
Abstract
Background:
Remnant gastric cancer (RGC) is increasing due to past use of subtotal gastrectomy to treat benign diseases, improvements in the detection of gastric cancer, and increased survival rates after gastrectomy for gastric cancer. Laparoscopic access provides the advantages and benefits of minimally invasive surgery. However, laparoscopic completion total gastrectomy (LCTG) for RGC is technically demanding, even for experienced surgeons. Because of its rarity and heterogeneity, no standard surgical strategy has been established and few surgeons will develop technical expertise to carry out this procedure.
Aim:
To describe our standard technique, giving surgeons a head start in LCTG and report the early experience with this stepwise approach.
Materials and Methods:
We detail all the steps involved in the procedure, including trocar placement and surgical description.
Results:
Between 2009 and 2019, a total of 8 patients with past history of RGC were operated with this technique. All patients had been previously operated by open method, 7 due to peptic ulcer disease and 1 due to gastric cancer. Their mean age at the time of the first surgery was 38.9 years (range 25–56 years) and the mean interval between the first and the second gastrectomy was 32.1 years (range 13.6–49). Billroth II was the previous reconstruction in all cases. A 5-trocar technique was used followed by total gastrectomy with side-to-side stapled intracorporeal esophagojejunostomy anastomosis and Roux-en-Y reconstruction. The mean operation time was 272 minutes (range 180–330) and median blood loss was 247 mL (range 50–500). There was no conversion and no major intraoperative complication. Major postoperative complications occurred in 3 patients.
Conclusion:
Completion total gastrectomy for RGC is a morbid procedure and laparoscopic access is technically feasible, hopefully carrying the benefits of faster recovery, reduced postoperative pain, and wound complications. By standardizing the approach, the learning curve may be shortened and better results achieved.
Introduction
Remnant Gastric Cancer (RGC) is defined as gastric cancer arising in the remnant stomach after partial gastrectomy for benign or malignant disease. 1 It was first described by Balfour in 1922, 2 and it is associated with several mechanisms as enterogastric reflux of bile acids, hypo- or achlorhydria with subsequent bacterial overgrowth and the effect of Helicobacter pylori. 3
A meta-analysis published in 2020 with 74,952 patients indicated that the pooled prevalence of RGC was 2.6% in patients with previous gastrectomy. 4
Several studies reported an increase in the incidence of RGC due to past use of subtotal gastrectomy to treat benign diseases, improvements in the detection of gastric cancer with more frequent use of endoscopy, and increased survival rates after subtotal gastrectomy for gastric cancer.3,5,6
Surgery remains as the main curative treatment option, and gastrectomy combined with adequate lymph node dissection is considered the standard surgical treatment for resectable gastric cancer (RGC included).
Laparoscopic completion total gastrectomy (LCTG) for RGC was first reported by Yamada et al. in 2005. 7 It is more challenging than that for primary gastric cancer due to adhesions to adjacent organs, anatomical changes around the stomach caused by the initial surgery, and changes in the lymphatic flow. 8
Until now studies have demonstrated that LCTG for RGC is technically demanding, but feasible and may lead to similar oncological results compared with the open method, but with better short-term outcomes. 9 Nevertheless, the procedure is remarkably difficult, even for those with extensive experience in both gastric cancer (GC) and laparoscopy, and articles detailing the technical aspects of the approach are lacking.
In this study, we present our stepwise approach to share ideas on how to approach RGC and help give surgeons a head start to perform LCTG.
Materials and Methods
Materials
One 12 mm disposable trocar
One 10 mm trocar
Three 5 mm trocars
One harmonic or Ligasure scalpel.
Positioning and trocar placement
The patient is placed in a supine position, in the reverse Trendelenburg position, with legs abducted. The surgeon stays between the legs and surgical assistants by the patient's side.
A 5-trocar technique is used, with work trocars placed as presented in Figure 1. The first 10 mm trocar is placed supraumbilically by the open method and a 12-mmHg pneumoperitoneum is established. The other four trocars are placed as follows: 12 mm trocar in the left lateral abdomen and 5 mm trocars in the epigastric area, right lateral abdomen, and left upper quadrant.

Trocar placement for LCTG procedure. LCTG, laparoscopic completion total gastrectomy.
Procedure
The procedure starts with a meticulous inspection of the abdominal cavity.
Adhesions are common, so the surgeon should carefully free all the adhesions to identify the structures and comprehend anatomy.
As seen in the Supplementary Video S1, we start by evaluating resectability. The gastrohepatic ligament is opened toward the hiatus, the right and left crus of the diaphragm are dissected and the gastroesophageal junction mobilized. Esophageal frozen sections are obtained at this moment if judged necessary.
Next, dissection is performed around the anastomosis. The enteric loop is separated from the transverse colon and the remnant omentum removed en bloc with the specimen. The afferent loop is dissected and divided. It is then lifted and freed from the transverse colon until the posterior face of the remaining stomach is identified. If the loop was brought to the upper abdomen through the mesocolon, this is hardened and care must be taken to preserve the colonic irrigation. Dissection progresses until the efferent limb is sectioned. The jejunum is always sectioned with an adequate margin from the anastomosis and its mesentery removed accordingly.
We recommend preoperative injection of indocyanine green (ICG) in the submucosa the day before the procedure. It is performed by endoscopy, and 0.1 mL are infused in each of the four quadrants around the tumor. It helps identify the proximal margin of the tumor, and the lymphatic drainage (it may lead to more broad resection of the jejunum mesentery).
Dissection proceeds along the greater curvature, the left gastroepiploic vessels, short gastric vessels, and gastrosplenic ligament are all divided, and all left side of the remnant stomach is exposed.
The dissection is continued clockwise by freeing the transverse colon and the pancreatic body, exposing the splenic artery. Lymph node station 11p is removed and, if present, 8a as well. Station 12a is not usually removed, since lymphatic drainage of the gastric remnant rarely goes to the hepatic hilum. Perioperative ICG injection helps identifying these particular cases.
The right crus of the diaphragm is exposed caudally and station 9 is removed. The celiac trunk is exposed and the left gastric vessels ligated and sectioned. This clears lymph node station 7.
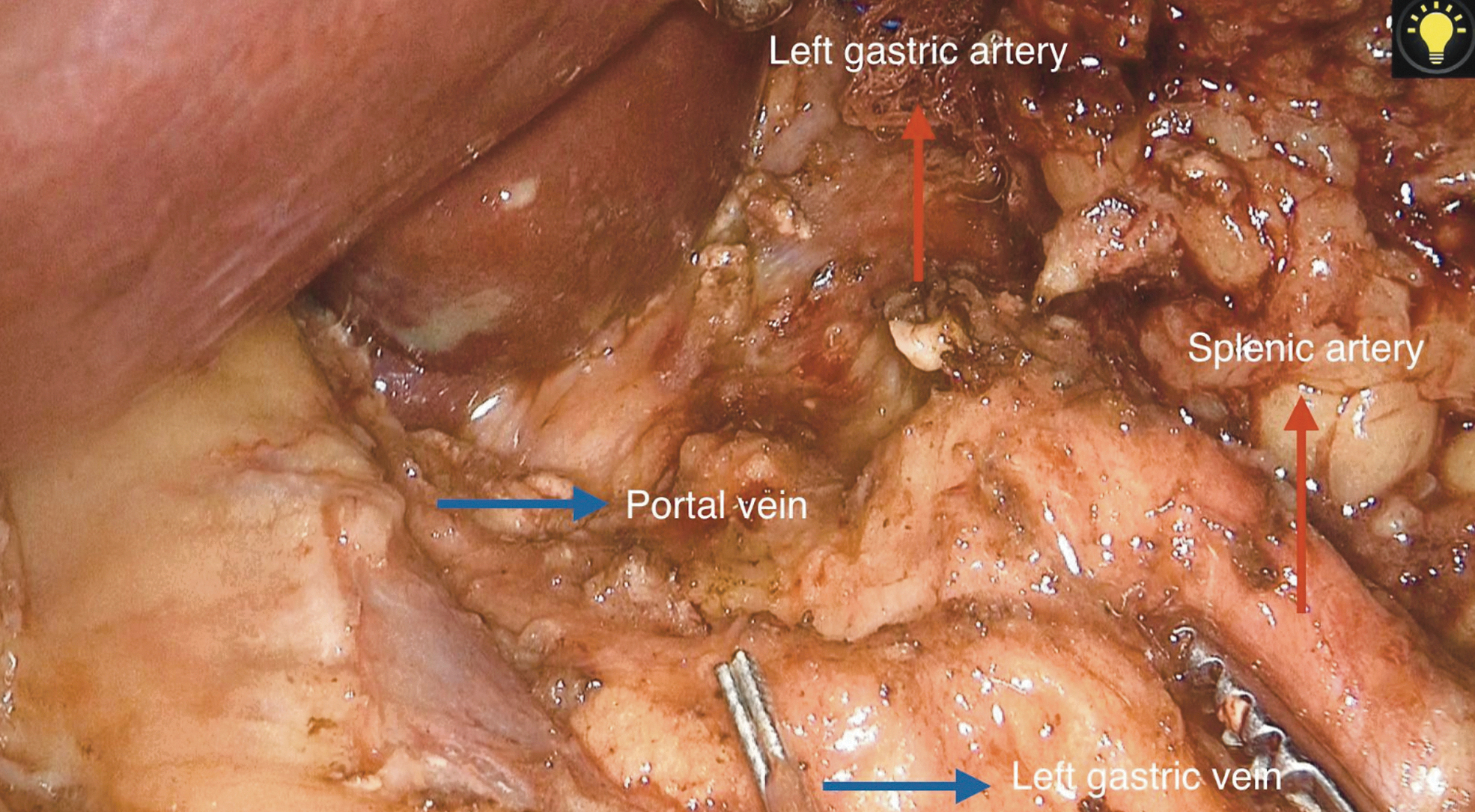
Anatomical variations may be present. The Supplementary Video S1 presents a case with absence of the common hepatic artery. In this situation the portal vein and the celiac trunk are exposed ensuring that any lymph node located in this area is removed (Fig. 2). A more frequent variation is the presence of an accessory left hepatic artery, branching from the left gastric artery. In this last situation, the vessel is skeletonized, dividing only the gastric branches.
The dissection plane along the right crus is found and the remnant stomach is completely mobilized.
After complete mobilization of the remnant stomach, reconstruction is performed. Our preference is for side-by-side intracorporeal esophagojejunostomy. The video presents our choice: an entry hole is performed in the esophagus and the jejunum, the linear stapler is inserted and the anastomosis performed, a boogie is progressed to the jejunum and then the esophagus sectioned (Fig. 3). A small entry hole remains and is easily closed by manual suture. When more extensive esophageal margin is required the esophagus is sectioned, frozen sections obtained, and a mechanical circular stapler or hand-sewn anastomosis performed. We prefer the last, which is made in two planes (full-thickness and seromuscular layer) with absorbable stitches. Suture is continuous, being interrupted at the angles. Barbed sutures can be used according to the surgeon's preference. The anastomosis is always tested with methylene blue.
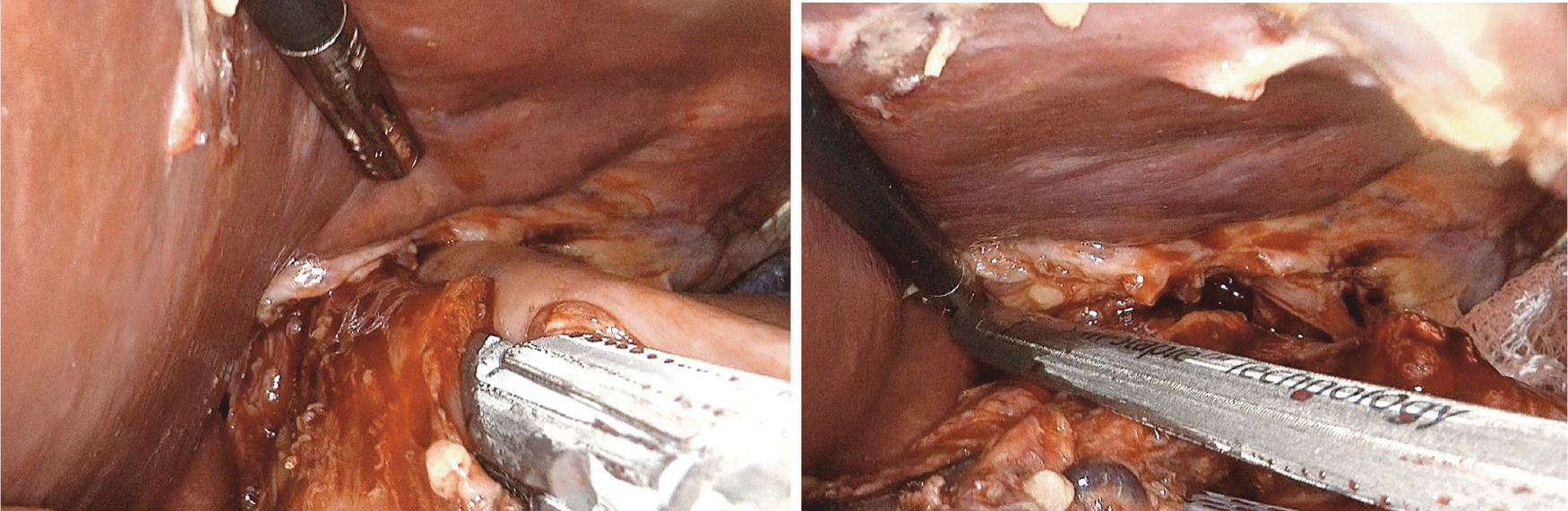
Side-by-side intracorporeal esophagojejunostomy followed by esophageal section.
A side-by-side stapled enteroenterostomy is created 60 cm below the esophagojejunostomy and the common opening is closed by hand-suturing. If the jejunal limb is too close to the Treitz ligament, manual anastomosis is preferred.
An open drain is left by the esophagojejunostomy and the specimen is removed after extending the camera trocar site.
The study was approved by the institutional review board.
Results
Between 2009 and 2019, 8 patients with RGC underwent LCTG. Patients characteristics are summarized in Table 1. Tumor location and size were defined by endoscopy.
Clinical Characteristics of Laparoscopic Completion Total Gastrectomy for Remnant Gastric Cancer
ASA, American Society of Anesthesiologists; BMI, body mass index; CCI, Charlson–Deyo Comorbidity Index; LCTG, laparoscopic completion total gastrectomy; SD, standard deviation.
Most patients were male (87.5%), with a mean body mass index of 22.6 and mean tumor size of 5.9 cm. Their mean age at the time of the first surgery was 38.9 years (range 25–56 years), and the mean interval between the first and the second gastrectomy was 32.1 years (range 13.6–49), with a mean age of 71.3 years at the time of the LCTG.
All patients had been previously operated by open method, 7 (87.5%) due to peptic ulcer disease and 1 due to gastric cancer. Billroth II was the previous reconstruction in all cases.
The mean operation duration was 272 minutes (range 180–330) and the median blood loss was 247 mL (range 50–500). No intraoperative blood transfusion was required. Mechanical side-to-side esophagojejunostomy was performed in all but one case (circular stapler). Pathological results are presented in Table 2. The mean number of retrieved lymph nodes was 28.6 and resection margins were negative in all cases. Three patients had esophagojejunostomy leakage, all were clinically managed by fasting, enteral nutrition, and broad-spectrum antibiotics. One of them died at postoperative day 73 due to pulmonary complications.
Pathological Characteristics
LCTG, laparoscopic completion total gastrectomy; SD, standard deviation.
Discussion
As experience in laparoscopic management of GC increases, the minimally invasive approach to RGC seems to be the next frontier. The procedure is complex, and as the prevalence of RGC is relatively rare only a limited number of cases are reported in the literature and clinical trials are unlikely to happen.
Compared with the open access, LCTG intends to achieve similar oncological results with the advantages of the laparoscopic approach (less intraoperative blood loss, faster recovery, fewer wound complications, less postoperative pain, and better cosmetic).5,6,8–16
Regarding morbidity, postoperative complications occurred in 37.5% of the cases, findings that are consistent with previous reports. A systematic review with 21 studies involving laparoscopic resection of RGC observed a postoperative complication rate ranging from 0% to 50% (8 studies showed no postoperative complications and 13 reported a postoperative complication rate ranging from 7% to 50%). This broad range must be interpreted in the context that all studies consist of retrospective small series, have selection bias, have short follow-ups, and include the learning curve (due to the rarity of RGC, few surgeons have the opportunity to gain sufficient experience with LCTG). In addition, RGC has high morbidity even with the open access. Eight studies compared laparoscopic and open completion gastrectomy, showing similar morbidity between the groups.5,7,8,10–27
The stepwise approach presented in this study intends to reduce the complexity of LCTG and give surgeons a head start over such a difficulty procedure. Rather than a rigid approach, the strategy showed provides tools to smooth the learning curve and encourage surgeons to laparoscopic manage RGC, seeking the known advantages of the laparoscopic access for this subgroup of patients. We also picked a case with anatomic variation (Supplementary Video S1) to exemplify, help avoid pitfalls, and prevent injuries. Hopefully, the clear step-by-step sequence will give confidence to peers, helping them reduce operative duration and complications.
Conclusion
LCTG for RGC is a demanding procedure. A standard approach is presented in this study to help surgeons in this next frontier.
Footnotes
Authorship Confirmation Statement
All individuals listed as authors agree that they have met the criteria for authorship, participated sufficiently in the study and approved the content of the submitted article.
Authors' Contributions
E.S. and A.R.D. were in charge of conception and design of study, critical analysis, and drafting and approval of the article to be published. M.F.K.P.R. was responsible for acquisition of data, critical analysis, and approval of the article to be published. A.Z.C. was in charge of acquisition of data and approval of the article to be published. U.R-J., B.Z., and I.C. were responsible for revising and approval of the article to be published.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.