
Abstract
Aim:
To assess the impact of the laparoscopic anatomic resections (LARs) on hepatocellular carcinoma (HCC) patients, analyzing the pooled short- and long-term outcomes of this technique and comparing it with the standard open approach [open anatomic resections (OAR)].
Material and Methods:
A systematic literature search was performed in PubMed, Embase, and Scopus for studies published between 2010 and 2020 concerning LAR for HCC.
Results:
After screening 311 articles, 10 studies with a total of 398 patients who underwent LAR for HCC were included. The pooled cohort included mostly male (76.6%), Child A (98.2%), with hepatitis B virus (HBV)-related disease (60.5%). The pooled conversion rate was 7.3%. The pooled overall complication rate was 10.2 with a mortality rate of 1.0%. In the pooled analyses of only comparative studies, LAR group included 378 versus 455 in OAR. Operative time was longer in the LAR group (329 minutes versus 248; P = .001). Blood loss (179 versus 331 mL; P = .018) was lower in the LAR group. The pooled mean length of hospital stay was 8.4 days in LARs and 11.3 in OARs (P = .002). The pooled rate of postoperative complications was higher in the OAR group (25.3 versus 13.8; P = .009), while mortality rates were similar. The LAR group had a pooled 3- and 5-year overall survival of 90.1 and 81.9 versus 83.5 and 80.7 of the OARs (P > .05), respectively.
Conclusions:
In conclusion, the LAR for HCC is safe and associated with decreased blood loss and length of hospital stay. Survival rates are comparable with those of the conventional open approach.
Introduction
Anatomic liver resection is the preferred surgical procedure for hepatocellular carcinoma (HCC) as this has been demonstrated to be associated with longer survivals than nonanatomic resections.1,2
For the last decade, the laparoscopic approach has been gaining consent among surgeons for the treatment of HCC. However, the laparoscopic anatomic resection (LAR) may be extremely challenging in this subset of patients usually characterized by an underlying liver disease, which add further complexity to the procedure. Several studies successfully demonstrated the safety of the laparoscopic approach when compared to the conventional open approach.3–16 Still, most of them included heterogeneous cohorts in terms of type of resection (e.g., anatomic/nonanatomic) making results about LARs difficult to be interpreted.3,8–10,13,14
This first systematic review, including the series reporting data on LAR, aims to assess the impact of the LARs on HCC patients, analyzing the pooled short- and long-term outcomes of this technique and comparing it with the standard open approach.
Material and Methods
Study selection
This study adhered to the 2010 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 17 A systematic literature search was performed in PubMed, Embase, and Scopus for studies published between January 1, 2010 and June 10, 2020. Search terms used were (((((((((“laparoscopes”[MeSH Terms] OR “laparoscopes”[All Fields]) OR “laparoscope”[All Fields]) OR “laparoscopical”[All Fields]) OR “laparoscopically”[All Fields]) OR “laparoscopics”[All Fields]) OR “laparoscopy”[MeSH Terms]) OR “laparoscopy”[All Fields]) OR “laparoscopic”[All Fields]) AND “anatomic*”[All Fields]) AND ((((“hepatectomy”[MeSH Terms] OR “hepatectomy”[All Fields]) OR (“liver”[All Fields] AND “resection”[All Fields])) OR “liver resection”[All Fields]) AND (((“carcinoma, hepatocellular”[MeSH Terms] OR (“carcinoma”[All Fields] AND “hepatocellular”[All Fields])) OR “hepatocellular carcinoma”[All Fields]) OR (“hepatocellular”[All Fields] AND “carcinoma”[All Fields]))). Titles, abstracts, and, if required, full-text articles were screened and selected by two authors (L.S. and A.B.) independently based on inclusion criteria. Disagreement on eligibility was addressed by discussion until consensus was obtained. When additional methodological clarifications were needed, authors were contacted via email.
Inclusion criteria
Studies in English concerning anatomic laparoscopic liver resection in the scenario of the HCC that could be retrieved as full-text were included.
For institutions reporting overlapping data, the most recent series or studies with a comparative design (laparoscopic versus open) were preferred. Excluded were abstracts, editorials, reviews, case report, studies on <10 laparoscopic resection, and studies in which no sufficient data on the selected population (anatomic resection in HCC) could be extracted.
Methodological quality
The Newcastle-Ottawa Scale 18 was used to assess the methodological quality by two authors (L.S. and A.B.). This scale designed for cohort studies assesses the methodological quality rating the quality of selection, comparability, and outcome of study participants. In case series, the maximum score was six points as comparability or selection of the controls were not present. High scores indicated a low risk.
Data extraction
Data extracted included study characteristics (study period, date of publication, study design, sample size), patients' characteristics (age, sex, Child score, underlying liver disease, tumor size), and operative (blood loss, blood transfusion, operative time, conversion to open surgery and resection margins) and postoperative outcomes (overall complications, specific surgical complications, and surgical complications according to the Clavien–Dindo grade 19 ).
The 3- and 5-year survival and disease-free survival rate were the primary outcomes. They were extracted from the Kaplan–Meier curves in those cases, in which they were not explicitly reported by the authors.
Statistical analysis
For categorical variables (including survival rates), the weighted pooled rates with 95% confidence intervals (95% CIs) were obtained by the Freeman–Tukey transformation. 20 Survival was expressed as pooled 3- and 5-year survival rates and its comparison according to the surgical approach was performed calculating the relative risk (RR) of death at the time point. The inverse variance method was used to pool continuous variables in weighted means and 95% CI. Continuous variables, which were presented as median and range (or median and interquartile range) in the included studies, were transformed in mean and standard deviation as suggested by Hozo et al. 21 Heterogeneity among the included studies was verified by inconsistency (I 2 ) statistics 22 and, if present, the random effects model was used. I2 values of <25% were interpreted as low heterogeneity and above 75% as considerable. MedCalc Statistical Software version 15.8 (MedCalc Software bvba, Ostend, Belgium) was used for the statistical analysis.
Results
Literature search
The literature search yielded a total of 311 potentially relevant articles. After excluding 188 articles based on titles and abstracts, the remaining 30 full-text articles were screened based on the inclusion criteria (Fig. 1).
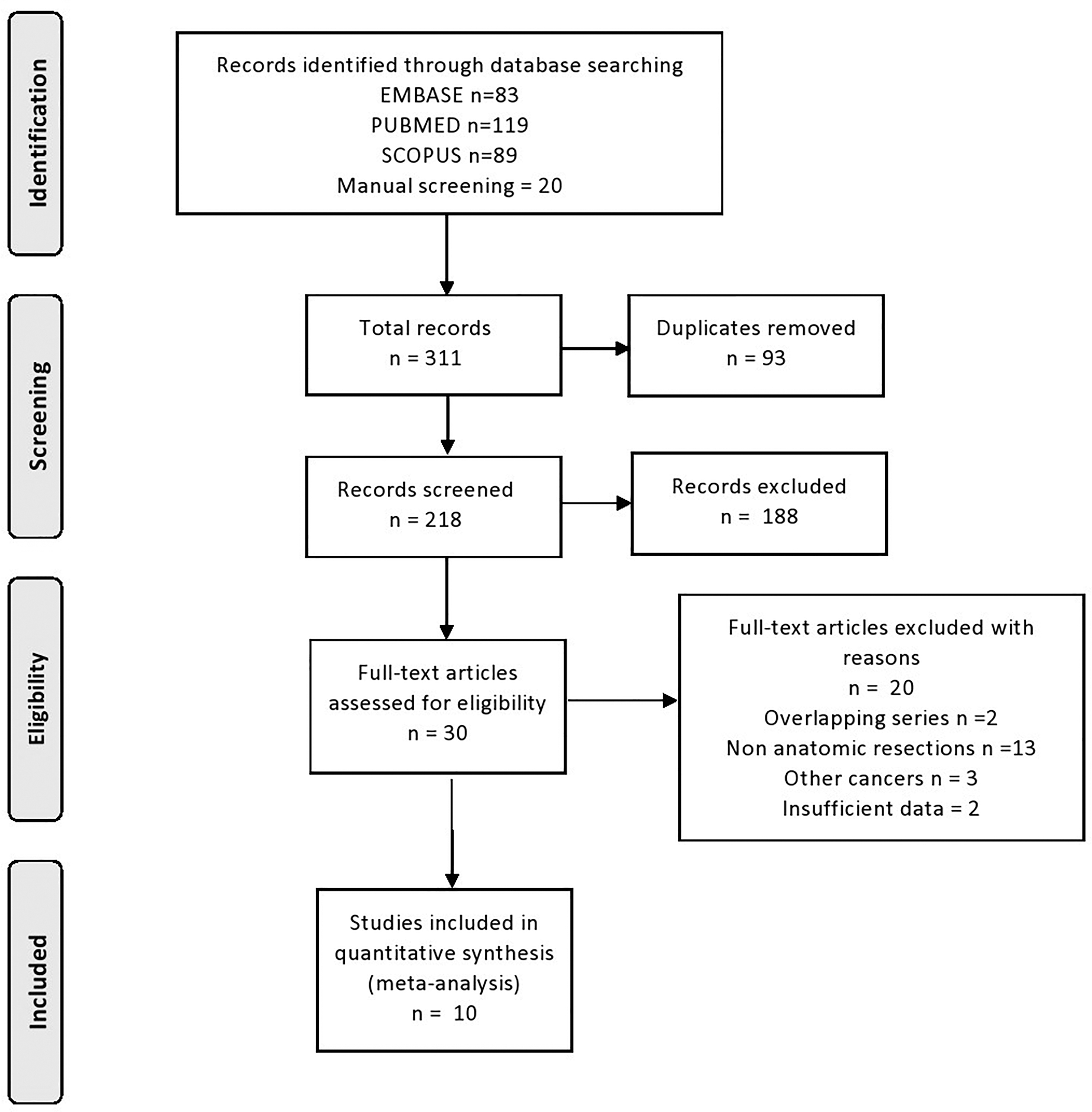
Flowchart of the selection process.
Ten studies,4–7,11,12,15,16,23,24 describing a total of 398 patients who underwent LAR for HCC were included.
Methodological quality and characteristics of the studies
The scores concerning the methodological quality of the included studies are reported in Table 1. Studies were rated with scores of 3–6 out of 7 for case series23,24 and 6–8 points out of 9 for comparative studies,4–7,11,12,15,16 which depicted a relatively low risk of bias (Table 1). All studies had a retrospective design.
Characteristics of the Included Studies
Study characteristics are shown in Table 1. Eight studies compared the laparoscopic approach with the open.4–7,11,12,15,16 Two studies were case series.23,24
Laparoscopic anatomic resections
The pooled cohort included 398 LARs. Patients' characteristics and perioperative variables are shown in Table 2. The pooled cohort included mostly male (76.6%), Child A (98.2%), with hepatitis B virus (HBV)-related disease (60.5%). The pooled conversion rate was 7.3% (0.6–19.9). The pooled overall complication rate was 10.2% (4.8–17.4) with a mortality rate of 1.0% (0.2–2.9). Among the included variables only sex, Child–Pugh score, blood transfusion, resection margins, mortality, Clavien–Dindo complications >2, bile leak, pulmonary infections, and 3- and 5-year survival had heterogeneity >0.05. The pooled 3- and 5-year overall survivals were 85.1% (78.1–90.3) and 72.8% (61.6–82.8), respectively. The 3-year disease-free survival was 65.4 (35.2–89.9).
Pooled Analyses of the Anatomic Laparoscopic Resections in the Included Studies
95% CI, 95% confidence interval; HBV, hepatitis B virus; HCV, hepatitis C virus.
Laparoscopic versus open anatomic resections
The two groups included 374 laparoscopic versus 455 open anatomic resections, respectively.
The pooled analyses of the studies comparing LAR and open anatomic resections (OAR) are presented in Table 3.
Pooled Analyses of Laparoscopic Versus Open Anatomic Resections
In Yoon et al. 15 only the propensity score-matched cohort was considered in the pooled comparative analysis.
95% CI, 95% confidence interval; HBV, hepatitis B virus; HCV, hepatitis C virus; LAR, laparoscopic anatomic resection; n.a., not applicable.
Pooled patients' preoperative characteristics were similar in the two groups. Tumor size was higher in the open group (4.4, 2.6–6.2 versus 5.0, 3.8–6.2; P = .006). Operative time was longer in the LAR group (329 minutes, 248–411 versus 248, 213–284; P = .001). Blood loss was decreased in the LAR group (179, 168–189 versus 331 mL, 198–465; P = .018). The pooled mean length of hospital stay was 8.4 days (7.2–9.6) in LARs and 11.3 (10.1–12.5) in OARs (P = .002). The pooled rate of postoperative complications was higher in the OAR group (25.3, 13.7–39.1 versus 13.8, 6.9–22.6; P = .009), while mortality rates were similar.
The laparoscopic group had a pooled 3- and 5-year overall survival of 90.1 (85.5–93.6) and 81.9 (63.3–94.9) versus 83.5 (71.7–92.6) and 80.7 (55.3–96.9) of the open group (RR 3-year 1.1, 0.99–1.14; P = .058—RR 5-year 0.99, 0.9–1.1; P = .872), respectively.
The RR of developing recurrence at 3 years after LAR was 0.99 (0.9–1.3, P = .965).
Discussion
LAR is safe with survivals comparable with those of the conventional open approach.
Several studies found that the anatomic resection is associated with improved survivals than nonanatomic resection.2,25,26 Moris et al. 2 meta-analyzed in their systematic review the results from 43 comparative studies for a total of 12,429 patients with HCC: the authors found that anatomic resections could offer a decreased risk of recurrence at 1, 3, and 5 years and of death at 5 years when compared with nonanatomic resection.
These results would suggest that HCC should always been resected with an anatomic resection, including tumor-bearing portal tributaries as well as major branch of the portal vein and hepatic artery whenever liver function is adequate for the required hepatectomy. This may be extremely challenging with the laparoscopic approach. However, our pooled analysis found acceptable complication rates (10.2%) with 5.0% of major complications comparable with those of current benchmarks for laparoscopic liver resections. 27 Lower rates in terms of overall complications were found when the laparoscopic approach was compared with the conventional open approach suggesting that laparoscopy can be performed safely also when an anatomic resection is required. Still, it must be highlighted that in the comparative pooled analyses, the open group had larger tumors and this parameter should be taken into account when interpreting the outcomes.
The laparoscopic approach seemed to be also associated with a decreased blood loss and need of blood transfusions. This is consistent with what has already been reported by Wang et al. 28 in their pooled comparative analyses of major liver resections for HCC. This may be due to two factors. First, these advantages may have been influenced by the technology used during the minimally invasive procedures and better magnification improving dissection. Second, it must be considered that the included series were all retrospective and it might have occurred that most of the open resections were performed at the beginning of the study period and they might have not benefited from the most advanced technology.
Recently, a few innovations have been introduced to improve the outcomes during laparoscopic liver resections.29,30 Berardi et al. 29 reported interesting results about parenchymal sparing anatomic resection in a series of colorectal liver metastasis and HCC: the authors exploited Indocyanine Green (ICG) Dye negative staining and three-dimensional preoperative reconstructions to achieve the most limited anatomic resection according to tumor location and size and, in their series of 86 patients, they reported 0% of 90-day mortality with 8.1% of overall morbidity. These outcomes are extremely promising suggesting that the advances in technology will keep supporting the surgeon in expanding the indications for minimally invasive surgery also in complex procedures. In this context, robotic surgery may offer additional advantages during anatomic liver resection representing a further minimally invasive option for the surgeon. 31
Our pooled analysis showed a markedly prolonged operative time in the LAR group. This may be again linked to the retrospective nature of the included studies and to the fact that none of them reported details about the effect that the learning curve could have had on outcomes.
This systematic review has a few limitations. First, it included only retrospective analyses and, therefore, it carries all the biases linked to their nature. Second, all but one 7 study was from Asian experiences and therefore patients' characteristics were mainly representative of a certain geographic area with HCC patients having usually HBV-related disease and low body mass index. Finally, due to the limited number of available studies, we could not perform a subanalysis on major and minor resections, which could have helped in identifying the role of laparoscopy in the different subsettings.
In conclusion, the LAR for HCC is safe and associated with decreased blood loss and length of hospital stay. Survival rates are comparable with those of the standard conventional approach. Further large prospective studies are required to confirm the role of the minimally invasive approach for anatomic resection in HCC western patients.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.