
Abstract
Introduction:
Trauma is a leading cause of death in young patients. The prevalence of blunt and penetrating trauma varies widely across the globe. Similarly, the global experience with laparoscopy in trauma patients also varies. There is a growing body of evidence to suggest that laparoscopy is feasible in trauma patients. We sought to contribute to these data by reporting our experience with laparoscopic management of blunt and penetrating trauma in a Belgian center.
Materials and Methods:
We retrospectively collected data on all trauma patients admitted to the Saint-Pierre University Hospital in Brussels, Belgium, over the 4-year period from January 2014 to December 2017. Hospital records for patients subjected to exploratory laparoscopy were retrospectively reviewed, and a descriptive analysis was reported.
Results:
There were 26 patients at a mean age of 40 years treated with laparoscopic exploration for injuries from blunt trauma (7), stab wounds (14), and gunshot injuries (5). The median interval between the arrival at the emergency unit and diagnostic laparoscopy was 175 minutes (range: 27–1440), and the median duration of operation was 119 minutes (range: 8–300). In all patients who underwent laparoscopy for trauma, there were 27% overall morbidity, no mortality, 11% reoperation rate, 7.4% conversions, and 19% incidence of negative laparoscopy. The median intensive care unit stay was 3 days (range: 0–41), and median total hospital stay was 7 days (range: 2–78).
Conclusions:
Laparoscopy is a safe, feasible, and effective tool in the surgical armamentarium to treat hemodynamically stable patients with blunt and penetrating abdominal trauma. It allows complete and thorough evaluation of intra-abdominal viscera, reduces the incidence of nontherapeutic operations, and allows therapeutic intervention to repair a variety of injuries. However, it requires appropriate surgeon training and experience with advanced laparoscopic techniques to ensure good outcomes.
Introduction
The management of blunt and penetrating abdominal trauma (PAT) has evolved over the past four decades. Laparotomy was considered standard management until the 1970s when there was a paradigm shift toward nonoperative management (NOM).1,2 This was fueled by recognition that up to 40% of trauma patients underwent nontherapeutic laparotomies, with their attendant complications.1,3 These included anesthetic complications, wound dehiscence, surgical site infections, incisional hernias, and prolonged hospital stay.1,3 Due to the reliability of diagnostic and interventional imaging, there has been a reduction in the proportion of negative laparotomies over the course of the last four decades.1,4,5 Another major change occurred toward the end of the 20th century, with the widespread acceptance of minimally invasive surgery (MIS) for most abdominal conditions in elective 6 and emergent settings.7,8 Early reports of MIS in trauma suggested that there was a high rate of missed injuries, ranging from 41% to 77%, 9 but this significantly reduced with the development of new technologies, better instrumentation, and improved surgical experience. Current data suggest that there is little difference in the rate of missed injuries compared with laparotomy, 3 and there is additional advantage of being able to repair injuries with the MIS approach. 10 There is an additional benefit in patients with PAT to detect simple penetration of the peritoneum.3,8,11 Although its utility in patients with blunt abdominal trauma (BAT) is less robust, there is still a role for MIS when there is the suspicion of diaphragmatic or hollow visceral injuries.12–14
In keeping with these changes, there has been an increase in the utility of MIS to manage hemodynamically stable trauma patients in our setting. We carried out this study to retrospectively evaluate the outcomes of MIS for trauma at our institution and also to review the existing literature in support of MIS for the abdominal trauma.
Materials and Methods
This study was carried out at the Saint-Pierre University Hospital in Brussels, Belgium. The institutional review board granted permission to access hospital records over a 4-year period between January 1, 2014 and December 30, 2017 for this study. All patients with BAT or PAT who were subjected to MIS were identified. Their hospital records were retrieved for detailed retrospective analysis.
At this facility, the decision to proceed to operation, choice of surgical approach, and need for conversion were wholly determined by the attending clinicians and were based on clinical parameters. Only hemodynamically stable patients were offered MIS. Hemodynamic stability was defined as the absence of catecholamine support or massive transfusion upon arrival at the emergency unit. The MIS approach was not offered to any patient with hemodynamic instability, intracranial injuries, major chest trauma, massive evisceration, and/or pregnancy. If these patients required operation, they were subjected to open surgery.
Penetrating trauma
Patients with penetrating trauma were resuscitated according to advanced trauma life-support protocols, and they were treated according to our management protocol for PAT (Fig. 1). Patients with limited evisceration had the viscera reduced and the peritoneum closed before laparoscopic exploration. Patients with massive evisceration were subjected to laparotomy for exploration of the abdomen.
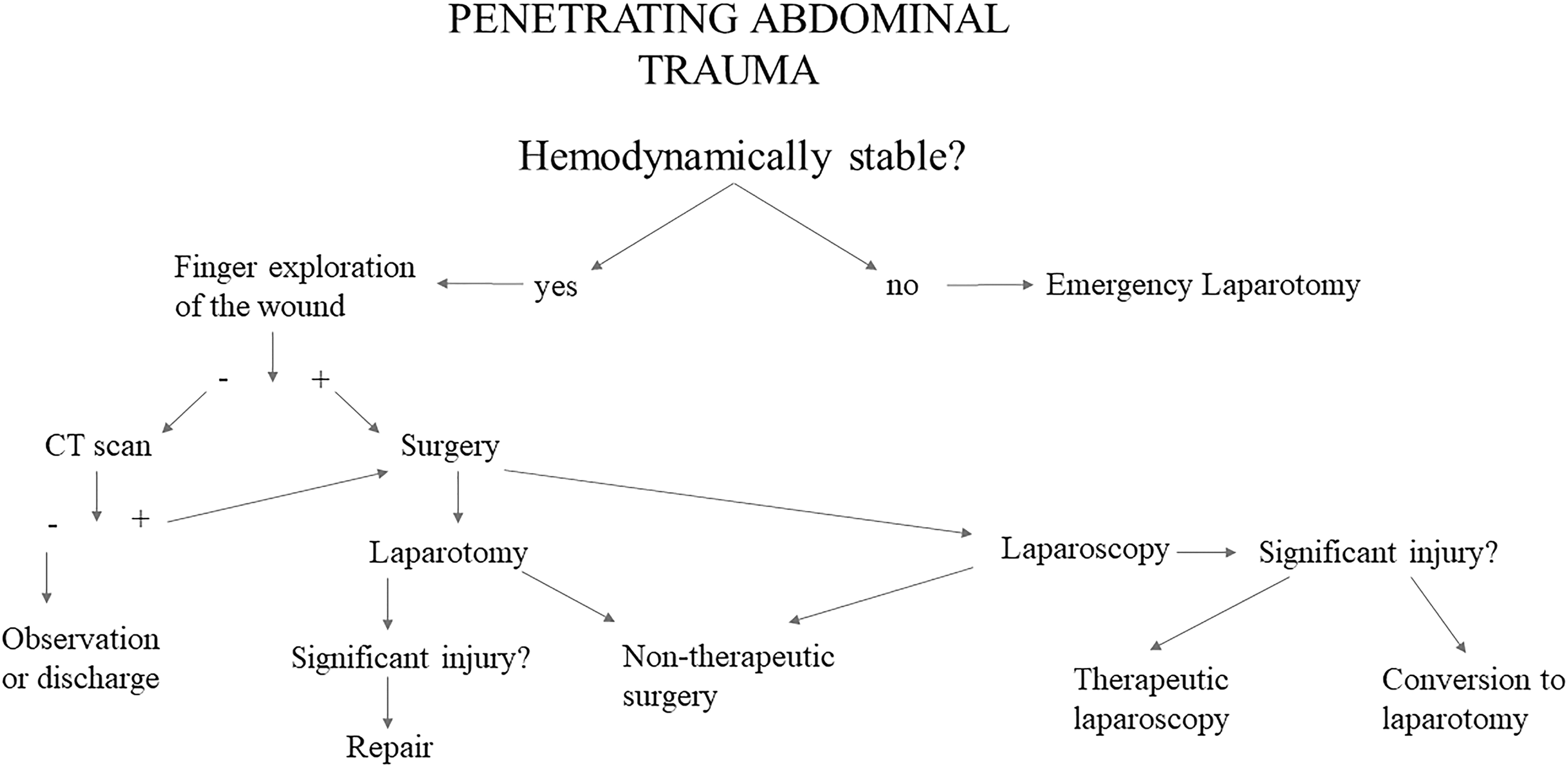
Our decisional algorithm for penetrating abdominal trauma.
In patients with PAT without evisceration, the abdominal wound was digitally explored under local anesthesia in the emergency room. In the presence of a peritoneal breach, the wound was temporarily closed to allow for insufflation, and the patients were taken for laparoscopic exploration. In the absence of a peritoneal breach, the patients were routinely sent for a contrast-enhanced computed tomography (CT) scan of the abdomen. Laparoscopic exploration was indicated when there was CT evidence of free fluid and/or a pneumoperitoneum. Those patients without pathologic CT findings were subjected to NOM, continued resuscitation, and active clinical observation for ∼24 hours.
Patients with thoracoabdominal stab wounds were assessed with plain chest radiographs and contrast-enhanced, thoracoabdominal CT scan. Patients with hemopneumothoraxes were treated with thoracostomy tube placement in the emergency room. NOM for a period of ∼24 hours ensued if there was no other indication for laparoscopic exploration.
Blunt trauma
After resuscitation, patients with BAT were routinely investigated with a contrast-enhanced CT of the abdomen and pelvis following our institutional algorithm (Fig. 2). The patients without pathologic findings on CT scan and those with low-grade solid visceral injuries were subjected to NOM, continued resuscitation, and active clinical observation for ∼24 hours. Patients were taken for exploratory laparoscopy when there was CT evidence of free fluid and/or free air and in the event of failure of NOM for solid organ injuries.
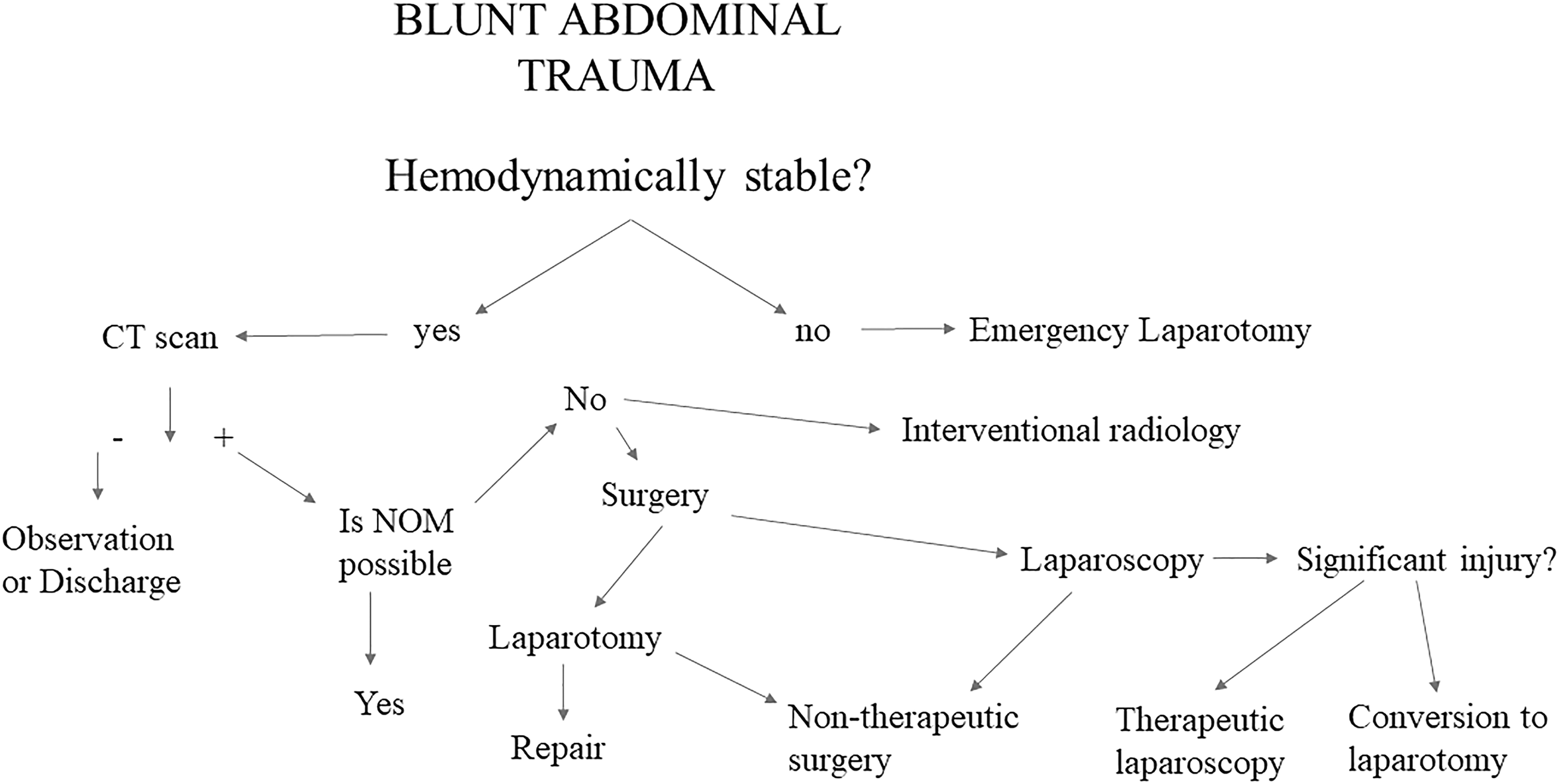
Our decisional algorithm for blunt abdominal trauma.
When patients were taken for exploratory laparoscopy, the attending surgeon was responsible for determining the positioning of the operating table and the surgical team, based on expected operative findings and CT findings. Generally, a transumbilical or paraumbilical approach was used for access, and the number and location of the working trocars were used as necessary, following the rules of triangulation during laparoscopy. A pneumoperitoneum of 14 mmHg was used, and drains were used selectively, as determined by the attending surgeon.
The following data were collected retrospectively from hospital records: patient demographics, injury mechanism, injury location, time of injury, interval between presentation and operation, details of operative findings, conversion rates, duration of hospitalization, duration of intensive care unit (ICU) stay, morbidity, and mortality. The 30-day morbidity and mortality were classified using the Dindo–Clavien classification. 15
Results
Over the 4-year study period, 26 patients presented to the emergency room with BAT or PAT and were taken to exploratory laparoscopy (Fig. 3). There was a preponderance of males (20 men, 6 women) at a median age of 37.5 years (range: 19–71).
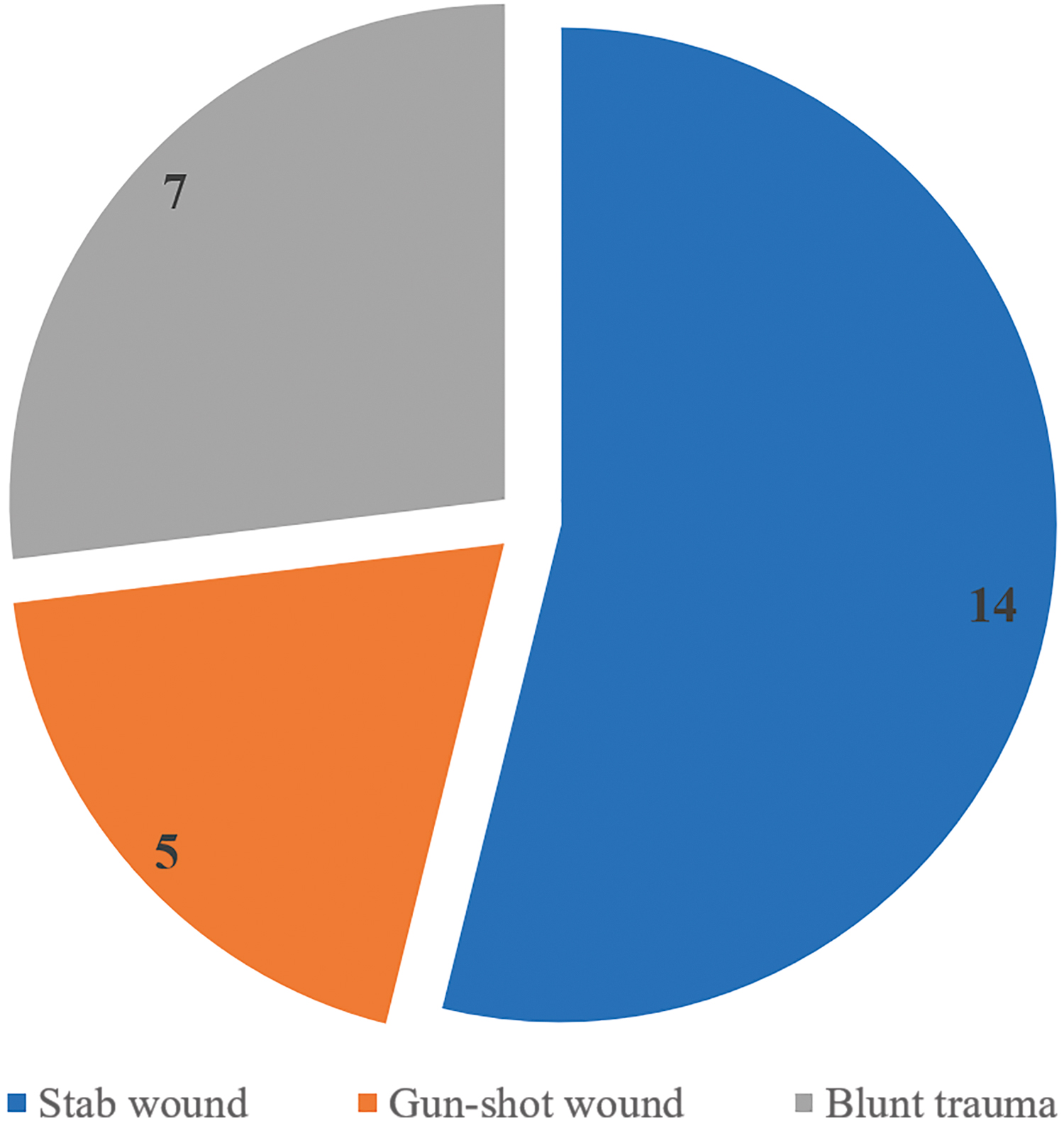
Type of abdominal trauma. Color images are available online.
Nineteen (73%) patients sustained penetrating abdominal injuries from stab wounds (14) or gunshot wounds (5). One of these patients had a minor evisceration. In this case, the viscera were reduced, and the peritoneum closed to facilitate exploratory laparoscopy. Digital exploration identified a peritoneal breach in 7 (39%) patients: 2 with gunshot wounds and 5 with stab wounds. These patients were transferred directly from the emergency room to the operation theater for exploratory laparoscopy. Eleven (58%) patients with penetrating injuries were taken for exploratory laparoscopy based on suspicious CT findings: active bleeding (4), free fluid (3), pneumoperitoneum (2), and nonspecific findings (2).
Seven (27%) patients sustained BAT and required exploratory laparoscopy due to suspicious CT findings (4), signs of peritonitis at the initial presentation (2), and development of peritonitis during a trial of NOM for blunt splenic injury (1).
Overall, 26 patients underwent exploratory laparoscopy. The median operative time for exploratory laparoscopy was 119 minutes (range: 8–300). In 5 cases, there were no intra-abdominal injuries found at laparoscopy. Therefore, the incidence of nontherapeutic laparoscopy in this series was 19%.
In the remaining cases, significant intraperitoneal injuries were encountered (Fig. 4). The patients had the following findings: small bowel lacerations (6), splenic injury (5), liver injury (5), diaphragmatic injuries (4), colonic injuries (3), gastric injuries (2), mesenteric vascular injury (1), bleeding from the round ligament (1), and pancreatic injury (1).

Injured organs. Color images are available online.
In this series, 2 (7.4%) patients underwent conversion to open surgery for development of perioperative hemodynamic instability (1) and technical difficulty with visceral obesity (1). In the other 24 patients, operative procedures were completed using the MIS approach. These included the following: small bowel resection with intracorporeal anastomosis (6), segmental colectomy with intracorporeal anastomoses (3), suture repair of gastric perforations (2), ligation of the round ligament (1), and oversewing of mesenteric vessel injuries (1). There were diaphragmatic repairs in 4 patients; 3 after stab wound and 1 after a gunshot wound. We attempted organ preservation by operative hemostasis in all patients with blunt visceral injuries, except for three patients who had laparoscopic splenectomies.
In this series, there were no deaths recorded. Seven (27%) patients experienced a complication (Table 1). There were three major complications (Dindo–Clavien ≥3) that required emergency reoperation (11%) for the following: missed small bowel laceration (1), anastomotic leak (1), and intra-abdominal collection (1). The other complications were classified as minor complications that required medical management only: surgical site infection (1), mild pancreatitis (1), and intra-abdominal collections (2).
Postoperative Complications
Requiring a reoperation.
Three (11%) patients in this series required reoperations, and all reoperative procedures were performed laparoscopically. The first patient presented with an epigastric stab wound, and was taken for laparoscopic repair of diaphragmatic injury and multiple small bowel injuries. Reoperation was required after gastrointestinal contents returned from abdominal drains and revealed a missed small bowel injury that was repaired laparoscopically. The second patient presented with BAT, and was taken for small bowel resection and primary anastomosis for a terminal ileal laceration. He required reoperation to create a terminal ileostomy after developing an anastomotic leak on the fourth postoperative day. The third patient had laparoscopic splenectomy for blunt splenic trauma. He required laparoscopic drainage of an intra-abdominal abscess on the fifth postoperative day.
The median postoperative ICU stay was 3 days (range: 1–41), and the median hospital stay was 7 days (range: 2–78). There were no readmissions in this series. However, long-term follow-up was limited because only 17 patients returned for follow-up visit after 1 month of discharge.
Discussion
In this study, we used hemodynamic stability as a prerequisite to consider laparoscopy in trauma patients. We firmly believe that this is necessary because rapid intervention is needed to stop bleeding in patients who are hemodynamically unstable. Although there are individual studies that controversially suggested the use of MIS in hemodynamically unstable patients, 16 we agree with the majority of authors in medical literature who suggest that MIS should be limited to hemodynamically stable patients only. 17 Other accepted contraindications to laparoscopy include high intracranial pressure after head trauma, 18 major thoracic trauma, 12 and a hostile abdomen with adhesions. 12
Most existing reports of laparoscopy for PAT consist of a disproportionate number of patients with stab wounds.13,19,20 This is because patients with gunshot wounds are more likely to have destructive injuries and tend to be hemodynamically unstable. This was the case in our series where only 5 patients had laparoscopy for gunshot wounds, and one of these patients required conversion to open surgery for rapid control of bleeding in the face of hemodynamic deterioration.
There are three things to consider when comparing laparoscopy versus open surgery for trauma: (1) duration of operation, (2) ability to detect injuries/incidence of missed injuries, and (3) ability to intervene when injuries are detected.
In general terms, MIS requires more operative time than open surgery. This is important to consider in the trauma patient who may quickly become hemodynamically unstable. In our study, the median total operative time was 2 hours (119 minutes), and this was comparable with reports in other studies in the medical literature.13,21,22 The longest operation in our series was in a patient who required conversion to open surgery for hemodynamic instability. Interestingly, Hajibandeh et al. 3 published a meta-analysis of one randomized study and 8 observational studies comparing MIS and open surgery for PAT and recorded a faster operation time (mean difference 27.99) with laparoscopy, although the studies analysis was statistically heterogeneous. This aspect could be associated to a laparoscopy for trauma usually performed by experienced laparoscopic surgeons, capable of rapid abdominal cavity exploration.
Laparoscopy also brings other advantages, such as the avoidance of nontherapeutic laparotomies. Historically, up to 40% of operations for penetrating trauma were reported to be negative laparotomies. 1 These negative laparotomies can be harmful for patients because they prolong the duration of hospitalization and bring attendant morbidity. 23 An advantage of MIS in patients with PAT is the ability to evaluate the presence of a peritoneal breach with 100% sensitivity and specificity.17,19,24 In our study, 19% of patients had nontherapeutic laparoscopy: 3 had no intraperitoneal injuries, 1 had a hemoperitoneum from a vessel in the abdominal wall, and one had normal intraperitoneal organs after reduction of evisceration. The 19% nontherapeutic laparotomy rate in our study is lower than the published figures for open exploration1,23 and also lower than those from early reports evaluating laparoscopic exploration. 17 Interestingly, one of our patients with a nontherapeutic laparoscopy had reduction of bowel evisceration. Some authors still consider evisceration a contraindication to MIS. 17 However, Matsevych et al. 25 reported that MIS allowed them to perform therapeutic operations in 73% of 39 patients with bowel evisceration after penetrating trauma. In our case, the patient was spared the attendant morbidity of a laparotomy incision as there was no injury detected.
A common criticism of MIS in trauma was the high rate of missed injuries in early studies. However, most recent reports have shown a dramatic improvement, with overall accuracy of diagnostic laparoscopy approaching 100% and only sporadic reports of missed injuries.17,24,26,27 In our series, there was only one (3.8%) missed small bowel injury. In retrospect, this may have been due to failure to examine the small bowel in its entirety. Therefore, we now advocate routine complete laparoscopic inspection of the entire small bowel, commencing at Treitz's angle and systematically examining caudally to the ileocecal valve.28,29
In early reports, the role of laparoscopy was limited to diagnosing intraperitoneal injuries, and many surgeons would then convert to open surgery for repair.19,30 However, many authors have since clearly demonstrated that laparoscopy can have a therapeutic role in repair of injuries and cessation of bleeding in patients with BAT and PAT.12,14,22,31–33 A variety of different traumatic injuries can be effectively managed laparoscopically. Multiple authors have reported effective laparoscopic repair of small bowel injuries,13,32,34 colonic injuries,21,34,35 and gastric injuries.14,21,34 In our study, 11 gastrointestinal injuries were repaired laparoscopically. This included primary repair of small bowel injuries (5), segmental colectomies with intracorporeal anastomoses (3), gastric repairs (2), and small bowel resection with intracorporeal anastomosis (1). There were good outcomes in these cases, with no anastomotic leaks. While we have shown that management of complex bowel injuries is feasible, it is important to appreciate that an important prerequisite is appropriate surgical training and experience.
MIS can provide great assistance to diagnose diaphragmatic injuries, especially since the diagnosis on imaging remains tenuous. 8 There are also reports of lacerations being effectively repaired laparoscopically.36,37 We identified significant lacerations in 4 patients with thoracoabdominal stab wounds in this study, and we demonstrated that diaphragmatic repairs with nonabsorbable polypropylene sutures were feasible in 100% of cases, even in complex cases with traumatic colonic herniation into the left chest.
BAT often causes liver and splenic injuries. While low-grade (I–II) injuries can be managed nonoperatively and urgent laparotomy is mandatory in case of hemodynamic instability, operative intervention is usually required for higher grade injuries, failed nonoperative/interventional radiology managements and in case where the BAT is associated with pneumoperitoneum, or there are signs of peritoneal irritation.4,21,33,38,39 When operative intervention is required for these solid visceral injuries, it is often required to address ongoing bleeding using a variety of techniques, such as application of topical hemostatic agents, cauterization, stapling, suturing, and/or packing. In extreme cases of splenic injury, splenectomy may be required. All these interventions, except the packing, can be performed laparoscopically if the appropriate tools and skill sets are available. In our study, we successfully managed 5 patients with bleeding liver lacerations and 2 with bleeding splenic lacerations using only monopolar cauterization through a laparoscopic approach. We also performed 3 laparoscopic splenectomies using clips to control the vessels instead of staplers, although 1 patient with morbid obesity required a conversion to open splenectomy. We have demonstrated, though, that these injuries can also be managed laparoscopically in the face of trauma.
In our series, there was a 7.5% conversion rate. This was comparable well with other reports in the medical literature,3,14 where conversion rates range from 2.1% to 46.8%. 3 It is important to recognize that the wide range of figures reported may be due to inherent bias since some authors considered laparoscopy only as a diagnostic tool, while therapeutic procedures mandated conversion. We do not believe that discovery of an injury should mandate conversion, and we have demonstrated that complex injuries can be managed using the laparoscopic approach. We do, however, concede that this requires significant technical skill and advanced laparoscopic experience.
In our series, we recorded 27% overall morbidity, no mortality, and 11% reoperation rate. This was comparable with other reports in recent literature.3,14,22,40 The 3-day median ICU stay and 7-day median duration of hospital stay in this series also compared well with other reports in medical literature.3,22,40,41 We believe that these results add to the existing data, demonstrating that laparoscopic exploration is feasible and effective to treat a variety of injuries in trauma patients. It also supports the use of laparoscopy for re-exploration to address complex injuries in delayed operations.
We recognize that there are inherent limitations to our report. First, this is a retrospective series with a limited number of patients that limits the statistical power of analysis. In addition, we were not able to compare open and laparoscopic surgery because only a small number of laparotomies were performed for trauma. We recognize that the study methodology introduces inherent selection bias because patients who were hemodynamically unstable were automatically selected for open surgery. Finally, there was short and inconsistent follow-up in this series, largely due to socioeconomic factors. The difficulty in long-term follow-up seems to be a consistent issue in reports on trauma patients.3,22,40 However, there is good communication between surgical centers in Belgium, and we were not made aware of any information to suggest that any patient required readmission or treatment at other centers.
Conclusions
Laparoscopy is a safe, feasible, and effective tool in the surgical armamentarium to treat hemodynamically stable patients with blunt and PAT. It allows complete and thorough evaluation of intra-abdominal viscera, reduces the incidence of nontherapeutic operations, and allows therapeutic intervention to repair a variety of injuries. However, it requires appropriate surgeon training and experience with advanced laparoscopic techniques to ensure good outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this work.