
Abstract
Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) is a recent surgical advancement for increasing the rate of successful liver resection. This technique is particularly important for patients with advanced tumor burden in whom future liver remnant volume is estimated to be too small to meet hepatic metabolic demands. With increasing acceptance of laparoscopic liver surgery and the related experience, even complex liver resection techniques such as ALPPS have been performed laparoscopically to improve patient outcomes. However, conventional laparoscopy has certain technical limitations that can result in a lack of dexterity. By overcoming these limitations, robot-assisted laparoscopy could become the preferred procedure for complex liver resection. In this study, we describe the technique of fully robotic ALPPS with simultaneous left colectomy in a patient with stage IV colorectal cancer. We emphasize on the performance of the robotic platform during certain difficult steps of the procedure.
Introduction
For the past two decades, the treatment of colorectal liver metastases (CLMs) has undergone tremendous improvements as a result of the advancements in systemic therapy, perioperative care, and surgical treatment. Several studies have shown that simultaneous resection of the primary tumor and synchronous CLMs is safe and effective as staged approach in selected patients. 1 In recent years, associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) 2 and its modified version, that is partial-ALPPS (p-ALPPS), 3 have been included among the conventional strategies for increasing the rate of liver resection in patients with advanced tumor burden and insufficient future liver remnant (FLR) volume. Compared with conventional two-stage liver resection, ALPPS is associated with better liver regenerative capacity and improved second-stage procedure outcomes. 4 Laparoscopic liver resection has been widely accepted, and its indications are expanding rapidly. 5
The possibility of performing complex liver resection with a minimally invasive approach is extremely appealing, and laparoscopic ALPPS has been reported to be feasible and safe. 6 However, ALPPS is a technically demanding procedure and conventional laparoscopy has some limitations, including the use of rigid instruments with a limited degree of motion, two-dimensional view, and unstable camera platform, which complicate complex liver resection. By overcoming these limitations, robot-assisted laparoscopy can increase the feasibility of minimally invasive surgery involved in complex liver resection with potential improvement in patient outcomes.
Methods
In this study, we report about a patient with colorectal cancer and synchronous CLMs who was successfully treated by fully robotic ALPPS and simultaneous left colectomy. The surgical technique is described step by step. Using supplemental videos, we also show in detail the performance of the robotic platform during technically demanding steps of the first and second stages of liver resection. The Institutional Review Board approved this study.
Results
Case presentation
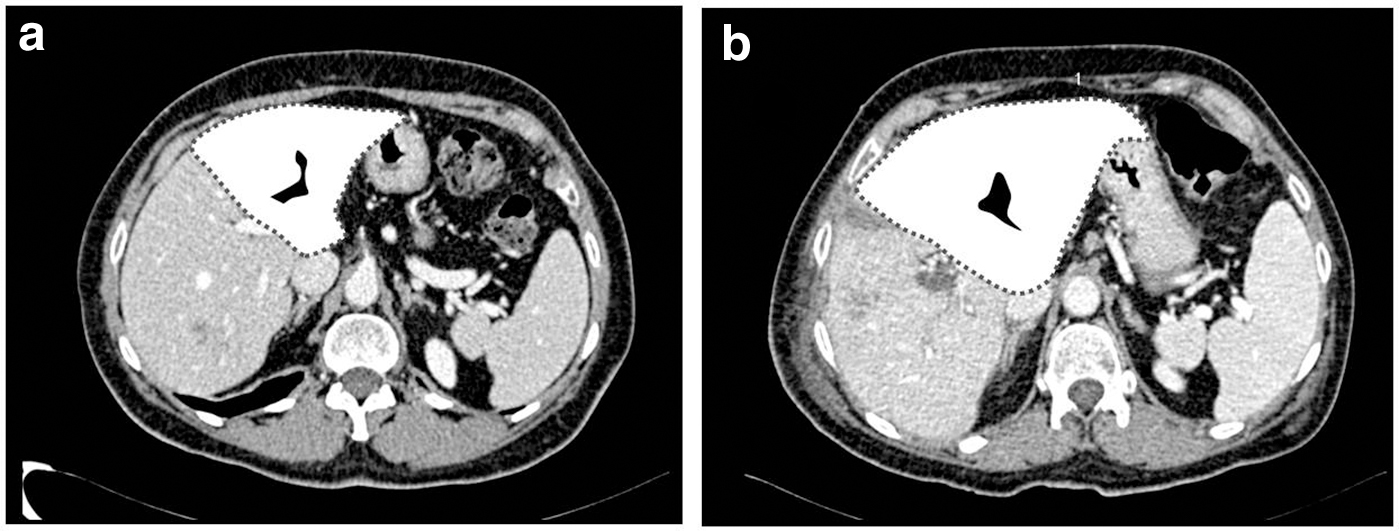
A 61-year-old woman presented with vague abdominal pain. Abdominal ultrasonography revealed multiple solid liver lesions. Contrast-enhanced computed tomography (CT) of the chest and abdomen showed four lesions (Sg4–5, Sg5, Sg6, and Sg7) in the right liver lobe, with the largest being 9 cm in size (Fig. 1a). CT revealed thickening of the left colon wall. Subsequent colonoscopy detected a 4-cm ulcerated lesion in the sigmoid colon, and biopsy confirmed the lesion to be invasive adenocarcinoma. Molecular analysis revealed a KRAS exon 2 mutation and wild-type NRAS and BRAF.

Contrast-enhanced CT scan showing CLMs in the right lobe before
After multidisciplinary tumor board evaluation, first-line chemotherapy comprising 5-fluorouracil, oxaliplatin, and bevacizumab was initiated. A significant tumor response was detected on CT after chemotherapy completion (Fig. 1b). Liver-specific contrast-enhanced magnetic resonance imaging confirmed the number and location of liver lesions; accordingly, the patient was referred to our department of surgery.
According to our policy, combined resection of the primary tumor and CLMs in a single procedure was considered; however, given the small FLR volume (Fig. 2a), liver resection with p-ALPPS combined with left colectomy was planned. Given our background in laparoscopic colorectal and liver resections (Table 1) and the recent implementation of robotic surgery at our department, the procedure was attempted using the Da Vinci “Xi” Surgical System platform (Intuitive Surgical, Sunnyvale, CA).
CT liver volumetry.
Minimally Invasive Colorectal and Liver resections at Our Institution (January 2006–March 2020)
For cancer or precancerous lesions.
From October 2019.
For benign and malignant lesions.
CD, grade of complication according to Clavien–Dindo classification; IQR, interquartile range.
Stage 1: robotic left colectomy combined with simultaneous first-stage p-ALPPS
The patient was placed in the supine position with legs apart. The operating table was adjusted to the 20° Trendelenburg position and rotated 20° toward the right. After pneumoperitoneum was established using a Veress needle, an optical trocar was introduced in the right flank and attached to a high-pressure continuous-flow insufflation system for assistance (AirSeal IFS system; SurgiQuest, Milford, CT).
Left colectomy was performed first (Supplementary Video S1). Four robotic ports were positioned along an oblique line from the left costal margin to the right anterior superior iliac spine (Fig. 3a). Standard left colectomy with intracorporeal vascular control and central lymph node dissection was performed. After dividing the rectum just above the peritoneal reflection using an articulated stapling device, the transection site at the level of the descending colon was identified using indocyanine green angiography. Then, the large bowel was exteriorized through a wound protector through suprapubic minilaparotomy and transected. Intracorporeal colorectal anastomosis was completed using transanal double-stapling technique.
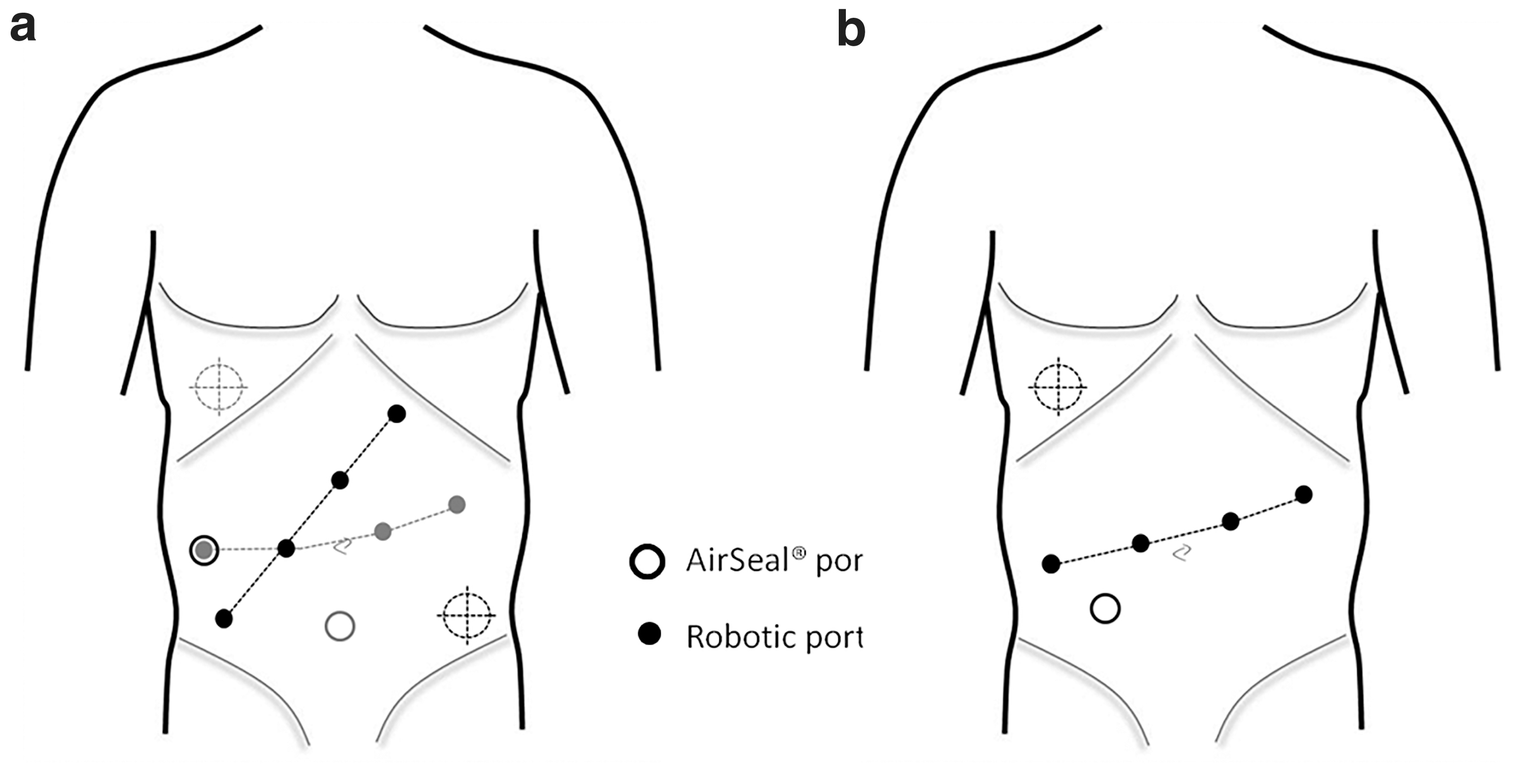
Schematic of the port placement.
Subsequently, liver resection was performed as planned (Supplementary Video S2). For performing the first step of p-ALPPS, redocking was necessary. Two additional robotic ports were introduced along the transverse umbilical line, and the assistant port was shifted to the site of the previous suprapubic minilaparotomy (Fig. 3a). The patient was placed in the 15° reverse Trendelenburg position and rotated 10° toward the left. Intraoperative ultrasound (IOUS) confirmed the number and sites of liver lesions. Cholecystectomy was not performed during the first stage of liver resection because IOUS revealed that the metastasis in Sg5 had infiltrated the gallbladder. A vessel loop was passed around the hepatic pedicle to facilitate the Pringle maneuver. Hilar dissection was performed using monopolar scissors. The right hepatic artery was looped, and the portal plate was exposed. The patient had portal trifurcation; therefore, the right posterior and anterior branches of the portal vein were individually isolated and encircled. After selective clamping of the right hepatic artery and both portal vein branches, discoloration on the Glissonian surface was marked using electrocautery. Next, the portal branches were ligated and the liver parenchyma was partially transected along the Cantlie line using an ultrasonic scalpel. On completion of the procedure, a nonsuction drain was placed along the transection groove.
Operation time was 361 min, and blood loss was 350 mL. The postoperative course was uneventful. After postoperative day 10, CT and hepatobiliary scintigraphy were performed to evaluate FLR hypertrophy (Fig. 2b) and liver function, respectively. The estimated FLR volume was considered adequate, and after 1 week the second stage of p-ALPPS was performed (Supplementary Video S3).
Stage 2: second-stage robotic p-ALPPS
Patient position and trocars placement were the same as those used in first-stage p-ALPPS (Fig. 3b). After cholecystectomy, the right branch of the hepatic artery was reisolated and divided with clips. The previously isolated right portal branches were identified, encircled, and individually divided in the same manner. The right hepatic duct was incised. After obtaining control over the vascular inflow, parenchymal transection was completed under IOUS guidance using an ultrasonic scalpel and bipolar forceps. The Glissonian pedicles and right branches of the middle hepatic vein were individually divided with clips. A major branch of the middle hepatic vein and the right hepatic vein were divided intraparenchymally using an articulating vascular stapler. Finally, the stump of the right hepatic duct was closed with a running suture. A specimen was extracted through suprapubic minilaparotomy, and a nonsuction drain was placed near the surface of the parenchymal transection.
Operation time was 327 min, and blood loss was 400 mL. The patient was treated for a surgical site infection at the site of suprapubic minilaparotomy on postoperative day 5 and was discharged 8 days after the second operation.
Complications
The most worrisome intraoperative complication of this procedure is massive bleeding secondary to hepatic vessels injury. Gentle dissection and adequate vascular exposure may prevent this complication. Once hemorrhage occurs, definitive primary repair through direct suture (e.g., lateral venorrhaphy) may be attempted. In this phase, the key concept is rapid achievement of vascular control, because an excessive delay may lead to fatal outcome. If minimally invasive management fails to control bleeding, conversion to open surgery is mandatory. Contrary to popular belief, the robotic platform does not significantly interfere with the conversion since robotic arms can be removed quickly from the operating field.
Additional complications include bile leakage, abdominal abscess, anastomotic leakage, and liver failure.
Conclusions
Fully robotic two-stage liver resection with ALPPS and simultaneous left colectomy was successfully performed. Extensive experience in laparoscopic liver surgery considerably shortened the learning curve required to perform robotic liver resection. Moreover, the use of robotic platforms can enhance the feasibility of minimally invasive surgery for complex abdominal surgery. The extent of its influence on patient outcomes should be explored in appropriately designed trials.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.