
Abstract
Background:
Mucinous colorectal adenocarcinoma (MAC) has a higher incidence of local extension, leading to lower overall resection rates. Few studies have investigated the outcomes of laparoscopic surgery for MACs to date. Therefore, we aimed to elucidate the validity of laparoscopic surgery for mucinous adenocarcinoma (MAC).
Methods:
This study analyzed short-term and long-term outcomes between laparoscopic and open surgery for MACs from 2008 to 2018. Multivariate analyses were used to define prognostic factors of overall survival (OS) and disease-free survival (DFS).
Results:
Patients in the laparoscopy (LAP) group had significantly less blood loss, fewer days to first flatus and to diet, and shorter length of hospital stay. The 3-year and 5-year DFS rates for all stages combined were 65.7% and 62.5% in the LAP group compared with 60.5% and 57.6% in the open (OPEN) surgery group (P = .521). The 3-year and 5-year OS rates for all stages combined were 72.3% and 67.3% in the LAP group compared with 72.6% and 67.8% in the OPEN group (P = .934). OS and DFS in stage II, stage III, and pathological T4 (pT4) stage patients who underwent laparoscopic surgery did not differ from patients who underwent open surgery. Multivariate analysis showed that stage pT4, pN2, and carcinoembryonic antigen (CEA) were significant predictors of OS. Independent factors, including intraoperative blood transfusion, stage pT4, pN2, CEA, and CA19-9, carbohydrate antigen 19-9, have a great effect on DFS.
Conclusions:
Laparoscopic surgery is a safe and feasible option for mucinous colorectal AC, which provides faster postoperative recovery and less intraoperative blood loss.
Introduction
Colorectal cancer (CRC), which is the third most diagnosed cancer and fourth leading cause of cancer-related deaths, 1 is a malignant tumor with a high prevalence, and an estimated 1.2 million people develop CRC worldwide every year. CRC has been divided into various pathological types by the World Health Organization, such as classic adenocarcinoma (AC), mucinous adenocarcinoma (MAC), signet ring cell carcinoma, and other rare variants of colorectal carcinomas. 2 MAC accounts for 1.6%–25.4% of all CRCs, 3 which is defined as comprising more than 50% extracellular mucin produced by tumor acinar cells. The prevalence of CRC in large population-based studies showed a lower rate (4%–5%) of MACs in Asians.3,4
Some studies showed that MAC is more frequently found in female patients and in younger patients 5 and has a worse prognosis than AC.6–8 The worse prognosis of MAC may be owing to the more advanced stage at diagnosis, greater propensity for early spread to regional lymph nodes, and lower response to chemotherapy.6–8 Other studies show that MAC has a similar prognosis to AC 9 and is not an independent predictor of decreased survival. 4 Given the relative rarity of the disease, it is crucial to understand the treatment and prognosis for MAC. This article suggests that special management and treatment for MAC may be needed. 10
The comprehensive treatments for CRC are more and more important. Several treatment options for CRC have emerged, such as chemotherapy, radiotherapy, molecular targeted therapy, and immunological therapy; however, surgical resection remains the only way to achieve radical cure. The outcome of surgery for CRC has improved substantially during the past three decades because of the introduction of total mesorectal excision (TME). 11 The combination of laparoscopic resection and TME leads to a new level of treatment for this cancer. Since Jacobs et al. first reported the technical feasibility of laparoscopic colectomy, 12 laparoscopic surgery has been a recommended method for colorectal surgery. Widespread adoption of minimally invasive surgery for CRC improved short-term outcomes and similar long-term oncological outcomes compared with open colectomy.13,14 Laparoscopic surgery offers better short-term outcomes such as less intraoperative blood loss, less postoperative pain, higher probability of good resection quality, quicker postoperative recovery, and shorter hospital stay.13–16 However, some studies showed that laparoscopic surgery for pathological T4 (pT4) CRC remains controversial.17,18 Meanwhile, more evidence is needed to demonstrate the long-term outcomes of laparoscopic surgery.
Many studies have explored the advantages and disadvantages of laparoscopic surgery compared with open surgery for CRC, but no designated analysis of laparoscopic treatment of MAC was reported. Compared with the nonmucinous subtype, MAC is characterized by a higher ratio of lymph node infiltration and peritoneal implant. 19 Patients with MAC generally have tumors of a higher T stage than those with AC, which may have a higher incidence of local extension, leading to lower curative and overall resection rates.10,20 Especially in the T4 stage of MAC, there may be invisible peritoneal metastasis (not detected by imaging). Therefore, it is necessary for us to conduct an intensive study of the laparoscopic treatment for MAC. This retrospective study aims to compare the outcomes of laparoscopic surgery with open surgery for MAC and investigate the risk factors for disease-free survival (DFS) and overall survival (OS) of patients with the disease after a curative operation.
Materials and Methods
Patients
All mucinous CRC patients treated at Guangzhou First People's Hospital and the Third Affiliated Hospital of Sun Yat-Sen University from 2009 to 2018 were enrolled in this study. Local institutional review boards (IRB) approved the data acquisition. The data included demographics, surgical procedure, pathologic stage, adjuvant therapy, recurrence, and survival rates. All patients were staged according to the American Joint Committee on Cancer (AJCC) seventh edition manual for CRC. The inclusion criteria included the following: (1) history of primary CRC; (2) histologically confirmed MAC; and (3) undergoing definitive open and laparoscopic surgery. The exclusion criteria included the following: (1) MAC with peritoneal or visceral metastasis (M1 stage); (2) palliative resection; (3) patients with emergency surgery; and (4) multiple primary tumors of the colorectum. Ethical approval was not necessary because this study was a retrospective study.
Surgical technique
Both open and laparoscopic surgeries were performed by colorectal surgeons with extensive experience. All laparoscopically assisted and open colectomies were radical resections with a complete mesocolic excision, central vascular ligation, and combined resection of invaded adjacent organs, which were performed according to protocol guidelines. Fasting until fluid and solid intake was based upon patient's tolerance in both surgical groups.
Histopathological examination
All specimens were examined by pathologists and surgeons shortly after surgery.
MAC is a histological subtype of CRC, which is defined as comprising more than 50% extracellular mucin, typically characterized by pools of extracellular mucin-containing malignant epithelium. The presence of MAC was documented. The status of lymph node metastasis was evaluated by pathologists through hematoxylin–eosin staining.
Observation indexes
Preoperative indexes included age, gender, body–mass index (BMI), tumor location, American Society of Anesthesiologists (ASA) score, comorbidity, and tumor markers, carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 (CA19-9). The intraoperative indexes included operation time, blood loss, blood transfusion, intraoperative complications, combined organ resection, postoperative complications, number of lymph nodes harvested, and conversion to open surgery. Postoperative indexes included tumor size, pathological T stage, pathological N stage, positive lymph node numbers, tumor grade, resection margin status, postoperative complications, flatus, resumption of oral intake, and hospital stay. Patients who had a conversion from a laparoscopic surgery to open procedure were categorized as having undergone open surgery.
The follow-up indexes included adjuvant chemotherapy received, DFS, and OS. For DFS, the follow-up time was recorded from the date of surgery to the first recurrence date for those with recurrence. For OS, the follow-up time was recorded from the date of surgery to the last follow-up date or from the date of surgery to the date of expiration.
Postoperative adjuvant chemotherapy and follow-up
The tumor, node, and metastasis (TNM) classification was defined by the criteria of the seventh AJCC/Union for International Cancer Control. After recovery from surgery, adjuvant chemotherapy by oncologists was recommended for patients with TNM stage III and high-risk stage II disease, unless there were contraindications related to a patient's performance status. According to the National Comprehensive Cancer Network guideline, patients were monitored with physical examinations and blood test results (CEA and CA19-9) every 3–6 months for the first 2 years and then every 6 months for the next 3 years. Chest/abdominal/pelvic computed tomography scan was performed every year for the first 5 years. Colonoscopy was performed 1 year after surgery (within 3–6 months if preoperative colonoscopy was incomplete) and every 2 years thereafter.
Statistical analyses
Statistical analyses were performed using SPSS26.0. Quantitative data are reported as the mean ± standard deviation or median. Categorical data were compared by χ 2 tests or Fisher's exact test, comparison of continuous data was done by use of the Mann–Whitney test. Survival curves (OS and DFS) were derived from Kaplan–Meier estimates, and the curves were compared by the log-rank test. Prognostic factors were identified by univariate analysis and further tested by multivariate analysis in Cox regression analysis. When the P value was <.15 in univariate analysis, it would be included in the multivariate analysis. Multivariate analysis was compared by forward stepwise (conditional likelihood ratio) regression. Results are reported as hazard ratios with 95% confidence intervals. A P value <.05 was considered statistically significant.
Results
During the period from 2009 to 2018, we collected a total of 162 mucinous CRC cases, according to the pathological database, from 4527 cases of CRC at the Guangzhou First People's Hospital and the Third Affiliated Hospital of Sun Yat-Sen University. There were 83 cases in the laparoscopy (LAP) group and 79 cases in the open surgery (OPEN) group. (Fig. 1)

Study flowchart showing patient selection. G, Guangzhou First People's Hospital; Z, The Third Affiliated Hospital of Sun Yat-Sen University.
There were no significant differences in age, gender, BMI, ASA score, tumor location, CA19-9, CEA, adjuvant therapy, or recurrence between the two groups (P > .05) (Table 1).
Clinical Information of One Hundred Sixty-Two Colorectal Cancer Cases
ASA, American Society of Anesthesiologists; BMI, body–mass index; CA19-9, carbohydrate antigen 19-9; CEA, carcinoembryonic antigen; LAP, laparoscopic surgery; OPEN, open surgery; SD, standard deviation.
For surgical outcomes, there were 6 (7.23%) patients who underwent conversion to open surgery, and all conversion cases were analyzed in the OPEN group. No relevant differences were noted between the two groups in terms of tumor size, intraoperative complications, and combined organ resection. Operative time showed no significant differences, while blood loss was significantly lower in the LAP group compared with the OPEN group (100.7 ± 87.2 mL versus 169.0 ± 127.9 mL, P = .007). The number of cases with postoperative complications within 30 days showed no relevant differences between the two groups. However, the frequency of appearance in postoperative complications within 30 days was 15 versus 25 in the LAP group compared with the OPEN group. With regard to postoperative recovery indexes, the LAP group was significantly better than the OPEN group (P < .05) in time to flatus and diet. The median hospital stay was 10 (5–62) days for the LAP group and 13 (7–42) days for the OPEN group, which showed a relevant difference between the two groups (P = .000) (Table 2).
Surgical Outcomes of One Hundred Sixty-Two Colorectal Cancer Cases
Some patients have multiple postoperative complications.
LAP, laparoscopic surgery; NR, no ratio; OPEN, open surgery; SD, standard deviation.
Regarding pathologic outcomes, the LAP group and OPEN group had no significant differences in terms of pT stage, pN stage, pTNM stage, and tumor margin (P > .05) (Table 3).
Pathologic Outcomes of One Hundred Sixty-Two Colorectal Cancer Cases
LAP, laparoscopic surgery; OPEN, open surgery; p, pathological; TNM, tumor, node, and metastasis.
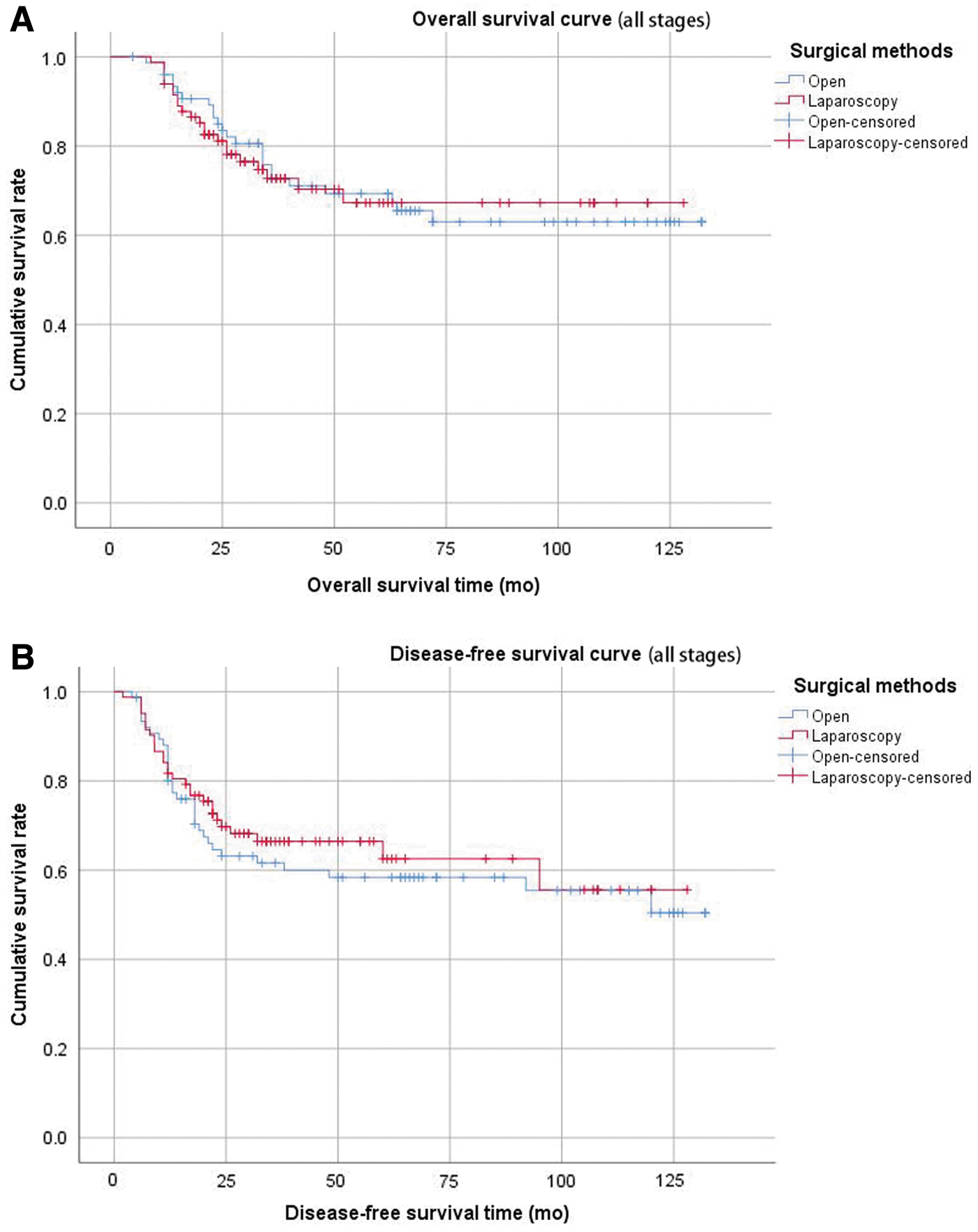
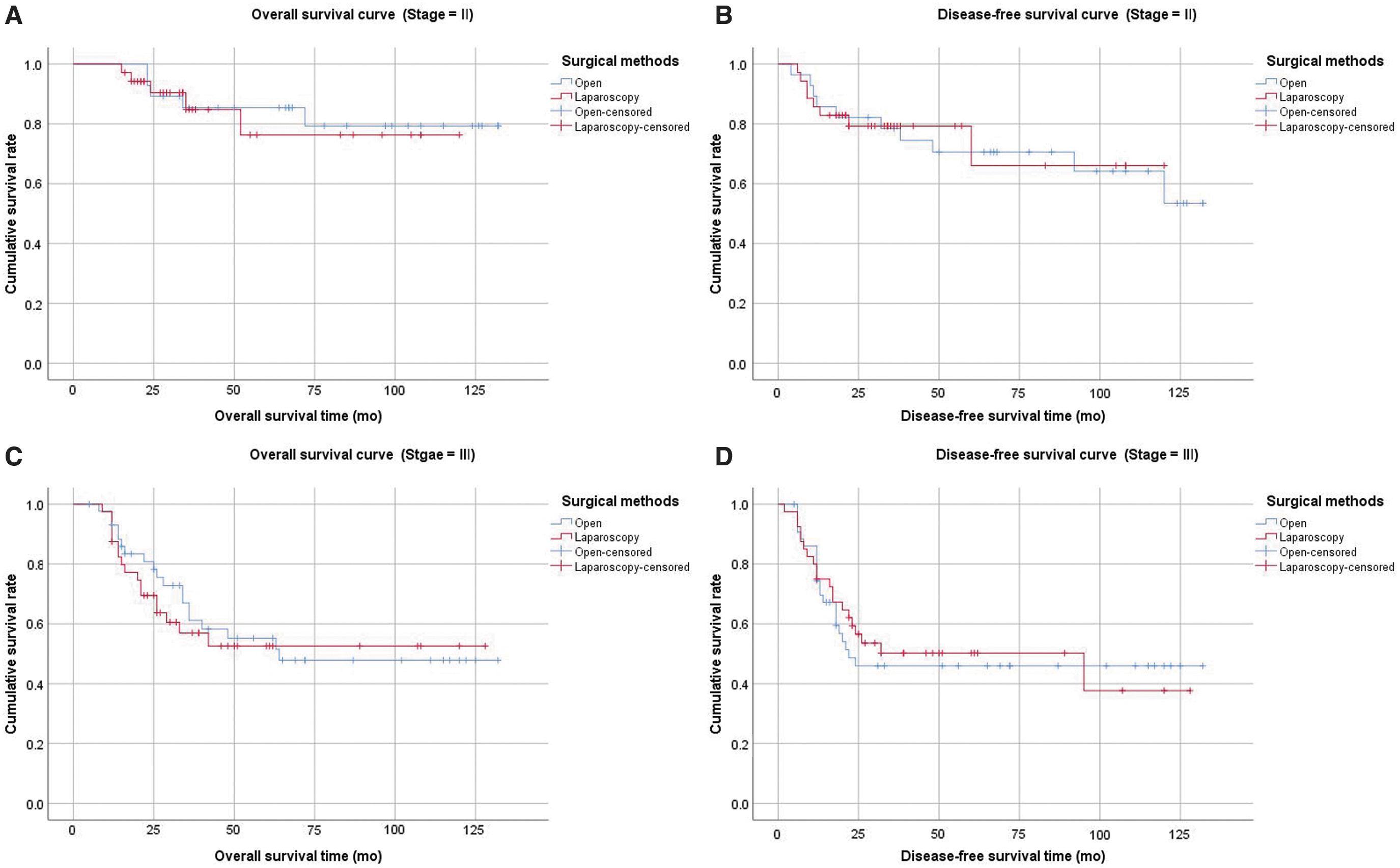
The median overall follow-up time was 37 months. OS and DFS rates in patients who had laparoscopic surgery were not different from patients who underwent open surgery (Fig. 2). The 3-year and 5-year DFS rates for all stages combined were 65.7% and 62.5% in the LAP group compared with 60.5% and 57.6% in the OPEN group (P = .521 by log-rank test). The 3-year and 5-year OS rates for all stages combined were 72.3% and 67.3% in the LAP group compared with 72.6% and 67.8% in the OPEN group (P = .934 by log-rank test). OS and DFS rates in stage II (P = .783 and P = .893), III (P = .676 and P = .799), and pT4 (P = .854 and P = .279) patients who underwent laparoscopic surgery were not different from patients who underwent open surgery (Figs. 3 and 4).

Multivariable analysis of DFS and OS did not show differences between laparoscopic and open surgery. In univariate and multivariate analyses of the entire cohort, the factors of stage pT4, pN2, and CEA were significant predictors of OS and the factors of transfusion, stage pT4, pN2, CEA, and CA199 were significant predictors of poorer DFS (Table 4).
Univariate and Multivariate Analyses of One Hundred Sixty-Two Mucinous Adenocarcinoma Patients for Overall Survival and Disease-Free Survival
p value < 0.05.
Cox multivariate analysis method = forward stepwise (conditional LR).
CA19-9, carbohydrate antigen 19-9; CEA, carcinoembryonic antigen; CI, confidence interval; HR, hazard ratio; LAP, laparoscopic surgery; LR, likelihood ratio; OPEN, open surgery; p, pathological; TNM, tumor, node, and metastasis.
Discussion
MAC is a unique pathologic entity first described by Parham in 1923. 21 Compared with colorectal AC, MAC more often has microsatellite instability, 22 which is also more likely to lead to lymph node metastasis, peritoneal implant, lymphovascular invasion, and perineural invasion. 4 Considering the particularity of MAC, patients with MAC may require adjustments in treatment; however, surgical resection remains the only way to achieve radical cure. The challenge of surgical treatment for MAC is avoiding intraoperative spillage and rupture of gelatinous MAC into the abdominal cavity. This challenge may become more difficult because of the complexity of laparoscopic operations and the influence of pneumoperitoneum. Therefore, we collected 162 mucinous CRC cases, according to the pathological database, from 4527 cases of CRC. There are 237 cases of MAC. The rate of MAC is 5.24%, consistent with other studies, showing that the mucinous subtype accounts for 4%–5% of CRCs from Asian countries.4,23 We divided these appropriate cases into two groups, the LAP group (83 cases) and OPEN group (79 cases). Short-term outcomes and long-term oncology outcomes were compared between the two groups. To our knowledge, this is the first attempt to compare the outcomes of laparoscopic versus open surgery for mucinous colorectal AC.
Since the first report of laparoscopic colorectal resection in 1991, laparoscopic surgery has become a recommended method for CRC surgery and is popularized in most hospitals. Several randomized controlled trials have shown that long-term oncological outcomes of laparoscopic surgery and the quality of the surgical specimen are equivalent to those of open surgery; however, recovery, physiological function, and other short-term outcome measures are improved with the laparoscopic approach.14,24–27 We found that laparoscopic resection for MAC could significantly reduce intraoperative blood loss, which was consistent with results from other studies.28,29 We consider that reduced blood loss is a result of the magnifying effect of laparoscopic operation and more careful operation. Laparoscopic surgery is less invasive than traditional (OPEN) surgery and reduces postoperative pain, and many studies have shown that laparoscopic surgery can reduce recovery time and the length of hospital stay.27,30–32 Our study also shows that the LAP group has significant advantages in time to flatus (P = .022), early oral feeding (P = .009), and hospital stay (P = .000) compared with the OPEN group (Table 2). We found that no significant differences were noted between the groups in terms of postoperative complications; however, some frequencies of complications in the LAP group were significantly lower than those in the OPEN group, especially in complications such as incision infection, pulmonary infection, and postoperative intestinal obstruction (Table 2). This is because patients with laparoscopic surgery can ambulate early and cough with less pain. Infection is one of the most common complications in the OPEN group, which means attention should be paid to the suture of incision and intraoperative sterile principles.
R0 resection and lymph node dissection are important factors affecting long-term survival in CRC surgery. Our study showed that there was no difference in the R0 resection rate, lymph node number, and pathological results between the two groups. We found no differences in the 3- and 5-year OS rates (P = .934) and 3- and 5-year DFS rates (P = .521) when comparing the two groups. We found that 46.2% of the cases in our study were stage pT4, consistent with some studies that showed MACs generally have higher clinical T stage than AC. 10 The European Association of Endoscopic Surgery and AJCC do not recommend laparoscopic treatment of pT4 CRC. 17 However, some studies have different opinions on LAP surgery being an acceptable and safe treatment for pT4 CRC patients.33–35 We found that the LAP group had no statistical difference compared with the OPEN group in OS (P = .854) and DFS (P = .279) rates for pT4 MAC by stratified analysis. Our results showed that 93.5% of patients were at stage II or stage III, which concurred with previous reports demonstrating that MAC was often present in an advanced stage.3,10,36 The more advanced stage of mucinous tumors is attributed to many factors, including being of less firm consistency than AC and the tendency to afflict the proximal colon, which serves to delay clinical symptoms until a more advanced stage has been reached. This study shows that the two groups had no differences in OS and DFS rates for stage II and stage III of MAC. Therefore, we believe that laparoscopic treatment in MAC can achieve similar oncological outcomes to open surgery. On analysis of the predictive factors for clinical outcomes, our data detected the depth of tumor infiltration (stage pT4), lymph node status (pN2), and CEA as independent predictors of OS. Stage pT4, pN2, CEA, CA19-9, and transfusion were independent predictors of DFS. The extensive invasion of the tumor into the colonic wall and lymph node metastasis increase intraoperative difficulties as a result of increasing intraoperative blood transfusion. Therefore, intraoperative blood transfusion is an independent predictor of DFS.
In brief, the results of this study suggest that laparoscopic surgery for MAC is a safe and technically feasible option. This study is not without limitations, the small number of patients studied and its retrospective nature are important limitations that have to be considered. Large-scale studies and multicenter studies are needed for more extensive analyses.
Conclusions
This study demonstrated that laparoscopic surgery for MAC reduces intraoperative blood loss, provides faster recovery, and does not adversely affect oncological outcomes. Stage pT4, pN2, and CEA were significant predictors of OS. Intraoperative blood transfusion, stage pT4, pN2, CEA, and CA19-9 were independent factors affecting DFS. We believe that laparoscopic resection of MAC is a safe and technically feasible option, but it should be performed by experienced surgeons. The credible guidelines for CRC and to treat different phenotypes such as MAC need future prospective studies.
Footnotes
Ethics Approval Statement
Ethical approval was obtained from the local institutional review board.
Patient Consent Statement
Informed consent was waived.
Author Contributions
Guarantors of the integrity of the entire study are Q.H., M.-H.Z., W.-L.L., and J.C.; study concepts/study design or data acquisition or data analysis/interpretation was performed by all authors; manuscript drafting or manuscript revision for important intellectual content was performed by all authors; approval of the final version of the submitted manuscript was given by all authors; literature research was performed by M.-H.Z. and Q.H.; and manuscript editing was done by all authors.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Medical Science and Technology Research Fund Project of Guangdong (A2019526), National Natural Science Foundation of China (81871943, 81972780), Natural Science Foundation of Guangdong Province (2017A030311035), and Basic and Applied Basic Research Fund of Guangdong Province (2020A1515010051).