
Abstract
Background:
Urethral catheterization is very common, considered a minor procedure done by physicians and well-trained nurses. However, in some traumatic or congenital cases, male catheterization is problematic. A multitude of techniques are available and still can utilize the natural urethral opening to manage this distressing situation. Among these techniques, cystoscopic-assisted retrograde catheterization and railroad techniques are reliable options. This article aimed to document application and to evaluate outcomes of both techniques for problematic male urethral catheterization.
Patients and Methods:
In our hospitals from February 2015 to March 2020, 167 boys with problematic urethral catheterization underwent cystoscopic-assisted catheterization technique over a guidewire and 6 cases underwent railroad technique due to failed cystoscopic-assisted technique. Both techniques were done under general anesthesia with the patient in supine position and their details will be presented later on.
Results:
Patients' mean age was 7.2 ± 2.9 years (range = 2–14). One hundred sixty-seven cases (96.5%) underwent cystoscopic-assisted catheterization, while only 6 cases (3.5%) were managed by railroad technique. For cystoscopic-assisted technique, mean operative time was 4 ± 1.5 minutes (range = 6–18). Mean follow-up period was 54 ± 1 months (range 6–60) with only 1 case developed urethral stricture. For the railroad technique, operative time was 7.5 ± 2.6 minutes (range = 10–34), mean follow-up was 45 ± 3 months with 3 cases developed vesicocutaneous fistula, and 4 cases developed residual urethral stricture.
Conclusion:
Cystoscopic-assisted retrograde catheterization is a minimally invasive, safe, and reliable technique to catheterize the exceptionally difficult male urethra.
Introduction
Urethral catheterization is one of the basic clinical skills widely performed in hospitals. 1 Catheterization indications include trauma general management, dilatation of stenosis/stricture, obtaining urine sample for urinalysis in neonates/infants, intraoperative identification/protection of urethra, bladder evacuation in lower abdominal/pelvic surgery, stenting urethral repair, clean intermittent catheterization for neurogenic bladder, and flushing mucus from augmented bladder (gastrocystoplasty).1–4 When problematic (as being difficult, failed, or contraindicated), several options exist as using Coude, council-tip or filiform catheter, urethral dilator, and guidewire mounted catheter. Urethral injuries are relatively common in pediatrics. They result from accidental or self-inflicted trauma, or instrumental manipulation. Iatrogenic urethral trauma causes one-third of anterior urethral strictures, with reported incidence of 3.2 per 1000 male admissions. 5 Other complications include gross hematuria (∼86% of cases), urinary retention, urinary tract infection (UTI), or stricture formation (estimated incidence of 3.4%).5,6 Iatrogenic injuries are preventable by education and catheter safety training programs; but when occur, they are distressing and costly as they require interventional procedures as urinary diversion, endourology, or operative repair; with each method having its own advantages, risks, and complications such as stricture formation, incontinence, and erectile dysfunction. With proper and timely management, excellent outcomes are anticipated.2,7 Herein, we aimed to document application and to evaluate outcomes of two techniques (cystoscopic-assisted over a guidewire and railroad) for management of boys with problematic urethral catheterization.
Materials and Methods
A retrospective study was conducted on 173 boys with problematic catheterization (Table 1), managed by cystoscopic-assisted retrograde over a hydrophilic guidewire technique, at Al-Houssain and Sayed Galal University hospitals, and Prince Mohammed Bin Abdulaziz hospital (PMAH), in the period from February 2015 to March 2020. Boys from 1 to 14 years of age with problematic catheterization due to trauma or difficult proximal hypospadias were included in the study. They included 159 emergency cases and 14 elective cases. Cases with complex urethral injury with massive contrast leak on radiography were excluded from the study. Primary outcomes included acquisition of adequate urine flow and incidence of UTI and bladder-cutaneous fistula formation. Secondary outcomes included incidence rate of stricture, incontinence, and erectile dysfunction. All cases were subjected to history taking, physical examination, and relevant investigations. Written informed consent was obtained from all patients enrolled. The study was approved by Institutional Review Board of Al-Azhar University hospitals and PMAH (Registration number: 00012367-15-01-005).
Important Parameters of the Study
FB, foreign body; SD, standard deviation; SP, suprapubic.
Initially in all cases, two trials to place catheter per urethra were done by the attending physician/nurse but failed.
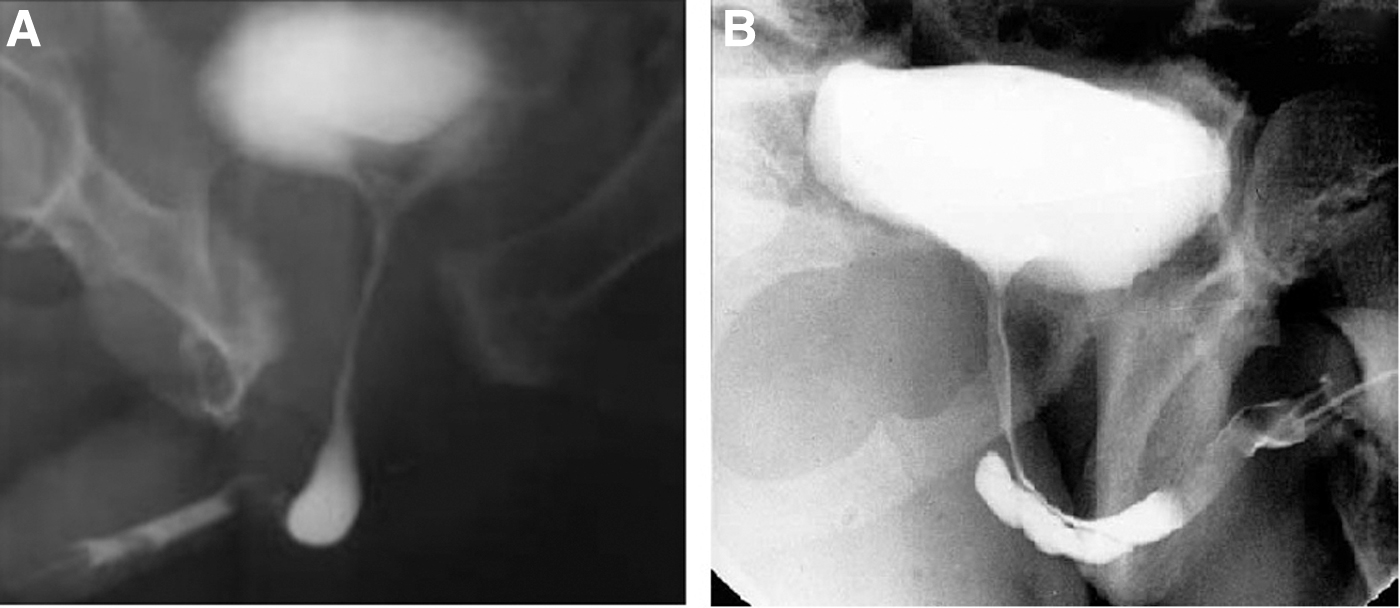
Plain radiography and computed tomography trauma with three dimensional formatting were done for accidental trauma cases and revealed fracture pubic ramus and diastasis of pubic symphysis in 27 cases, and fracture acetabulum and iliac crest with widened sacroiliac joint in 9 cases. Retrograde urethrography (RGU) revealed stretched but intact membranoprostatic urethra ( = type I Goldman classification) (Fig. 1A) in 27 of 36 pelvic fracture cases and isolated anterior urethral (penile/bulbar) injury ( = type V Goldman classification) (Fig. 1B) in the 94 local urethral trauma cases. It also revealed arrested dye/filling defect in self-inflicted transurethral foreign body (FB) insertion cases.
Procedures have been performed under general anesthesia by all the surgical team members equally.
Technical details
Cystoscopic-assisted retrograde over guidewire technique
The technique was performed on the same day of admission. Steps were as follows: according to patient's age, 6-to-14 Fr flexible cystoscope (Urology; Karl Storz®, Tuttlingen, Germany) containing a 0.035 Fr (0.89 mm) hydrophilic guidewire (SensorTM; Boston Scientific Corporation, Boston, MA) in its working channel was passed per external urethral meatus. The cystoscope was manipulated through the urethra until it reached the bladder cavity. Cystoscope was withdrawn; keeping the guidewire in-place, a Foley's catheter (after puncturing the center of its tip using a 20- or 18-gauge intravenous (IV) cannula and trocar held in the dominant hand and the catheter in the other hand, the pointed end of IV cannula and trocar was inserted from out-inside through the catheter's terminal side opening and directed toward the catheter's tip then advanced carefully until it punctured and appeared from the catheter's tip center) was threaded on the guidewire up to the bladder; its balloon was inflated with saline, followed by withdrawal of the guidewire (Fig. 2).
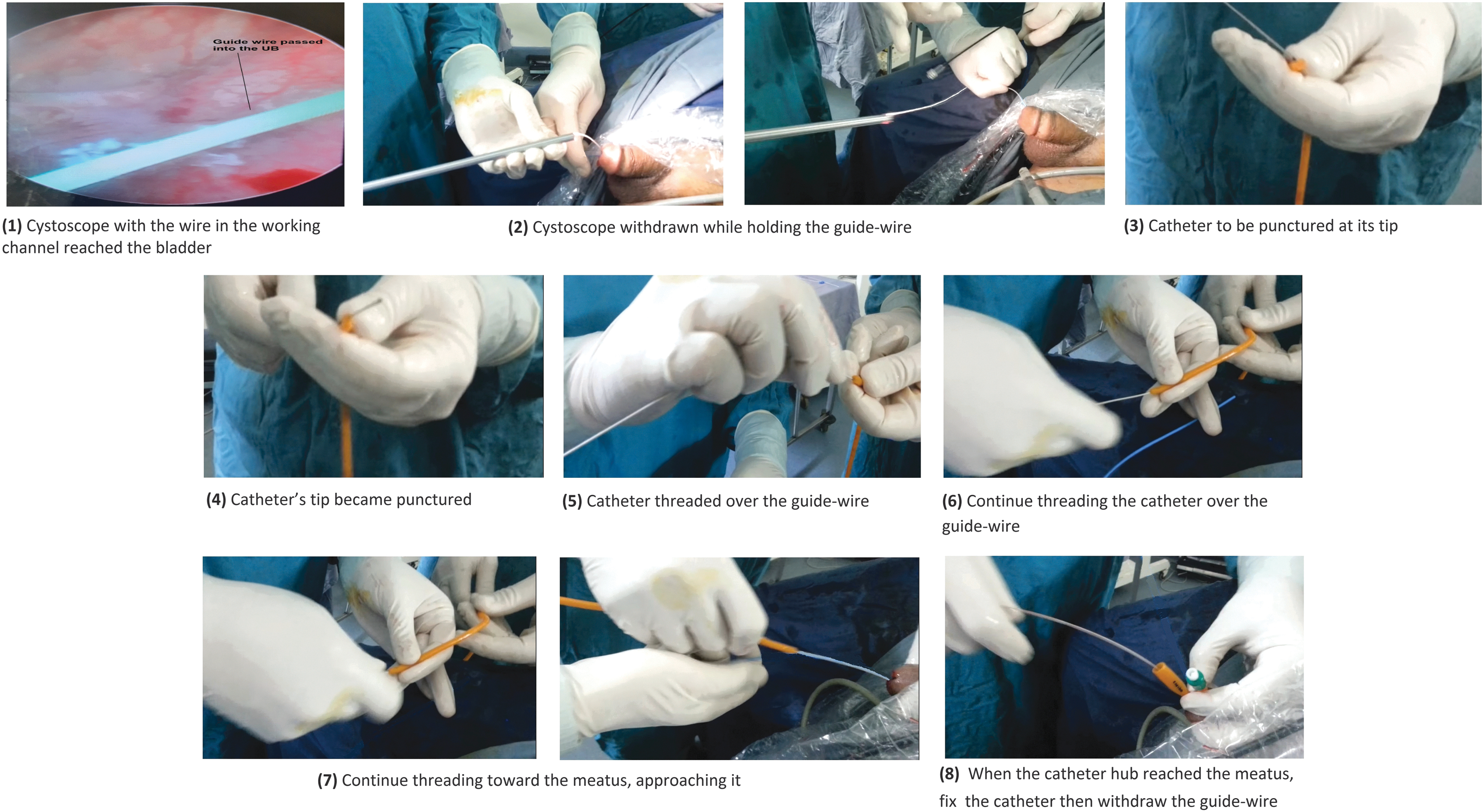
Steps of cystoscopic-assisted technique.
Railroad technique
It was performed for 3 cases of anterior pelvic fracture-associated cases and 3 cases of local urethral injury by impacted FB.
Steps (Fig. 3): It included antegrade insertion of a large size Foley's catheter via suprapubic (SP) cystostomy, blindly directing its tip toward the internal urethral meatus, advancing it through urethra until emerged from the external urethral meatus, snugly tying it by a thread to age-appropriate Foley's catheter, retrograde pulling of this catheter complex after lubricating it by sterile KY gel through the urethra until appeared from the SP opening, followed by cutting the connecting thread, then the vesical catheter was reinserted and its balloon was inflated and loosely tying the penile catheter to a thread protruding from the cystostomy to prevent accidental slippage and, after about 10–14 days, by cutting this thread, the penile catheter was left free to fall.

During the railroad technique, retrograde ± antegrade urethrography was done to assess for contrast leak, early stricture, or dilatation. At completion of the procedure, the view was as shown in Figure 4. Postoperatively, the patients were put under bacteriostatic (ampicillin or trimethoprim sulfamethoxazole according to age) coverage, catheter training (by alternative clamping and release), and stent care.
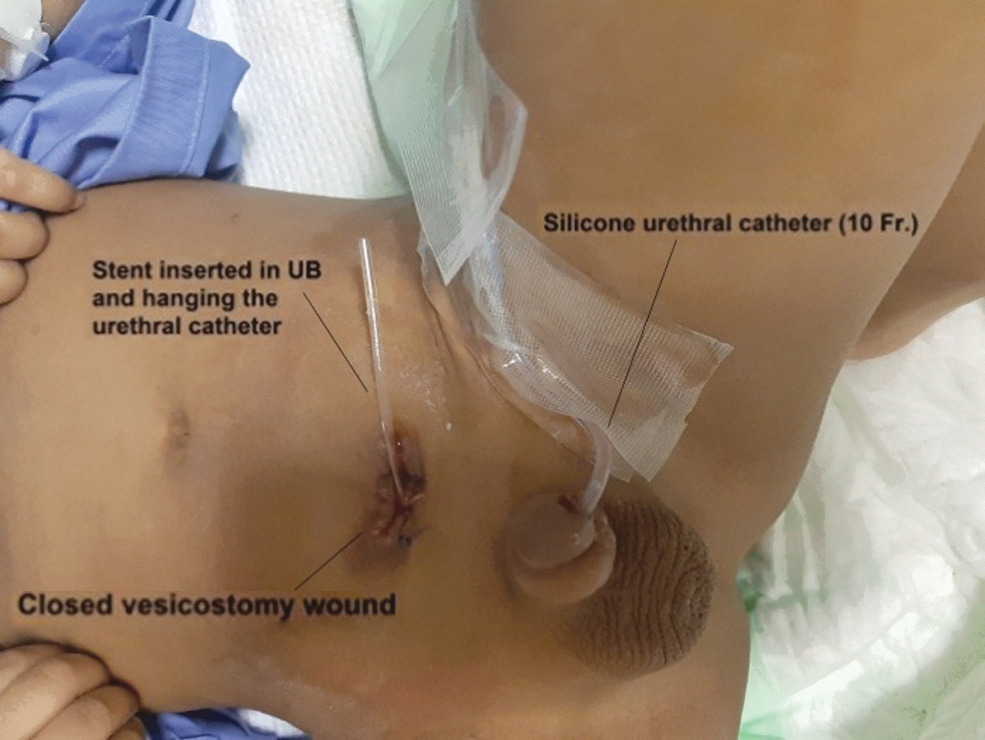
View at the completion of the railroad procedure.
Patients were followed up by regular urinalysis (to detect UTI), uroflowmetry (to assess urine stream flow rate), and ultrasonography (U/S) (to assess the urinary bladder [UB] wall thickness, presence of trabeculations, urine turbidity, and postvoid residual volume) in addition to on request (RGU for cases still complained of dysuria and straining). Patient compliance with follow-up was 100% (no patient loss to follow-up).
Statistical analysis
Data were analyzed using the statistical package for social sciences (SPSS) version 24.0 (IBM SPSS Statistics for Windows; IBM Corp, Armonk, NY). The measurement data are expressed as mean ± standard deviation, range, and average for continuous variables and frequency count and percentage for categorical variables.
Results
One hundred seventy-three boys with problematic urethral catheterization were included in the study. One hundred sixty-seven cases underwent cystoscopic-assisted retrograde technique, whereas 6 cases underwent railroad technique after initial SP catheter placement (Table 2). Overall mean age was 7.2 ± 2.9 years (range = 2–14 years). Mean operative time was 4 ± 1.5 minutes (range = 6–18 minutes) for cystoscopic-assisted retrograde technique and 7.5 ± 2.6 minutes (range = 10–34 minutes) for railroad technique. Mean follow-up period was 54 ± 1 months for cystoscopic-assisted retrograde technique and 45 ± 3 months for railroad technique. No patient was lost to follow-up.
Results of the Study
Significant difference between the two techniques with regard to parameters.
Short-term: <12 months of follow-up.
Long-term: ≥12 months of follow-up.
SD, standard deviation; SP, suprapubic; U/S, ultrasonography; UTI, urinary tract infection.
On RGU and during the cystoscopic-assisted retrograde technique, bladder neck was intact in all cases (no case had been found to have bladder neck injury or abnormality).
We found that 166 of 167 cases (99%) of the cystoscopic-assisted technique improved, while only 2 of 6 cases (33%) of the railroad technique improved.
Cases still complaining of difficulty and straining on micturition on follow-up were assessed by RGU (their number decreased with increased follow-up period denoting improvement). Uroflowmetry had been much improved with return of the normal bell-shaped curve of voiding in cases of residual stricture after successful endoscopic dilatation.
Eight cases with skull fracture and intracranial hemorrhage underwent operative intervention by the neurosurgical team, while 20 of 36 cases with pelvic fracture and 11 of 21 cases with lower limb (LL) fracture underwent fixation of their significant injuries by the orthopedic team.
Complications
UTI developed in 4 cases of railroad technique due to SP opening, which invited infection. Of the 6 cases managed by the railroad technique, 3 (50%) cases developed vesicocutaneous fistula, 2 of them were successfully sealed by topical application of sliver nitrate sticks, and 1 case required operative closure. Of the 167 cases that underwent cystoscopic-assisted technique, only 1 case (0.6%) suffered traumatic stricture (Fig. 5), but responded well to serial dilatation, whereas 4 of 6 cases (67%) of the railroad technique developed traumatic stricture with evidence of back-pressure changes on U/S, 3 responded to serial (3–5 sessions) cystoscopic dilatation over guidewire, and 1 case required eventual optical urethrotomy. None of the cases developed incontinence or erectile dysfunction. Eventual RGU (Fig. 6) and eventual U/S revealed normal.

RGU showing proximal penile urethral stricture. RGU, retrograde urethrography.
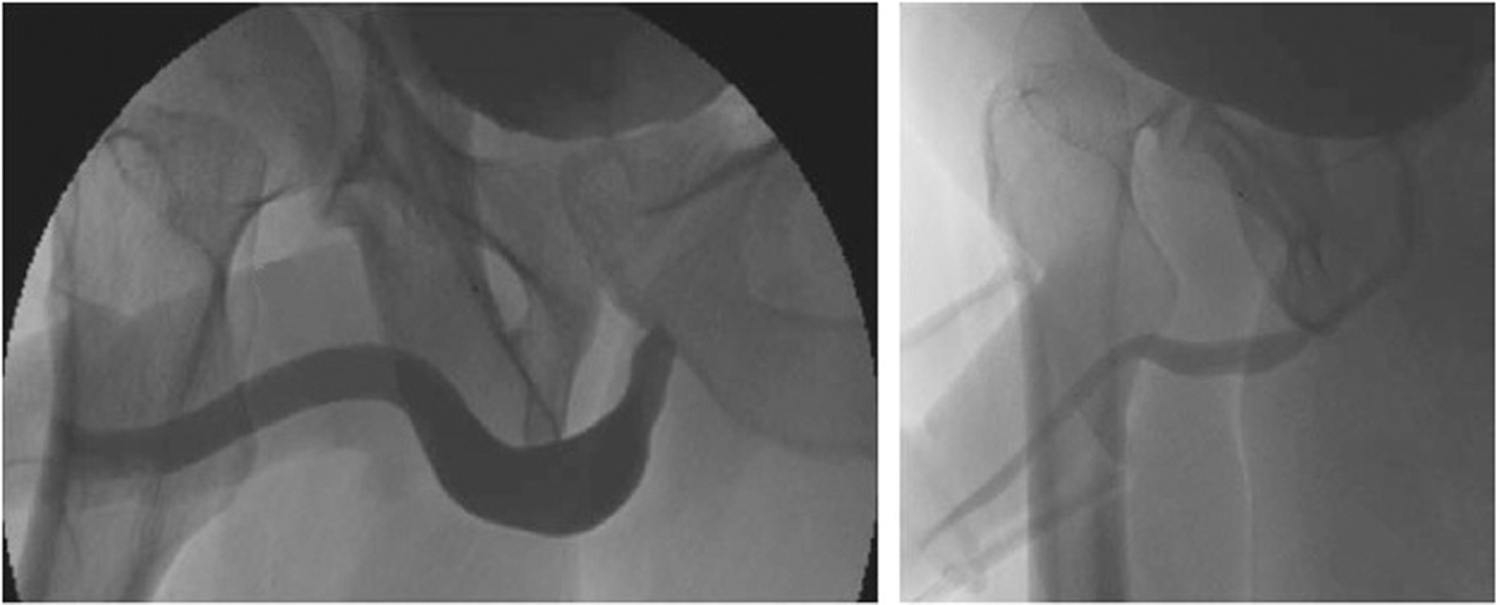
Eventual RGU revealed normal urethral anatomy. RGU, retrograde urethrography.
Discussion
About 25% of pediatric patients require urethral catheterization at a time during their health care course. 3 Urethral injuries are relatively common in children, with estimated incidence of ∼1 in 2000 general trauma victims and 3.4% of pediatric genitourinary trauma.8–10 Most urethral injuries are caused by major blunt trauma such as motor vehicle collisions or fall from height. These affect the posterior urethra and are commonly associated with pelvic fracture. Straddle injuries may lead to short- and long-term complications. 11 External penetrating trauma to the anterior urethra is rare and is usually caused by animal bite, gunshot, stab wound, and FB insertion. Iatrogenic urethral injury mostly results from difficult catheter insertion, transurethral procedures, or dilation and is a commonly reported event.3,9 They commonly affect anterior or posterior urethral segments. 8
Usually, the rationale in proximal hypospadias is the retrograde catheterization to stent the repair (urethroplasty) in early postoperative period. But, in unlucky cases with failed or difficult catheterization due to severe chordee or curled-up catheter or intra- or postoperative catheter slippage jeopardizing the repair for disruption, we have resorted to cystoscopic-assisted retrograde catheterization technique at the commencement of the surgery to stent the urethra and support and save the repair.
In our study, cystoscopy failed to progress (due to poor visualization) in only three cases of general trauma anterior pelvic fracture-associated urethral injury due to hematoma and edema at injury site and in another 3 cases with local urethral trauma by FB insertion due to impacted object; so, percutaneous SP cystostomy was done to temporarily decompress the bladder, followed later on (after 7–10 days) by railroad technique to stent the urethra. This time interval was to give a chance for the injured tissue to regain its vitality and edema to subside.
There is great debate about the optimum initial treatment for the emergency cases, but mainstays include drainage of the UB, mainly with a SP catheter followed by primary endoscopic realignment of the urethra if possible or, if this failed or was unavailable or with complicated critical case, delayed repair is a better option. A treatment modality mainly for adults is the early careful fluoroscopic-guided urethral catheter insertion. This can be performed at the time of injury, using interlocking sounds or catheters via both retrograde and antegrade approaches. 3
Early endoscopic realignment for adult patients using a combined transurethral and percutaneous transvesical approach may be a safe option. By that time, the patient's general condition has usually improved, pelvic hematoma has stabilized, and hemorrhage and sepsis no longer exist.10,12–14 Moudouni et al. described early endoscopic realignment of posterior traumatic urethral disruption. 15
Jepson et al. utilized several endourological techniques to treat 8 patients with average time to realignment was 9.5 days. 12 Olapade-Olaopa et al. also used variable endoscopic techniques for primary endoscopic realignment of posterior urethral trauma. 16 Ying-Hao et al. were first to use the technique of urethroscopic realignment for treating 16 patients with ruptured bulbar urethra. 17 Ku et al. compared immediate versus delayed treatment of bulbar urethral disruption. 18 All these authors had found endoscopic technique to be safe, ideal, and successful.
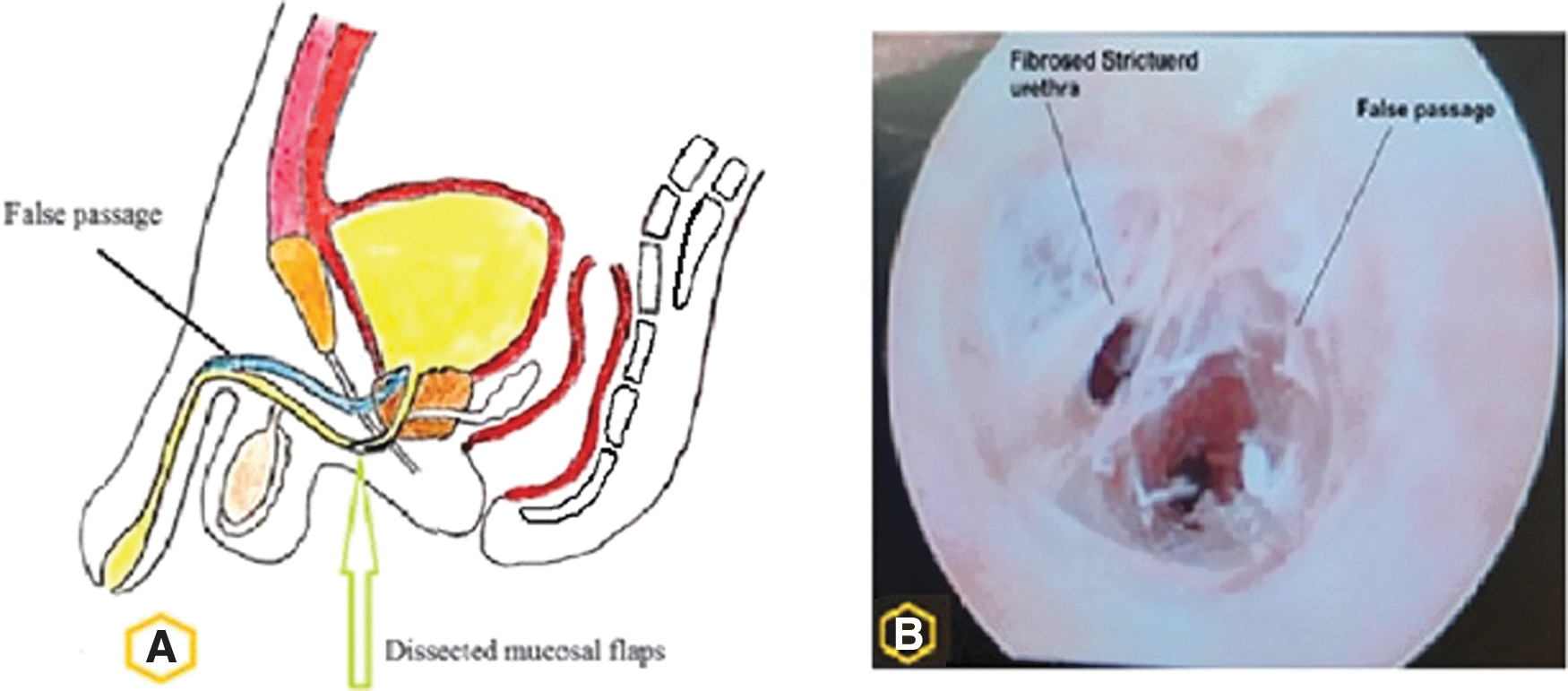
Dissected mucosal flaps (acting as one-way valve) and false passage are consequences and, also, possible causes of difficult urethral catheterization (Fig. 7). About 90% of false passages occur at the posterior urethra.4,7,19 Other possible cause of problematic catheterization is sphincter spasm, especially in young anxious patient with acute urine retention. In the younger anxious patients, sphincter contraction is strong and should be suspected so, with absent signs of urethritis or prior urethral manipulation; adequate patient sedation must be assured and gentle advancing of the catheter should be steadily kept until the sphincter yields.4,20
In every case, fully inserting the catheter up to the Y hub (bifurcation) confirms that it reached the UB and avoids premature balloon inflation that injures the urethra with resultant significant hematuria.20,21
In our study, general trauma cases required catheterization to facilitate the patient care (as they were unconscious due to head injury or bed-ridden due to pelvis or LL fracture and monitor hydration status (by measuring urine output). In local urethral trauma cases, the need for catheterization arose urgently as they presented with acute urine retention, agonizing SP pain, and full bladder.
We think that vesicocutaneous fistula occurred in railroad technique due to badly healed SP opening.
These results indicate that the cystoscopic-assisted retrograde technique is superior to the railroad technique on short-term outcome, then both techniques are nearly similar on long-term outcomes. Villanueva and Hemstreet, 22 Lachat et al., 23 and Zammit and German 24 also documented feasible successful utilization of endoscopic-guided hydrophilic guidewire technique for difficult urethral catheterization.
In our study, we adopted Goldman et al. classification for urethral injury. 25 All our cases were managed nonoperatively with excellent outcome; few easily managed complications, and reasonably long follow-up period. There was relatively high incidence of UTI and stricture formation in the railroad technique because it had been done in a delayed manner on top of SP catheter placement, which invited infection. Also the railroad technique entails use of two catheters in opposing directions (one antegrade and the other retrograde) passing to-and-fro via the urethra; which poses more invasion and manipulation to the fragile urethra. No case in our study has developed incontinence or erectile dysfunction as the bladder neck and penile innervation were intact.
Cystoscopic-assisted retrograde technique enables urethral catheterization under direct vision thus, avoiding conversion of a potential partial tear into complete one. It functions to stent the urethra until restores its continuity.
To the authors' knowledge, cystoscopic-assisted over a guidewire technique had not been satisfactorily documented before in pediatric literature although many authors utilized it, mainly in adult patients. This technique is minimally invasive, safe, and reproducible, so, worthy to be educated to junior physicians. It utilizes the natural urethral orifice without need to create an extra-opening SP that may invite UTI. Also, when necessary, it can be applied deliberately in both emergency and elective cases.
In conclusion, we found that cystoscopic-assisted retrograde catheterization is a reliable and accurate method to catheterize the male urethra and it offers excellent outcomes with minimal complications, whereas the railroad technique should now be abandoned in the current era of endourology and miniature pediatric instruments.
Drawbacks, limitations of the study, and future recommendations
Sample size of the study may be a drawback. None of our traumatic cases underwent operative repair of his injury. Further studies handling operative management of urethral injuries on larger sample size are required for comparison to yield more meaningful generalizable results and conclusions.
Footnotes
Authors Contributions
Study conception and design: M.A.M.; Data acquisition: M.A.D. and A.S.S.B.; Analysis and data interpretation: A.A.H.; Drafting of the article: M.A.M. and M.S.; Critical revision: K.Z.A. and M.H.H. All authors have read and approved the final article.
Acknowledgments
The authors acknowledge their colleagues in Urology Department for cooperation and provision of the supplies used in cystoscopic-assisted technique.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.