
Abstract
Background:
Renal transplantation is the ideal treatment method for end-stage renal disease. Since deceased organ donation rates cannot meet the demand, live donor kidney transplantation (LDKT) is commonly performed worldwide. Laparoscopic donor nephrectomy (LDN) is currently the most commonly preferred minimally invasive donor nephrectomy technique. However, experienced surgeons should perform this procedure since the safety of the live donor is the priority in transplant practice. In this study, we aimed to investigate this procedure's safety at the hands of a surgeon during the transition period from open donor nephrectomy (ODN) to LDN.
Methods:
Data of the donors and recipients who underwent LDN and LDKT in Ankara Medicana Hospital between 2016 and 2019 were included in this study. Demographic, surgical, and immunological data of the donors and recipients were collected retrospectively. Donor data, including duration of surgery, warm ischemia time (WIT), complication rates, duration of hospital stay, and recipient data such as patient and graft survival rates, were compared with the published literature.
Results:
Two hundred donors and 200 recipients were included. The complication rate, surgical time, WIT at the donor site, and 1- and 3-year patient and graft survival rates were all comparable with the literature. Survival rates were irrespective of the relationship status of the donors with recipients.
Conclusions:
The LDN procedure can be safely performed by a surgeon with extensive laparoscopic surgery experience in general surgery cases and ODN.
Introduction
Kidney transplantation is the best treatment for patients with end-stage renal disease (ESRD), and it provides significantly better survival rates for patients than dialysis. 1 Refinements in surgical technique, improvements in postoperative care, individualized immunosuppressive treatment protocols, and increased rate of live kidney donations enhanced kidney transplant outcomes. 2 Besides, live donor kidney transplantation (LDKT) offers numerous significant advantages, including shorter waiting time for transplantation, higher quality renal grafts, elective surgical setting, and an opportunity for a preemptive transplant.3,4
Worldwide, the LDKT rate increased significantly after the implementation of minimal invasive donor nephrectomy techniques. 3 In our center, we performed ∼800 open donor nephrectomy (ODN) procedures between 2012 and 2016. In June 2016, we started implementing minimal invasive techniques. Herein, we analyzed the demographic, operative, and immunological data of donors who underwent laparoscopic donor nephrectomy (LDN) in our center. This analysis was followed by comparing our findings and survival data with those reported by international registries and other transplant programs.
Materials and Methods
This study was conducted under the Declaration of Helsinki Ethical Principles and Good Clinical Practices protocol and approved by the ethics committee of Ankara Medicana International Hospital. All patients were consented to be included in this study. All LDN and subsequent LDKT cases performed by the same surgeon (United States) in Ankara Medicana International Hospital between June 2016 and June 2019 were included.
The medical charts of the patients were reviewed retrospectively. Donor and recipient variables, including age, gender, body mass index (BMI), the relationship of the donor to the recipient, human leukocyte antigen (HLA), cold ischemia time (CIT), warm ischemia time (WIT), estimated blood loss (EBL), and surgical times, were all recorded.
During the donor selection process, an algorithm was used to determine the most suitable donor. Candidates who were older than 18 years were considered potential donors. Donor candidates with hypertension, diabetes, or obesity were not accepted. Normotensive, nondiabetic adults with no urological abnormalities or systemic illnesses with acceptable HLA matching, ABO blood group compatibility, and negative crossmatch with the recipient were accepted as appropriate candidates for donor nephrectomy. No ABO-incompatible transplants were performed. Candidates with abnormal renal function tests, blood biochemistry, or complete blood count results or patients with 24-hour urine creatinine clearance less than 100 mL/minute were not considered donors. All donors were informed about the outcomes of LDN and LDKT procedures. A formal psychiatric evaluation was also performed for all donors before the surgery.
A computerized tomography angiogram was performed for all donor candidates for the identification of renal vasculature. The left kidney with a single renal artery and vein was preferred when possible. However, since the presence of bilateral multiple renal arteries or veins is a common anatomical variation, we had to accept kidneys with vascular variations. In those cases, our preference was again the left kidney, when technically possible, to obtain an extra length of the renal vein.
LDN technique
The position of the donor was lateral decubitus in all cases. The first trocar was inserted periumbilically, and the abdomen was insufflated with carbon dioxide. A video-endoscope was introduced, and three to four additional trocars were inserted, as described previously. 5 The right or left hemicolon was dissected from the lateral abdominal wall and mobilized medially. Gerota's fascia was opened, and the kidney was dissected from the surrounding connective tissue. The renal vessels and ureter were dissected. Subsequently, an 8-cm Pfannenstiel incision was made, while maintaining pneumoperitoneum. The ureter was clipped distally and divided. This step was followed by an alignment maneuver for the approximation of the renal artery and vein so that the vascular stapler could fit in and safely include these two vessels. Before firing the stapling device, the endoscopic camera was angled at 70° to ensure there is no superposition of the vessels. An Endo GIA™ curved tip reload with Tri-Staple™ technology automatic cutting laparoscopic stapler was used to divide the renal vessels. Subsequently, the kidney was extracted by hand and cooled immediately. Pneumoperitoneum was re-established, and hemostasis was checked in the operative field. A closed-loop suction drain was placed at the surgical site through one of the 5-mm trocars. The Pfannenstiel incision was closed by continuously suturing the fascia with no. 1 loop polydioxanone stitch, and skin incisions were sutured using skin staplers.
Kidney transplantation technique
All recipients underwent renal transplantation through an extraperitoneal approach through a Gibson incision. Allograft vasculature was anastomosed in an end-to-side manner to the external iliac artery and vein in the right iliac fossa. An ice-soaked sterile swab was used to stabilize and cool the kidney during these anastomoses. Mannitol 10% was routinely administered before reperfusion.
Immunosuppression protocol
All recipients received risk-adjusted induction immunosuppression with either basiliximab or anti-thymocyte globulin (ATG) and intravenous methylprednisolone. Postoperatively, recipients received a triple-drug protocol, including prednisone, mycophenolate mofetil 2 × 1000 mg/day, and 0,15 mg/kg of extended-release tacrolimus for maintenance immunosuppression. Sulfamethoxazole-trimethoprim and valganciclovir were given as prophylaxis for pneumocystis pneumonia and Cytomegalovirus infection, respectively. Tacrolimus levels were maintained at 10–15 ng/mL for the first 6 weeks after transplant and between 8 and 12 ng/mL afterward. Two doses of methylprednisolone were administered as 500 mg intravenous infusions before and after transplant. This dose was then tapered to 250 mg once daily for 2 days. After discharge, patients were switched to a daily dose of 50 mg oral prednisone, which was gradually tapered down to a daily maintenance dose of 5 mg. Patients were followed up twice weekly for the first 6 weeks and once weekly for up to 3 months. After 3 months, patients were followed every 2 weeks for up to 1 year and then monthly. Patient survival was defined as the time between the date of transplant and date of death or last date of follow-up. Graft survival was defined as the time between the date of transplant and either date of graft failure (i.e., return to dialysis) or the last date of follow-up with a functioning graft.
Statistical analysis
Data were analyzed by SPSS 20 statistical software (SPSS, Inc., Chicago, IL). A two-tailed P-value <.05 was considered statistically significant. Categorical variables were reported as percentages, while continuous variables were reported as means and standard deviations. For continuous variables, group comparisons were analyzed using the Kruskal–Wallis test, Student's t-test, or analysis of variance followed by Bonferroni posttests in the case that overall P-value was significant. Categorical variables were compared with the chi-square test. Patient and graft survival rates were calculated by the Kaplan–Meier method, and the log rank test was used to compare the differences in survival.
Results
Donor and recipient relationship status
There were 200 LDKTs performed in our center during the study period. Among these donors, 42 (21%) were siblings, 40 (20%) were parents, 13 (6.5%) were children, 9 (4.5%) were second-degree relatives, 20 (10%) were third-degree relatives, and 5 (2.5%) were fourth-degree relatives of the recipients. On the other hand, 71 (35.5%) were unrelated donors, of whom 39 (19.5%) were spouses, 30 (15%) were friends, and 2 (1%) participated in a paired donation (Fig. 1).
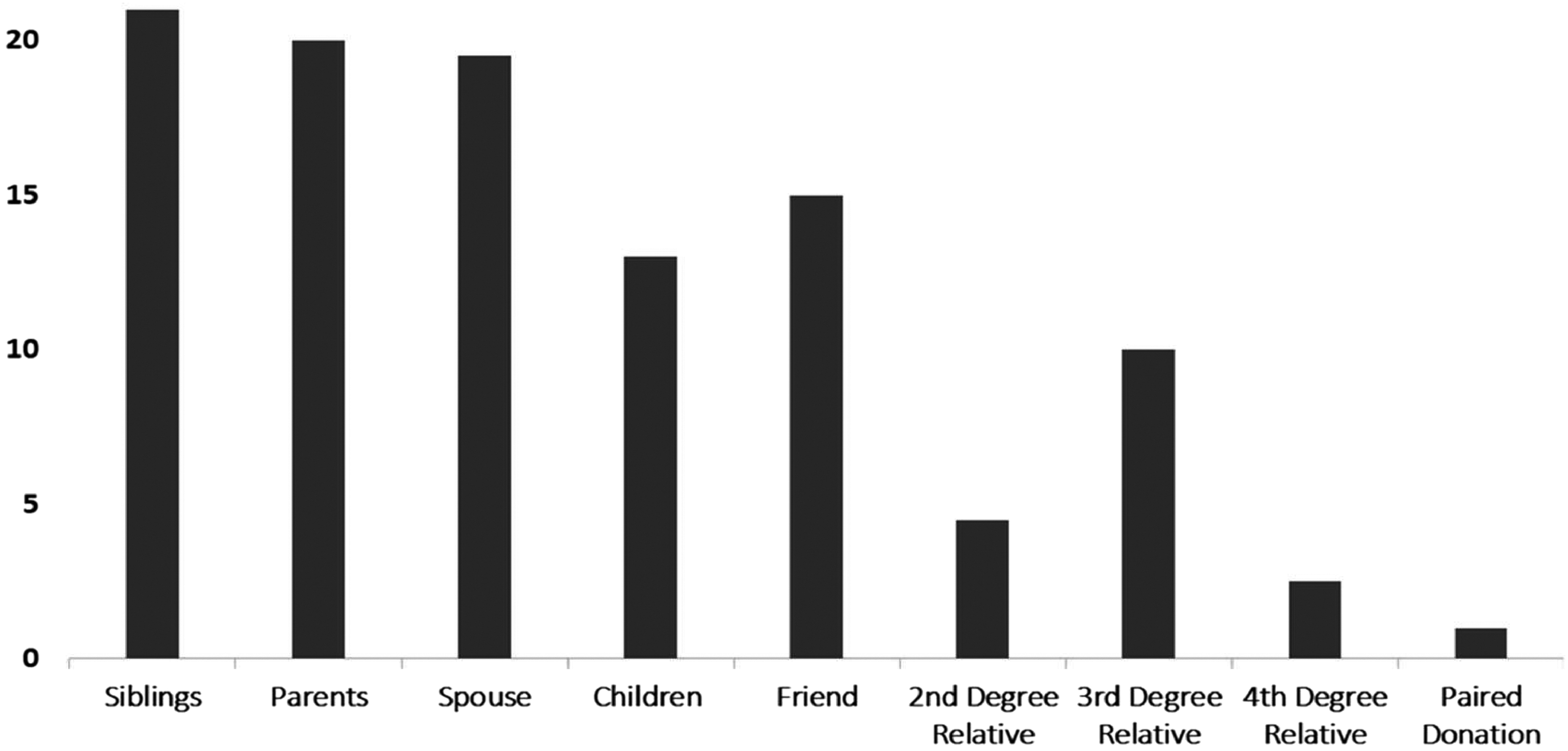
Donor and recipient relationship status in the study cohort.
Donor and recipient demographic and surgical data
Among 200 live donors, 103 (51.5%) were male and 97 (49.5%) were female, while among recipients, 129 (64.5%) were male and 71 (35.5%) were female. The mean donor age was 44.57 ± 13.0 years, whereas the mean recipient age was 43.40 ± 13.06 years (18–70). Mean BMI of donors and recipients was 29.9 ± 2 kg/m2 and 31.5 ± 1 kg/m2, respectively. In 166 (83%) cases, the left kidney, and in 34 (17%) cases, the right kidney was retrieved. Mean EBL was 120 mL (100–220). In 2 (1%) LDN procedures, conversion to the ODN procedure was required. One was converted to check a possible injury site at the descending colon, and the other one was converted due to sudden intraoperative bleeding, which started during hilar dissection. This patient did not require any blood transfusions or surgical re-exploration. Two patients (1%) had wound infection, and 1 (0.5%) patient developed a hernia at the Pfannenstiel incision site. Patients with wound infection were treated conservatively, while the patient with incisional hernia necessitated hernia repair. Demographic and surgical data of the entire cohort are shown in Table 1.
Demographic and Surgical Data of the 200 Consecutive Transplants
BMI, body mass index; EBL, estimated blood loss.
The mean surgical time of LDN and WIT at the donor site was 68.4 ± 14.7 (32–116) and 2.8 ± 1.2 (1.6–4.0) minutes. Mean CIT was 25 ± 10 minutes, whereas the WIT at the recipient site (i.e., anastomosis time) was 19.5 ± 10 minutes. The mean duration of recipient surgery was 123 ± 8 minutes. The mean length of hospital stay was 2.5 ± 1.5 and 9.5 ± 3 days for donors and recipients, respectively.
Patient and graft survival rates
HLA-A, HLA-B, and HLA-D typings revealed full antigen mismatch in 29 (14.5%), 5 mismatches in 30 (15%), 4 mismatches in 33 (16.5%), 3 mismatches in 53 (26.5%), 2 mismatches in 25 (12.5%), 1 mismatch in 13 (6.5%), and full antigen match in 17 (8.5%) transplants. Basiliximab and ATG were used for immunosuppression induction in 71 (35.5%) and 129 (64.5%) patients. The 1- and 3-year patient and graft survival rates for the LDKTs performed from first-degree relatives were 96%, 93%, and 93%, 84%, respectively. In the second-degree LDKT group, the 1- and 3-year patient survival rates were 94% and 90%, respectively, while the corresponding graft survival rates were 93% and 86%. In the live unrelated transplantations, the 1- and 3-year patient survival rates were 93% and 90%, respectively, and the corresponding graft survival rates were 83% and 78% (Fig. 2).
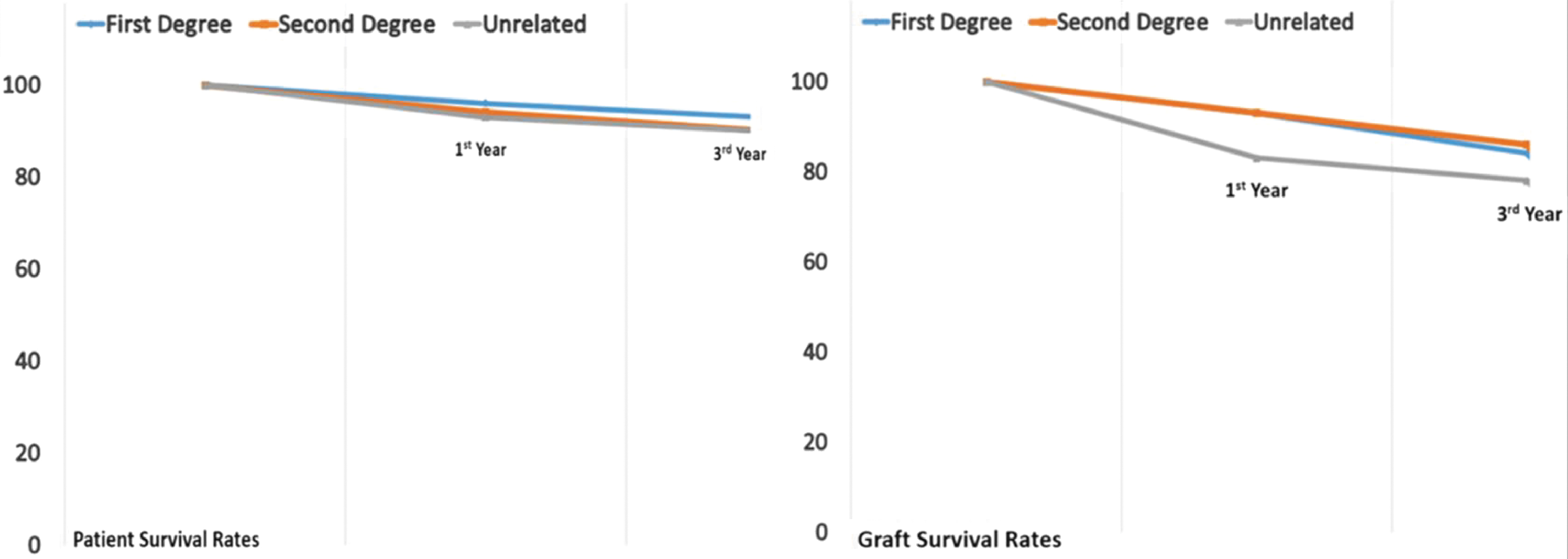
Patient and graft survival rates as per relationship status between the donors and recipients.
Analysis of the graft and patient survival rates as per HLA match/mismatch status of the donors and recipients revealed no difference between different HLA match/mismatch groups (P > .05). There was only one early graft loss in the entire cohort, and it was due to renal artery thrombosis.
Discussion
Renal transplantation is the most effective treatment for ESRD. 1 The LDKTs are being widely preferred since the organ demand cannot be met solely by deceased kidney donation. 2 Currently, the most preferred techniques for kidney retrieval involve minimally invasive approaches. 3 These techniques provide advantages such as quick postoperative recovery, less pain, better cosmetic outcomes, and low complication rates to the donor. 3 Among these techniques, transperitoneal LDN has gained more popularity than the others. 4 After considerable ODN experience, we have adopted the transperitoneal LDN technique to comply with the advancing trends in our center. During this adaptation period, we collected donor, recipient, surgery, and immunology data to analyze the outcomes of our 3-year experience with transperitoneal LDN. Despite the steep learning curve described for LDN, our results represent a smooth transition from ODN to LDN. An indication of this smooth transition is the low rate of conversion to open technique in our series. Besides, our LDN complication rate was also comparable with the rates reported in this literature.5,6 This uneventful adaptation may be due to our extensive laparoscopy experience in other general surgery cases, such as appendectomy, cholecystectomy, splenectomy, and colectomy. Our findings indicate that laparoscopic surgery experience achieved in these cases can be combined with the experience in ODN and transferred to LDN practice. Thus, the time needed for the completion of the learning curve can be shortened. Also, our mean surgical time and WIT were comparable with the literature. 5 These findings are especially important since it has been shown that there was a significant correlation between the surgical time of LDN and LDKT outcomes. 2 Our graft survival rates were also comparable with the current reports.5–7 Another critical parameter that affects the outcome of LDKT is the immunological compatibility of the donor and the recipient. 8 Argani described the role of HLA mismatches in LDKT and emphasized the significance of anti-HLA antibodies, leading to chronic allograft nephropathy and subsequent graft loss. 9 Sayin et al. evaluated the determinants of long-term graft function in a cohort of 288 transplant patients and showed that three or fewer HLA mismatches were associated with better graft survival. 10 In our study, analysis of patients with different numbers of HLA mismatches did not reveal any difference in the overall graft survival rates. However, it should be noted that our follow-up period was relatively short. Therefore, our analysis might have failed to reveal the long-term benefits of donor and recipient HLA compatibility.
According to the 2018 Turkish Ministry of Health data, 87% of kidney transplants were performed from live donors. 11 Current Turkish organ transplantation legislation allows third- and fourth-degree relatives to donate a kidney for transplantation. Third- and fourth-degree relatives constituted 12.5% of our live donor pool in our center. In our study, patient and graft survival rates did not differ with the degree of relationship between donors and recipients. Similarly, Gupta et al. examined the impact of this parameter on kidney transplant outcomes. 12 Their cohort included 122 recipients with 52 (42.6%) first-degree donors, 34 (27.9%) spousal donors, 12 (9.8%) second- or third-degree donors, and 24 deceased donors. In this study, there was no difference between these subgroups in terms of patient and graft survival rates.
Since its introduction in 1995, the LDN procedure has continuously evolved and become the gold standard technique for donor nephrectomies. 13 Moreover, renal allografts retrieved laparoscopically provided transplant outcomes comparable to those of ODN. 7 The advantages of LDN are also reflected in the studies that report an increase in live donation rates in the last decades. 14
Our series of 200 laparoscopic donor nephrectomies proved acceptable donor morbidity, while achieving favorable graft outcomes. Although retrospective in nature, this study proves that the adoption of transperitoneal LDN technique in a center experienced in ODN is feasible and safe, provided that the primary surgeon is experienced in other advanced laparoscopic general surgery cases.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.