertion phase would not be found in the withdrawal phase, especially for these with small size, leading to the miss rate and terminal recurrence. 8
As a result, in recent years, the viewpoint of polypectomy during both insertion and withdrawal phase has been proposed. Several randomized clinical trials (RCTs) compared polypectomy during both insertion and withdrawal phase with during withdrawal phase only, but the results were not consistent. Besides, the sample size of some studies was pretty small. Up to now, it is still a controversial issue. Therefore, this promoted us to perform this systematic review and meta-analysis to explore the clinical value of this proposal.
Materials and Methods
Search strategy
We conducted a systematic literature searching in PubMed and Ovid for studies that compared polypectomy during both insertion and withdrawal phase with during withdrawal phase only on April 3, 2020. The key search terms included “insertion OR insertional OR inserted” AND “colonoscopy OR polypectomy OR poly OR adenoma.” Besides, we also checked the references of articles and reviews for related studies that could be included in our meta-analysis. Ethical approval is not needed for this study because it's a meta-analysis.
Inclusion and exclusion criteria
The inclusion criteria for this study included (1) both insertion and withdrawal phase versus withdrawal phase only for polypectomy; (2) detail outcomes were reported; (3) RCTs. The exclusion criteria included (1) any type of studies without detail data, including review, editorial, correspondence, and conference abstract; (2) single-arm study.
Data extraction
All studies detected by primary searching were reviewed by Q.D. and S.T. A third reviewer (B.C.) would be consulted if controversy came out. Following items were extracted from the included studies including first author's name, year of publication, total patients, male patients, age, history of prior colonoscopy, indication for colonoscopy, and other reported outcomes in each group.
Outcomes of interests
Adenoma detection rate (ADR) was selected as the primary outcome.
The secondary outcomes included the number of adenomas per individuals, total procedure time, insertion time, withdrawal time, ease of the procedure, and individual's assessment of discomfort during the procedure.
Quality assessment
Q.D. and S.T. evaluated the quality of included studies by modified Jadad score system. 9 Besides, Cochrane risk of bias stool in Reviewer Manager was also used to evaluate the bias risk of included studies.
Statistical analysis
We used the Review Manager version 5.0 (The Cochrane Collaboration, Software Update, Oxford) for the data analysis. P < .05 was defined as statistically significant. Weighted mean difference (WMD) and pooled odds ratios (ORs) were calculated for the continuous and dichotomous outcomes, respectively. If only means and range values or median and range values were reported for continuous outcomes, the means and standard deviations would be calculated by methods described by Wan et al. 10 When both P < .05 and I2 > 50% were observed, heterogeneity were confirmed and a random-effects model would be used. Otherwise, a fixed-effects model was applied. Begg's funnel plot was used to evaluate publication bias. We only calculated the outcomes reported by three or more studies.
Results
The detail process and result of literature searching were showed in Figure 1. A total of 1942 studies were retrieved with the initial search algorithm. After removing duplications, there still remained 1291 studies. After reviewing titles and abstracts, only 35 relevant studies were kept for further evaluation. Besides, no additional record was identified through manual search. Among the 35 studies, 30 literatures were excluded for the following reasons: 26 were about new technique for colonoscopy, 2 were about the effect of position on colonoscopy, 1 was anesthesia related, and 1 was editorial. Finally, five RCTs published between 2012 and 2020 with a total of 2694 individuals were included in this meta-analysis.11–15
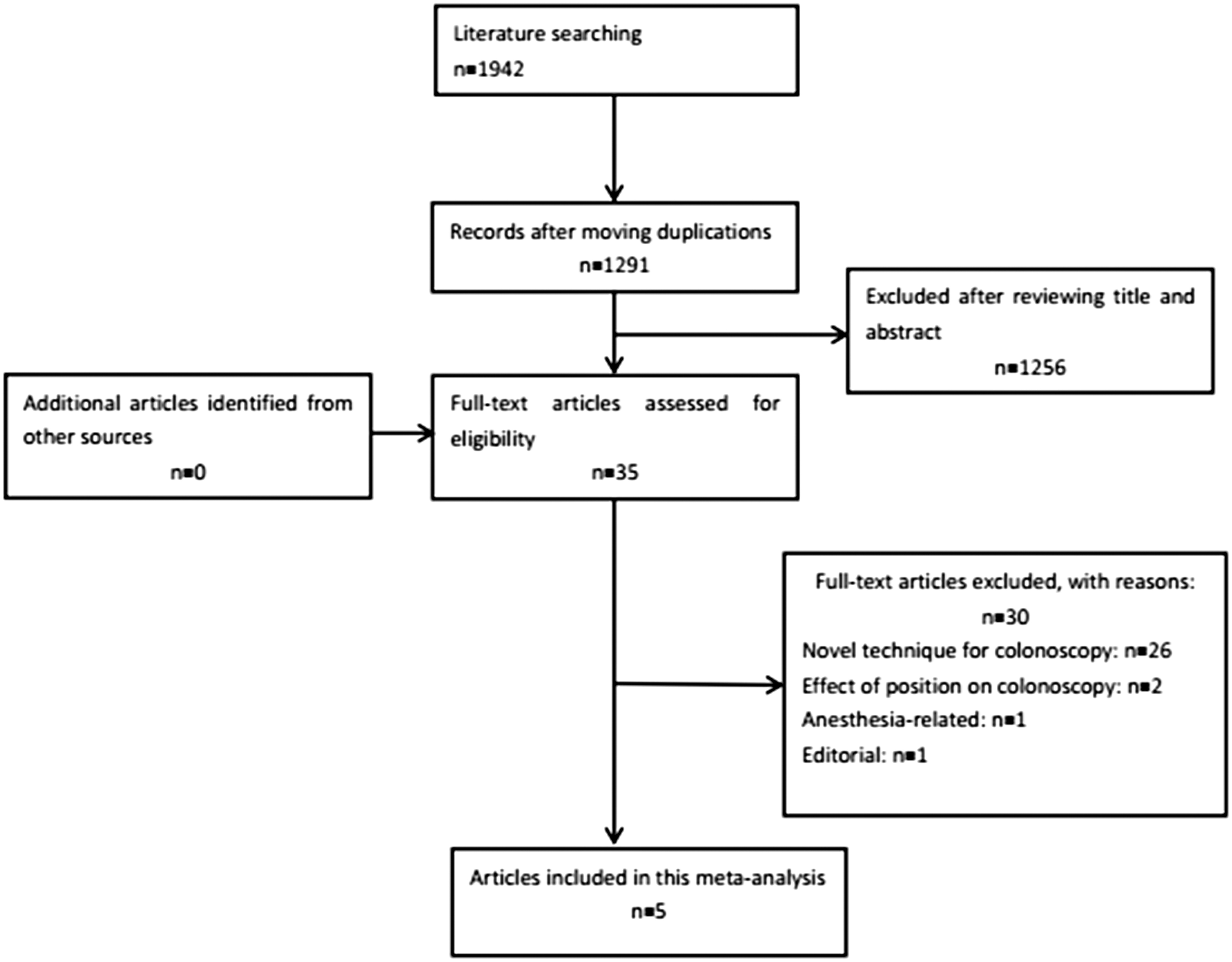
Preferred reporting items for systematic review and meta-analysis flow diagram.
Participants' demographics
No significant difference was observed between the two groups for the baseline information (Table 1).
Participants' Demographics
AI, artificial intelligence; BMI, body mass index; Con, conventional; RCT, randomized clinical trial.
Quality of included studies
All included studies were evaluated as high quality (Table 1). The assessment of risk bias for included studies was showed in Figure 2.
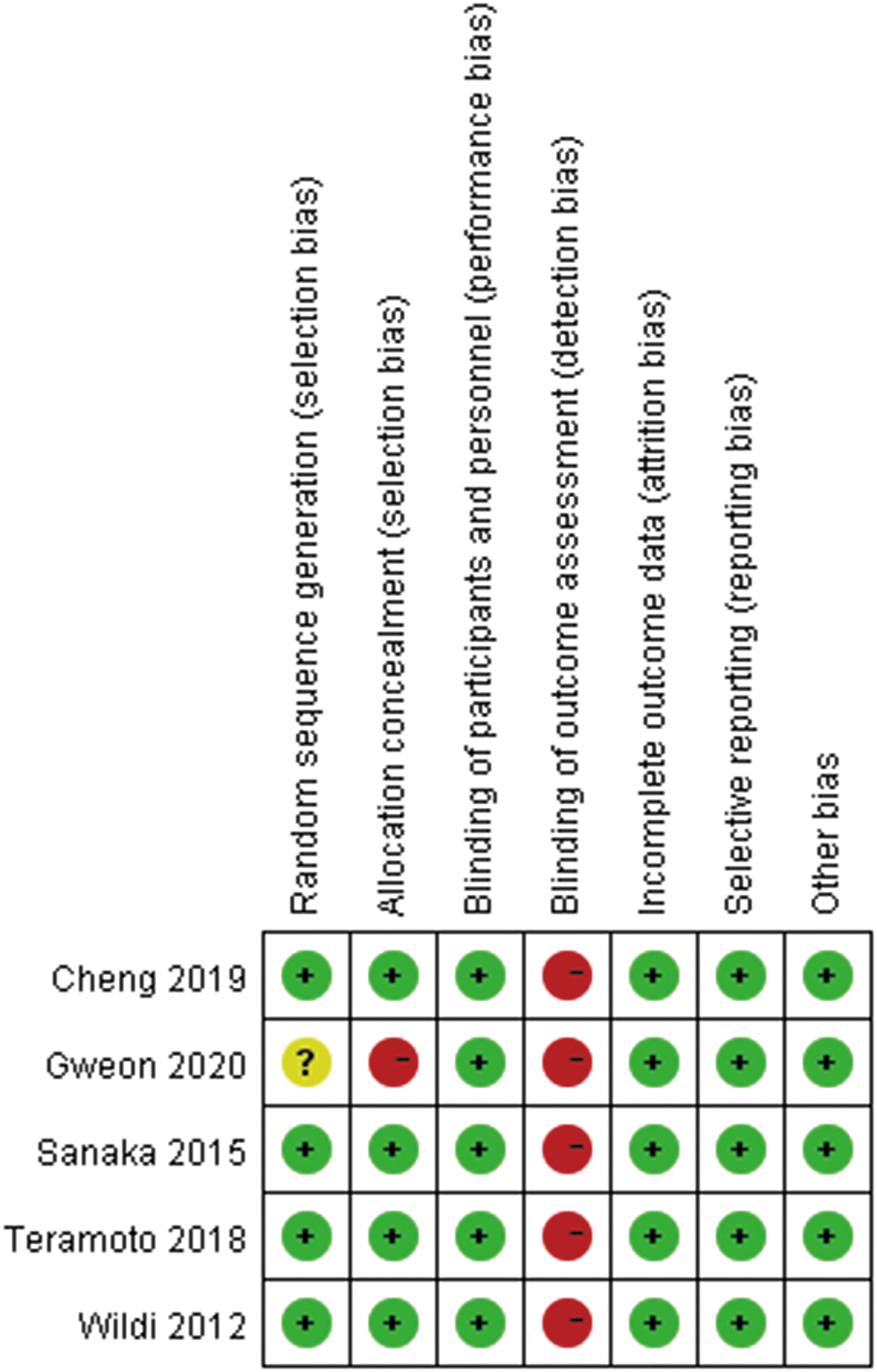
Cochrane risk of bias.
Primary outcomes
No significant difference was observed between the two groups for ADR (P = .99, OR = 1.00, 95% CI 0.84–1.19, I2 = 0%) (Fig. 3).
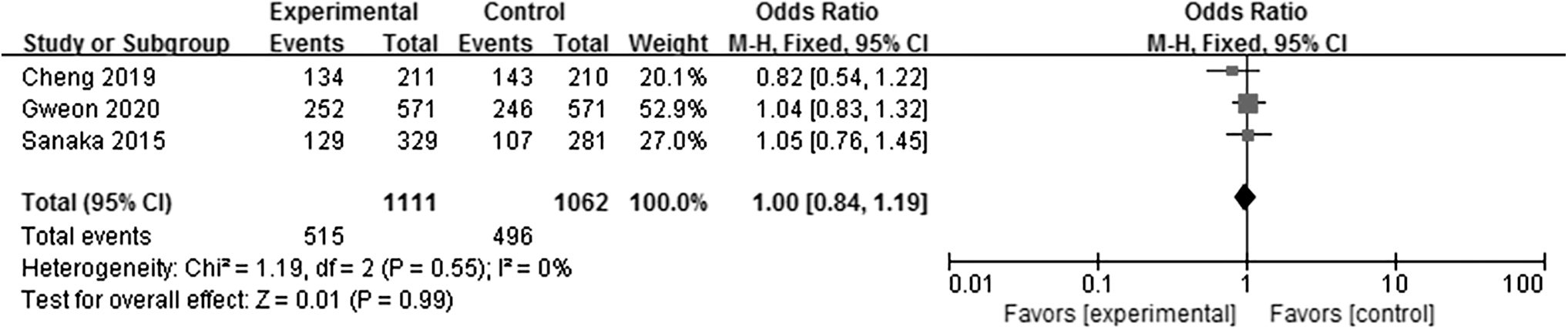
Meta-analysis for adenoma detection rate.
Secondary outcomes
The two groups had similar average number of adenomas per individuals (P = .53, WMD = 0.04, 95% CI −0.09 to 0.17, I2 = 30%). As for procedure time, no significant difference was observed between the two groups for total procedure time (P = .51, WMD = −0.70, 95% CI −2.78 to 1.37, I2 = 76%), but polypectomy during both insertion and withdrawal group showed significantly longer time for insertion phase (P = .01, WMD = 2.16, 95% CI 0.47–3.84, I2 = 95%), and shorter time for withdrawal phase (P = .010, WMD = −2.32, 95% CI −4.09 to −0.56, I2 = 94%).
In addition, the score for ease of the procedure (P = .32, WMD = −0.08, 95% CI −0.24 to 0.08, I2 = 86%) and individuals' discomfort (P = .71, WMD = 0.01, 95% CI −0.03 to 0.05, I2 = 30%) was also not significantly different between the two groups (Table 2).
Meta-Analysis of Secondary Outcomes
CI, confidence interval; OR, odds ratio; WMD, weighted mean difference.
Discussion
Missed polyp or adenoma during colonoscopy procedure is regarded as one of the main causes for the current high incidence of CRC. 13 Nevertheless, the traditional practice of colonoscopy was queried, for which the detection and polypectomy were performed in withdrawal phase only. 16 In recent years, several RCTs were conducted to explore whether detection and polypectomy in both insertion and withdrawal phase could improve the outcomes, but the results were not consistent. This promoted us to perform this study to summarize current available evidence for further exploration. Unfortunately, we did not observe obvious advantages for ADR with detection and polypectomy during both insertion and withdrawal phase.
Previous studies have demonstrated that increasing withdrawal time was associated with improved ADR in the traditional practice. 17 Although the study group in this meta-analysis had significantly shorter time than that in the control group, the ADR was still comparable. Obviously, adenomas detected in the insertion phase of study group contributed to this outcome, with the prolonged time for insertion procedure. Up to now, we still do not know whether prolong insertion time could be associated with increasing ADR as well. In the past, the reason for insertion phase without polypectomy was that endoscopists wanted to arrive at the terminal cecum as soon as possible and to reduce individuals' discomfort. 12 These are the basic guarantee of a successful colonoscopy examination. Detection and polypectomy during insertion would increase the phase time and delay the arrival at terminal cecum without doubt. Limited data showed this would not affect the cecum intubation rate. 14 According to the score of the ease of the procedure and individuals' discomfort between the two groups, it seems that detection and polypectomy during insertion phase would not bring additional trouble to endoscopists or individuals.
Previous literatures showed that polyps with large size (∼10 mm) could be dealt with in the withdrawal phase because the risk for missing of these lesions was relatively low. 11 More attention should be paid to the small lesions, especially for these are <5 mm in size. However, two studies included this meta-analysis reported no significant difference between the two groups for the size of detected lesions, regardless of any size category. 11 However, one study showed the larger size of polyps removed during withdrawal phase in the study group than that in control group, but the data were comparable between the two groups in another study. 15 In consideration of the sample size, more studies could be conducted in the future to focus on the affection on small lesions. In addition, although CRC could be transformed from the small polyps or adenomas, it would have an interval time about 2–3 years for the growth. 18 If the small lesions are missed in the first colonoscopy, it might be detected in the next examination. So, some authors also proposed the query that whether it is worthwhile for us to take great pains to change the traditional practice of colonoscopy, and in recent years, several techniques have been developed to improve the lesions detection rate in the withdrawal phase. 19 Nevertheless, even though several guidelines have recommended the optimal time interval for colonoscopy screening, the compliance of individuals are still not good enough, for colonoscopy examination is not a pleasant procedure.
The strength of this study should be highlighted. First, to our best knowledge, this is the first meta-analysis to synthesis the current evidence comparing detection and polypectomy during both insertion and withdrawal phase with withdrawal phase only. Second, all included studies were RCTs. The limitation of this study is that the number of included studies was not large and some outcomes that were reported by two studies were not taken. We are looking forward to further clinical trial. Besides, high heterogeneity was observed in some outcomes. Although we performed sensitivity analysis by removing one study each time, the outcomes remained unchanged. One the one hand, although all included studies were RCTs, it could not blind to endoscopist. The change for the traditional practice might influence the operation, even these with rich experience. On the other, one included study focused on the left-side colon and could contribute to the heterogeneity.
In conclusion, current evidence does not support detection and polypectomy during both insertion and withdrawal phase for colonoscopy examination. We are looking forward to the long-term outcomes of these studies. More studies are still warranted in the future for further exploration, especially for the detection rate of small lesions.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Natural Science Foundation of Zhejiang Province (LY15H030014).