
Abstract
Background and Purpose:
Operative microwave ablation (MWA) is a safe modality for treating hepatic tumors. The aim of this study is to present our 10-year, single-center experience of operative MWA for neuroendocrine liver metastases (NLM).
Methods:
A single-institution retrospective review of patients who underwent operative MWA for NLM was performed (2008–2018). Demographics, primary tumor site, operative approach, combined surgical operations, and carcinoid symptoms were recorded. Clinical outcomes for major complications, readmission, and mortality were analyzed 30 days postoperatively. Postablation imaging was evaluated for incomplete ablation/missed lesions, and surveillance imaging reviewed for local, regional, and metastatic recurrence.
Results:
Of the 50 patients (166 targeted lesions) who received MWA for NLM, 41 (82%) were treated with a minimally invasive approach, and 22 (44%) underwent MWA concomitant with hepatectomy and/or primary tumor resection. Within the study cohort 70% of patients were treated with curative intent with a 77% (27/35) success rate. Carcinoid symptoms were reported in 40% (20/50) of patients preoperatively, and MWA treatment improved symptoms in 19/20 patients. Incomplete ablation occurred in 1/166 treated lesions. Recurrence-free survival at 1 and 5 years was 86% and 28%, respectively. Overall survival at 1 and 5 years was 94% and 70%, respectively (median follow-up 32 months, range 0–116 months).
Conclusion:
Operative MWA is a versatile modality, which can be safe and effectively performed alone or combined with hepatectomy for NLM, preferably using a minimally invasive approach, to achieve symptom control and possibly improve survival.
Introduction
The incidence of neuroendocrine tumors (NETs) has increased three- to fivefold over the past four decades. 1 Due to the indolent and often asymptomatic progression of NETs, presentation with neuroendocrine liver metastases (NLM) is common, and NLM incidence is associated with the primary NET site (<5% with appendiceal carcinoma, up to 91% for small bowel NET). 2 The presence of NLM represents the most important prognostic factor regardless of primary site, and when left untreated, 5-year survival is typically <50%.3,4
Systemic treatment[s] for NLM usually demonstrates poor disease control, making surgical resection the primary option for curative treatment. However, 60%–80% of patients with NLM present with an unresectable burden of disease due to bilobar hepatic disease and/or extrahepatic metastasis. 2 Liver-directed therapies, including trans-arterial chemo-embolization (TACE) and selective internal radiation therapy (SIRT), can cause disease regression with a survival advantage, but only 75% of lesions respond and result duration can be limited. 5 Consequently, thermal ablation (radiofrequency ablation [RFA] and microwave ablation [MWA]) has shown increasing use for treating NLM and is reported as a safe and effective modality.4,6,7
Despite several technical advantages that MWA may offer over RFA,8,9 the greater period over which RFA has been available means that the majority of reports using thermal ablation for treating NLM have used RFA.10–12 Specific to the MWA literature, NLM treatment is confined to limited institutional series or a subset of patients within larger studies of hepatic tumor ablation with MWA.13,14 As such, reports for MWA of NLM often combine both operative (laparoscopic and open) and percutaneous approaches.14,15
The aim of this study is to report our 10-year experience of operative MWA performed specifically for NLM using a predominantly minimally invasive approach. The primary outcome was overall survival (OS), and secondary outcomes included technical ablation success, carcinoid symptom improvement, and postoperative morbidity.
Methods and Materials
Institutional assurances, patient selection, and data collection
Approval for this study was obtained from the Institutional Review Board (Carolinas Medical Center). A retrospective review was performed for all patients who underwent operative MWA for NLM at our institute (January 2008 to July 2018). Patients were identified through an institutional diagnostic and billing database for MWA of NETs. For patients who underwent multiple MWA procedures, data were reported only once for the initial ablation[s]. Patient demographics, preablation tumor size/number, previous treatments, and absence/presence of carcinoid symptoms (e.g., flushing, diarrhea, sweats, and abdominal pain) were assessed pre- and postoperatively and oncologic outcomes recorded.
Patient participation and operative indications
All patients with NLM were evaluated in a multidisciplinary manner after complete clinical staging with triphasic abdominal and noncontrasted chest computed tomography (CT) or magnetic resonance imaging as necessary. In addition to standard preoperative chest/abdomen imaging to localize disease, the majority of patients underwent whole-body imaging with either somatostatin receptor scintigraphy (octreotide scan) or gallium-68 dotatate positron emission tomography (PET)/CT scan to rule out distant metastases, particularly in patients undergoing curative intent. Multimodality liver directed therapies were considered for all patients and included resection, ablation, TACE, SIRT, somatostatin analogs, and other systemic therapy as appropriate for tumor biology and stage. The use of MWA alone, or as a combined surgical treatment, was offered for multiple indications, which included patients unfit for a major hepatic resection, extensive hepatic disease burden curable with combined ablation and resection, small lesions that would otherwise necessitate a major hepatic resection, cytoreduction for potential survival benefit, and patients with severe carcinoid symptoms refractory to available medical treatments.
Operative MWA technique
All MWAs were performed under general anesthesia using a laparoscopic technique when feasible or an open technique when necessary. The majority of MWAs were performed with one of several 2.45 GHz MWA systems, with the exception of 7 patients who were treated with a 915 MHz MWA system during the first 5 years of the study. Single ablation zones were used for tumors <3 cm. Tumors >3 cm were treated with overlapping ablation zones. Intraoperative ultrasound (IOUS) was used in all cases with a laparoscopic or open probe (as appropriate) to confirm lesions from preoperative imaging, identify additional lesions, guide MWA antenna placement, avoid ablation of critical vascular structures, and confirm the ablation zone. Operative details were recorded for operative time, estimated blood loss, number/location of lesions ablated by hepatic segment, size of lesions (by maximal diameter on IOUS), ablation time/power setting, energy delivered, and use of combined procedures (if performed) concomitant with operative MWA.
Postablation surveillance
Postoperative length of stay, 30-day major complications (graded III–V using the Clavien-Dindo classification scale), and 30-day perioperative mortality were recorded. 16 Reduction or resolution of carcinoid symptoms was documented based on patient report at time of first postoperative clinic visit. For evaluation of ablation success all patients were scheduled to receive a postoperative triphasic CT scan within 4–6 weeks of surgery. Scans were scheduled every 4 months for 2 years for surveillance.
Ablation definitions and outcomes
An incomplete ablation was defined as residual arterial enhancement within or along the margin of the ablation zone on initial postablation imaging most consistent with persistent tumor. A missed lesion was defined as a new enhancing hepatic lesion on the first postablation scan not adjacent to an ablation zone and not detected preoperatively or at time of surgery. Local recurrence (LR) was defined as an enhancing lesion contiguous with the ablation zone present on subsequent surveillance imaging, which was not present on the initial postablation scan. Regional recurrence (RR) was defined as intrahepatic recurrence on subsequent imaging not adjacent to the ablation site. Metastatic recurrence (MR) was defined as extrahepatic recurrence.
Curative intent was defined as a preoperative surgical plan to treat known disease supported by visual and IOUS confirmation of treatment of all known lesions. Successful cure was assigned to patients under curative intent who had no evidence of missed lesions or incomplete ablations on the first postablation scan. Cytoreductive intent was defined as known untreated disease (intrahepatic or extrahepatic) by the conclusion of the operation. Recurrence-free survival (RFS) was evaluated only for patients with a curative outcome, whereas progression-free survival was evaluated for all patients with a cytoreductive outcome (cytoreductive intent or failed cure).
Statistical analysis
Quantitative data for patient and operative outcomes were reported for categorical and continuous variables by number with percentages or median with ranges, respectively. Survival estimates were calculated using the Kaplan–Meier method, censoring patients lost to follow-up. A P value <.05 was considered significant. Statistical analysis was performed using Stata (StataCorp, V13).
Results
Patient demographics and tumor characteristics
During the 10-year study period 50 patients with NLM were treated using operative MWA (Table 1). The most common primary NET sites were intestinal (n = 26), pancreatic (n = 13), pulmonary/mediastinal (n = 4), gastric (n = 1), and rectal (n = 1), with 5 patients having an unknown primary NET site. Overall, 25/50 patients received operative MWA as a part of their initial treatment plan for newly diagnosed neuroendocrine (NE) malignancy, often occurring in combination with hepatic and/or primary resection. The remaining 25 patients who previously underwent resection of a primary NE tumor were offered operative MWA after multidisciplinary evaluation as one component of a multimodal treatment plan for either initial treatment of newly-diagnosed NLM (n = 15) or for persistent liver metastases despite previous liver-directed therapy (n = 10).
Demographics and Neuroendocrine Tumor Characteristics
BMI, body mass index; MWA, microwave ablation; NET, neuroendocrine tumor.
Preoperatively, 31/50 patients (24/35 patients treated with curative intent and 7/15 patients treated with cytoreductive intent) underwent whole body imaging with either somatostatin receptor scintigraphy (octreotide scan) or gallium-68 dotatate PET/CT scan at our institution before MWA to rule out distant metastases. Of note, several of the “non-imaged” patients were referred to our institution for liver-directed therapy (including MWA) from oncologists outside our hospital system who reported that the patients did not have distant metastases known, but confirmatory imaging or reports were unable to be obtained to verify. In total, 1/50 patients (treated with cytoreductive intent) had bone metastases at the time of MWA, and their treatment intent was for refractory carcinoid symptoms.
Operative characteristics and outcomes
Operative characteristics and early postoperative outcomes are presented in Table 2. Curative intent was pursued in 70% of patients (n = 35), the remaining 15 patients being treated with cytoreductive intent. Of the 28 patients who underwent MWA alone 96% (n = 27) were performed with a minimally invasive approach, the only open MWA occurring within the first year of the study. The remaining 22 patients underwent operative MWA combined with hepatic resection (n = 16), primary NET resection (n = 3), or both (n = 3), of which 64% (14 of 22) of procedures were performed using an entirely minimally invasive approach (Fig. 1). Open operations were performed for combined procedures in 5 patients with major hepatic resection and 3 patients with resection of the primary NET through hemicolectomy with concurrent major hepatectomy (n = 1), sternotomy with mediastinal resection and concurrent hepatectomy (n = 1), and pancreaticoduodenectomy (n = 1). With the exception of 2 patients, the open-combined operations were performed for curative intent.
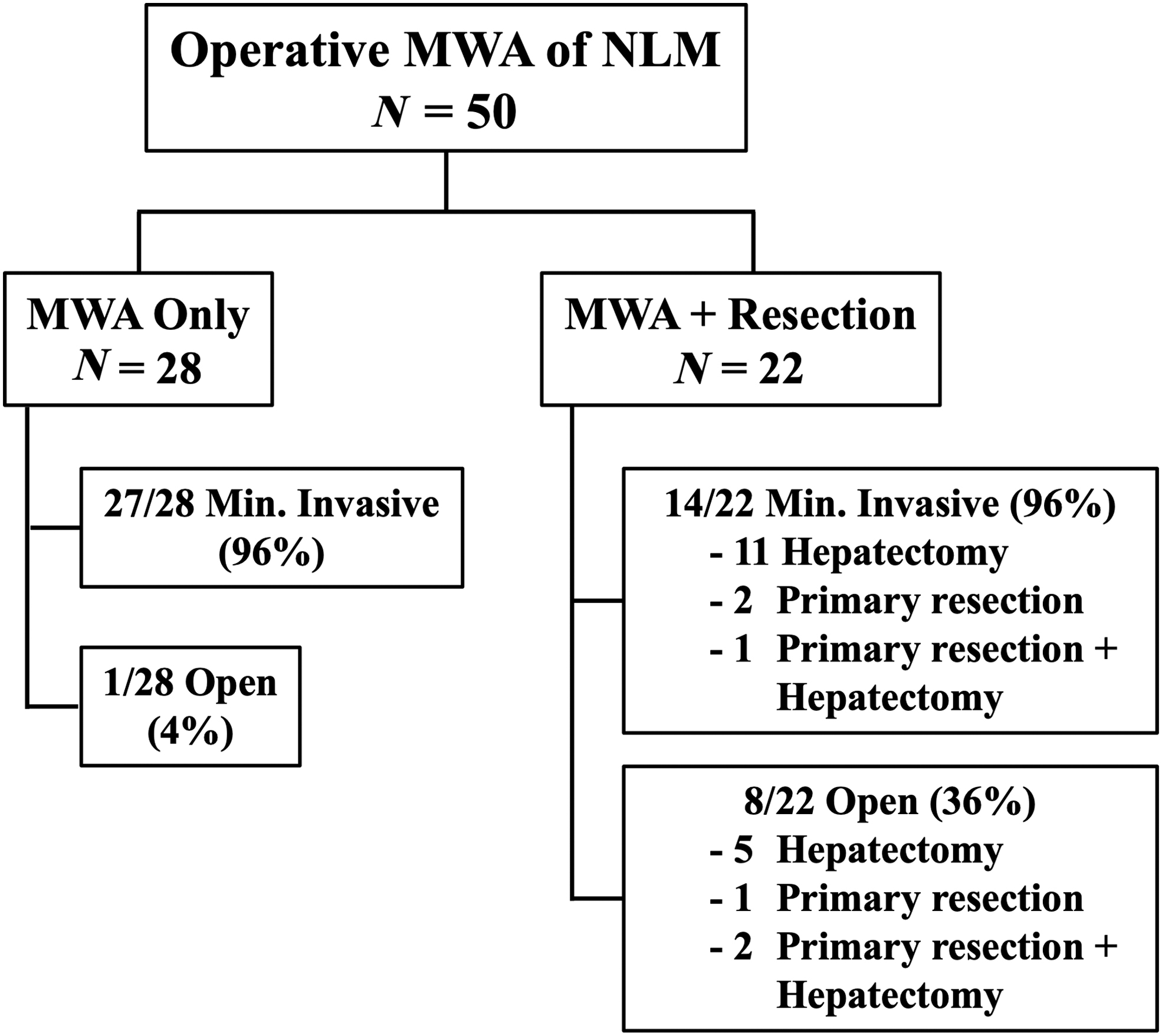
Operative approaches for MWA. MWA, microwave ablation.
Operative Characteristics and Outcomes
Includes 4 patients who had a staged hepatectomy for curative intent.
Includes 1 patient who had a staged hepatectomy following combined MWA and primary resection for curative intent.
EBL, estimated blood loss; IQR, interquartile range; LoS, length of stay; MWA, microwave ablation.
During the 30-day postoperative period, 7/50 patients required readmission and 7/50 patients experienced a major complication (Clavien-Dindo grade III–V) with 6/7 major complications occurring in patients who underwent a combined operation (Table 2). No patients required unplanned reoperation. One patient died during the 30-day period after rapidly progressive pneumonia on postoperative day 1, which progressed to respiratory failure, septic shock, and hepatic failure with death 4 days after surgery (Table 2).
Tumor and ablation characteristics
Of the 201 hepatic lesions identified during surgery 44 (22%) were not previously identified by preoperative imaging. Of the total lesions identified 35 were either surface lesions treated with local excision or tumors for which size/ablation details were not recorded and so were not included in further analysis (Table 3). Overall, 166 intrahepatic tumors were included for analysis of MWA characteristics, and distribution of hepatic lesions was even between the right (54%) and left (46%) hepatic lobes (Table 3). The median number of applications per tumor, time of ablation, and total energy delivered varied by tumor size, with longer ablation times and higher total energy delivered being evidenced at increasing tumor size (Supplementary Table S1).
Tumor Characteristics
Small surface lesions and lesions without size measurement were not included in analysis of tumor/ablation characteristics.
MWA, microwave ablation.
Ablation outcomes
Immediately following ablation, one patient was found to have an incomplete lesion ablation, resulting in an overall incomplete ablation rate of 0.6%/tumor treated with MWA (1/166) (Supplementary Table S2). Missed lesions were identified in 8/35 patients (24%) treated with curative intent.
Symptom improvement
Before MWA, 40% of patients (20/50) reported carcinoid symptoms refractory to medical therapy (Table 1). Of these patients, 19/20 reported improvement or resolution of symptoms postoperatively (Supplementary Table S2), including a 100% (10/10) rate of improvement in those patients who could not achieve successful radiographic cure from disease with cytoreductive intent (n = 6) or failed curative intent (n = 4).
Of the 21 patients on somatostatin analogs at the time of MWA, 4 patients came off these medications and 2 patients had a dose reduction. Of these patients, the duration of symptom resolution for 4 patients was at least 2–3 years before requiring resumption of medication for disease and/or symptom progression. The other 2 patients required medication resumption within a few months of cessation for control of newly diagnosed recurrent disease (not recurrent uncontrolled symptoms). However, for the majority of patients on somatostatin analogs at the time of MWA (15/21), medication was continued postoperatively by the oncologist for systemic disease control regardless of impact on symptoms, particularly for patients with cytoreductive intent. Overall symptom improvement was tracked through all patient visits with surgery or oncology until the study date or loss to follow-up (only 2 patients). Carcinoid symptoms remained improved or resolved for >1 year in 16/19 patients with preoperative symptoms, ranging from 2 to 10 years of durable symptom control (mostly depending on time from intervention to the study date).
One patient (treated with successful curative intent) had carcinoid-induced right heart disease before MWA. This patient had severe tricuspid valve regurgitation which did improve after combined hepatic resection and MWA of the other hepatic lobe for successful curative treatment of all known diseases.
Recurrence and survival
Median patient follow-up was 32 months (range 0–116 months) (Table 4). No patients were found to have LR at the ablation site. Patients with successful radiographic cure developed RR in 12 patients (44%) and MR in 7 patients (26%) (Table 4). Seven patients underwent at least one subsequent operative MWA for RR. Five patients with residual disease after initial surgery also underwent at least one additional operative MWA to treat disease progression (Table 4).
Disease Recurrence and Survival Estimates
Includes patients treated with (1) cytoreductive intent or (2) failed curative intent.
LR, local recurrence; MR, metastatic recurrence; MWA, microwave ablation; OS, overall survival; PFS, progression-free survival; RFS, recurrence-free survival; RR, regional recurrence.
During the study period, only 2 patients were lost to follow-up before 1 year after MWA. These patients were both treated with curative intent and were lost to follow-up after their 1- and 9-month follow-up visits, respectively. Ten patients died during the study period. Only one death occurred during the first 30-day postoperative period, with the remaining deaths ranging between 4 months and 10 years from the date of MWA (median 2.6 years). All surviving patients had follow-up though at the end of the study date, depending on time from intervention to the study date. OS was calculated using Kaplan–Meier analysis with appropriate censoring of patients lost to follow-up for patients with curative and cytoreductive outcomes after operative MWA was performed to determine estimated survival trends (Fig. 2). OS for patients with a curative outcome at 1 and 5 years was 96% and 70%, respectively. OS for patients with a cytoreductive outcome at 1 and 5 years was 89% and 69%, respectively. Median OS was not reached during the follow-up in this study period.
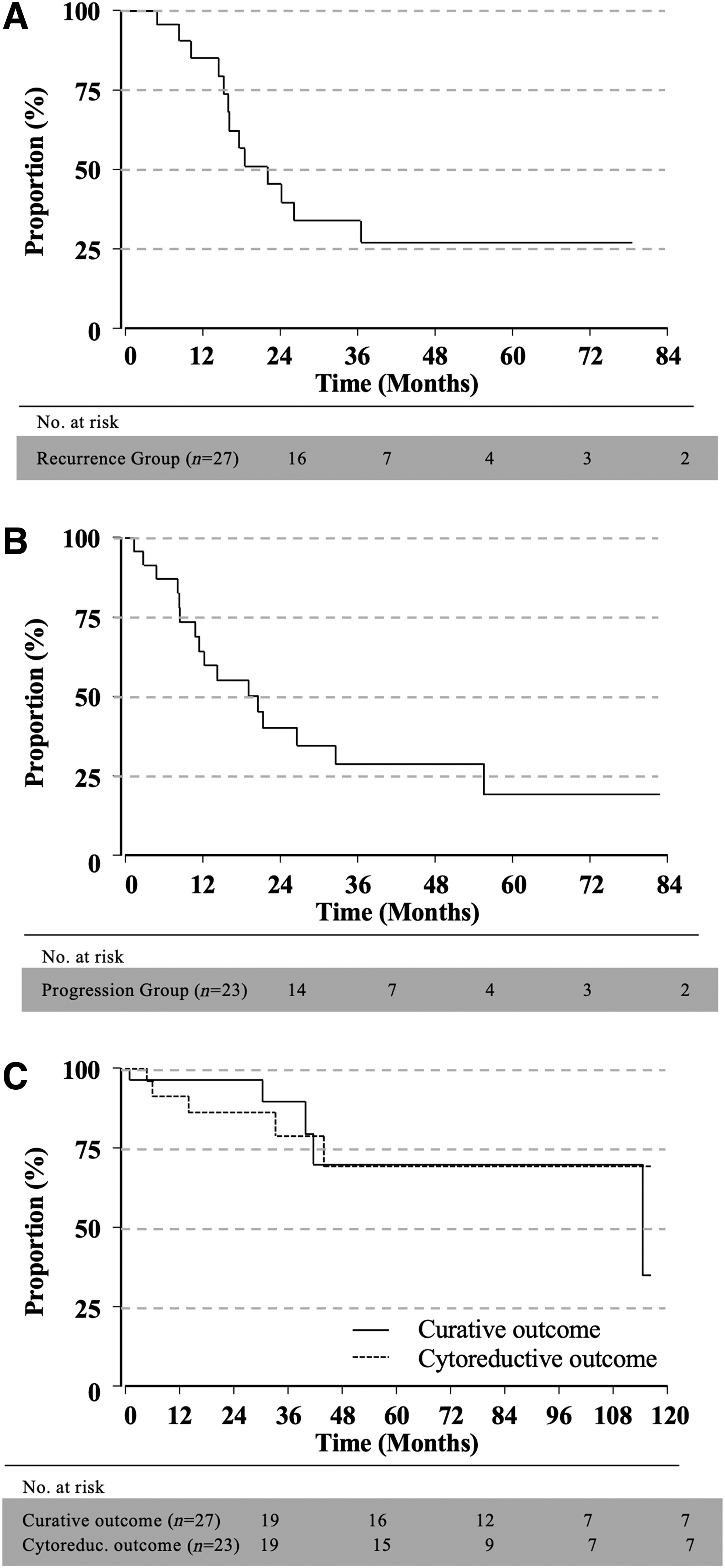
Kaplan–Meier analysis for
Discussion
Operative MWA is a versatile modality, which can be safely and effectively performed with or without concurrent liver resection, preferably using a minimally invasive approach. To the author's knowledge, this study represents the largest single-center experience with operative MWA for the treatment of NLM. Overall, MWA with IOUS guidance was successful with a low rate of incomplete ablation and no LR at the ablation site. Curative intent was successful in 77% of patients and was associated with substantial overall and RFS. The majority of patients was successfully treated with a completely minimally invasive approach, whether by MWA alone (96%) or combined with resection (64%) to achieve disease cure or adequate debulking. Operative MWA also effectively facilitated improvement or resolution of carcinoid symptoms in patients treated with curative (93%) and cytoreductive intent (100%).
Curative hepatic resection is well reported as a first option for the majority of patients with NLM with the best OS reported for limited disease amenable to surgical resection alone (70%–90% at 5 years), despite overall high recurrence.17,18 However, due to the inherently indolent progression of disease, 60%–80% of patients with NLM present with extensive intrahepatic or extrahepatic disease burden, which precludes cure by resection alone.2,19,20 Multiple adjunctive liver-directed and lesion-directed therapies have been used in the pursuit of disease cure and control for NLM, including increased use of thermal ablation. 21 To date the role operative of MWA in curative and cytoreductive treatment approaches is unclear as a result of variability in ablative technologies/approaches, the concurrent use of MWA with resection, and the timing of MWA use with other locoregional therapies. 2
In contrast to curative treatments for NLM, the role of cytoreductive (debulking) interventions for patients with uncurable disease burden has been controversial, although mounting data suggest that cytoreduction may provide survival benefit.22,23 Cytoreduction is more clearly defined for patients experiencing severe carcinoid symptoms since it provides substantial relief in addition to survival benefit. 24 Of note, a potential survival benefit has also been suggested (even for asymptomatic patients) when at least 80%–90% of debulking is achieved.25,26 Recent efforts, including a large multi-institutional analysis by Ejaz et al., have begun to identify patients who are most likely to benefit from cytoreduction. 26 However, the potential for operative MWA to serve as treatment option to achieve adequate cytoreduction remains undefined.
Independent of treatment intent, technical success of operative MWA begins with evaluation of the ability to achieve complete ablation (assessed on the first postablation imaging). 27 In our study rate of incomplete ablation was 0.6% per lesion, which is lower than the 4.5% incomplete ablation rate for NLM in the largest multi-institutional series of operative MWA. 14 Of note, Takahashi et al. reported on laparoscopic MWA of 301 lesions that included 115 NLM with no incomplete ablations, although postablation imaging was only performed 1–2 weeks postoperatively. 13 Comparison alongside operative RFA is limited as both incomplete ablations and LR have been frequently reported as a combined outcome of 6.3%–7.9% of lesions for NLM.28–31 However, LR can be reflective of both technical success and tumor biology and should be evaluated separately from incomplete ablation. 27 In comparison, LR has been reported for 3%–11% of NLM patients in multi-institutional studies for MWA and as low as 0% in two of the largest single center series to date.13,14,32,33 No patients developed LR in this study, although it should be noted that loss to follow-up and indolent disease course may contribute to limit detection.
Several technical advantages of operative MWA for NLM are also highlighted in our study. Operative MWA should be performed through a minimally invasive approach whenever possible. In addition, laparoscopic MWA can be effectively combined with minimally invasive hepatic resection in many patients with complex/multifocal disease to expand the opportunity for both curative and cytoreductive treatment. To date, incorporation of operative MWA in studies as a modality for surgical cure alongside resection for NLM has only been reported in a few studies. 17 MWA performed through an operative approach also allows for multimodal detection and treatment of metastatic disease, utilizing laparoscopic IOUS for all minimally invasive MWA. In our series 22% of lesions were newly detected, which is similar (although slightly higher) than rates previously reported for operative MWA.14,28,34
NETs also have a predilection for peritoneal spread, which may be occult on preoperative CT imaging. For example, in a national survey in the Netherlands, Madani et al. reported that 19% of metastatic NE tumors had peritoneal disease. 35 Consequently, a laparoscopic approach may improve clearance of tumor burden in patients pursuing curative intent and may help achieve the >90% debulking needed for adequate cytoreduction. 26 Operative MWA also allows for mobilization of the liver away from critical structures and is typically feasible through a laparoscopic approach. Laparoscopic visualization and hepatic mobilization may also facilitate ablation of lesions otherwise difficult to access such as posterior lesions (segments VI–VIII) that otherwise may require a transthoracic approach when performed percutaneously, an approach that is associated with a significant risk of incomplete ablation and/or serious complications.36,37
Whether for curative or cytoreductive intent, operative MWA achieved excellent carcinoid symptom control and a favorable potential survival impact in this patient series. Symptom improvement or resolution was consistent with the >95% symptom control previously reported for MWA. 30 While nonlocal disease recurrence in those who achieve curative treatment was expectedly common, operative MWA achieved a median RFS of nearly 20 months with 85% radiographically disease free at 12 months, which is similar to the median RFS of 24–33 months reported in contemporary studies of MWA for NLM.14,32,33 The potential impact of operative MWA on OS was supported in patients who achieve successful cure (1 year 96%; 5 years 70%), as well as for cytoreduction (89% and 69%, respectively). Although comparative OS data are sparsely reported for institutional operative MWA studies, the largest multi-institutional series has reported a 5-year OS of 54% with median OS of 92 months. 14
Several inherent limitations should be considered for this single-institution review, including potential patient selection bias, variability within ablation instruments/techniques used, indications for hepatic resection versus ablation, and locoregional and systemic therapies. Consequently, direct causation for oncologic outcomes in this study cannot be independently associated with operative MWA. Survival outcomes could also be impacted by repeated ablations for recurrence, additional liver-directed therapies, and systemic treatment following MWA. Pancreatic NETs are known to have worse survival than other primary sites with NLM; however, these were not evaluated separately in this study because of the limited number of patients. Median follow-up was <3 years, limiting long-term analysis. Loss to long-term follow-up occurred, in part, since many patients were referred from community oncology practices for liver-directed interventions and then returned for long-term oncologic follow-up to their community oncologists, which do not have shared electronic medical records.
Conclusions
Operative MWA is a versatile modality, which can be safe and effectively performed alone or combined with hepatectomy for NLM to achieve substantial symptom control and survival improvement, preferably through a minimally invasive approach. To fully evaluate the efficacy of MWA in the treatment of NLM, a multi-institutional trial in which outcomes for MWA are compared with other surgical approaches is necessary.
Footnotes
Acknowledgments
The authors acknowledge Allyson Cochran for assistance with statistical support and Gerri Chadwick and Jill Jurgensen for assistance with revising/editing the article.
Disclosure Statement
No competing financial interests exist.
Funding Information
No external funding was received to support this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.