
Abstract
Background:
Delayed gastric emptying (DGE) is a common complication after esophagectomy with gastric tube reconstruction. It is still unclear whether a pyloric drainage procedure might reduce the risk of DGE.
Methods:
We identified in our database all patients subjected to Ivor Lewis esophagectomy after neoadjuvant chemoradiotherapy in the period 2000–2012. In the period 2000–2009, we performed a routine pyloroplasty (pyloroplasty group, PP group, 15 patients), after 2009 we did not perform any type of pyloric drainage procedure (nonpyloroplasty group, NPP group, 11 patients). We compared the groups with subjective questionnaires to assess the perceived quality of life (QoL) (QLQ-C30 and OES-18) and with objective test to study the gastric tube emptying (timed barium swallow test, scintigraphy, 24 hours' pH-metry).
Results:
No difference was observed in questionnaires QLC-C30 and OES-18 scores: 73% of patients in PP group and 63% in NPP group scored their overall QoL as good to excellent (QLC-C30). We did not report difference in timed barium swallow test results and in scintigraphy results. Twenty-four-hour pH-metry results showed in PP group a nonsignificant higher number of acid reflux episodes (NPP group 23.2 ± 9.5 versus PP group 41.3 ± 10.7, P = .29) and a longer time with pH <4 (NPP group 0.89% ± 1.6% versus PP group 3.1% ± 2.1%, P = .24).
Conclusions:
In our series, pyloroplasty was not associated with improved long-term QoL nor with better gastric conduit emptying. Further studies are needed to confirm these findings.
Introduction
Surgery is a cornerstone in the curative treatment of esophageal malignancies. Even if several different techniques to treat esophageal cancers are reported in the literature, in all the most common procedures the stomach, either as a whole or fashioned in a gastric tube, is utilized for alimentary tract reconstruction. The management of the pylorus is one of the main unsolved issues in this setting: during the proximal esophageal resection, the vagus trunks are necessarily sectioned, thus removing the inhibitory parasympathetic innervation 1 to the pylorus. According to some authors, 2 the resultant hypertonia of the pylorus may lead to clinically relevant delayed gastric emptying (DGE). In some series, DGE has been described in 4%–50% 3 of patients after esophagectomy. The consequent stasis within the gastric tube is associated with symptoms (i.e., vomiting, nausea, and early satiety) and with higher risk of complications such as aspiration pneumonia.
Pyloric drainage procedures are widely used to reduce the risk of DGE, but there is no agreement on their actual benefits. Many authors suggest that only a minority of patients suffer from DGE and that the intrinsic motor activity of the gastric tube can recover, even completely. 4 Moreover, these additional procedures can carry various complications such as shortening of the gastric tube, increased gastric dumping, biliary reflux, and even severe leak.
The current literature on this topic remains contradictory, and no consensus has been reached so far neither about the usefulness of pyloric drainage 2 nor about the optimal drainage technique 4 (pyoroplasty versus pyloromiotomy versus botox injection). Most of published studies have a small and heterogeneous sample size and often compare different surgical procedures. In addition, in many studies, data on long-term functional outcomes after surgery are not reported. Lastly, the definition of DGE varies widely across the studies, being defined either on the basis of symptoms of gastric stasis5,6 or on the presence of specific radiological findings,7,8 or both.9,10
The aim of our study is to compare two homogeneous groups of patients subjected to open Ivor Lewis esophagectomy (with or without pyloroplasty) in terms of solid and liquid gastric emptying, acid reflux in the esophageal remnant, and quality of life (QoL) after at least 12 months after surgery.
Patients and Methods
We reviewed our prospectively maintained database to identify all patients who underwent Ivor Lewis esophagectomy for esophageal cancer at our institution in the period January 2000– December 2012. Among them, we selected the patients who fulfilled the following criteria: age 18–80 years, no previous operations on the upper gastrointestinal (GI) tract, neoadjuvant chemoradiotherapy according to our protocol (proposed in a previous publication 11 ), curative (R0) resection, no sign of anastomotic stricture, no signs of recurrence at the last follow-up, and a follow-up period of at least 12 months. All patients considered as eligible for the study were proposed to join the study through an informational interview.
The standard surgical procedure was a modified open Ivor Lewis esophagectomy with a two-field lymphadenectomy. The continuity of the digestive tract was achieved through a right intrathoracic esophagogastric circular stapled (25 mm) end-to-end anastomosis, with a narrow gastric tube (3 cm wide). 12 Until December 2009, we performed as routine a prophylactic Heineke–Mikulicz pyloroplasty (pyloroplasty group, PP). After January 2010, we changed our clinical practice not performing anymore any type of pyloric drainage procedure (nonpyloroplasty group, NPP).
Patients were asked to complete the EORTC (European Organization for Research and Treat of Cancer) questionnaires QLQ-C3013 and OES-1814 for the assessment of QoL and functional disorders after esophagectomy; they were also subjected to a timed barium swallow test, a scintigraphy with radiolabeled solid meal, and a 24-hour pH-metry. The study was approved by the IRB of the University of Verona.
Timed barium swallow test
We used the Mecalc CLISIS instrument, set on the program for the digestive system contrasts with 1 image/sec and normal magnification. The focus–detector distance was set to 115 cm, with tube at 0°. The patient was positioned upright in front of the camera. Patients were asked to drink, in a single swallow, 45 mL of barium (Prontobario-Bracco™) diluted in 100 mL of water. We recorded 20 seconds of continuous fluoroscopy after the initial swallow, with subsequent radiographs at 1, 5, 10, and 45 minutes, measuring height, width, and the area of the barium columns above the pylorus at every time. Patients had fasted for at least 8 hours before the test, and during the breaks were recommended not to eat or drink.
Scintigraphy
We used a gamma-camera Picker Prism 1500 with parallel holes LEHR collimator and a computer Odyssey Fx. A semisolid balanced meal (80 g, protein 5.2%, carbohydrates 7.1%, fat 2.5%) was labeled with 40 MBq of 99mTc-nanocolloid. During the test, they were seated close to the gamma camera (field of view from the jugular notch to the upper abdomen, images matrix 128 × 128, zoom 1). To study the gastric emptying, we first acquired dynamic images of 60 seconds per frame for 30 minutes, then we acquired static images of 60 seconds per frame every 10 until 120 minutes postoral administration. The images were aligned and analyzed using region of interest drawn on the gastric conduit. Parametric images and time–activity curves were created. Patients were asked not to drink or eat in the 6 hours before the test. During the intervals, we invited the patients to stand up and to walk to mimic the normal prandial behavior but to avoid eating or drinking.
Twenty-four hours' pH-metry
We performed a 24 hours pH-metry with a two-channel catheter equipped with two electrodes placed at a distance of 15 cm. The upper electrode was placed 2 cm below the upper esophageal sphincter (identified through an esophageal manometry) and the lower electrode in the gastric tube. Patients were asked to stop proton pump inhibitors therapy at least 10 days before the test. We analyzed the number of reflux episodes, the time with pH <4 in the esophageal remnant, and the recovery of acidity in the gastric conduit.
Statistical analysis
Significance of differences between groups (PP group; NPP group) was evaluated using Fisher's exact test for nominal variables, chi square for ordinal variables and Wilcoxon–Mann–Whitney rank-sum test for continuous variables. Statistical significance was set at P < .05. P values reported are two tailed.
Results
A total of 341 patients underwent Ivor Lewis esophagectomy in the study period: among them, 63 fulfilled the inclusion criteria. After the informational interview, 37 patients refused to join the study. The final sample size was 26 patients: 15 patients (57.7%) underwent a pyloroplasty procedure (PP group), whereas in 11 cases (42.3%) we did not perform a pyloric drainage procedure (NPP group). Table 1 presents patients' baseline characteristics.
Baseline Characteristics of the Patients
NPP, nonpyloroplasty; PP, pyloroplasty.
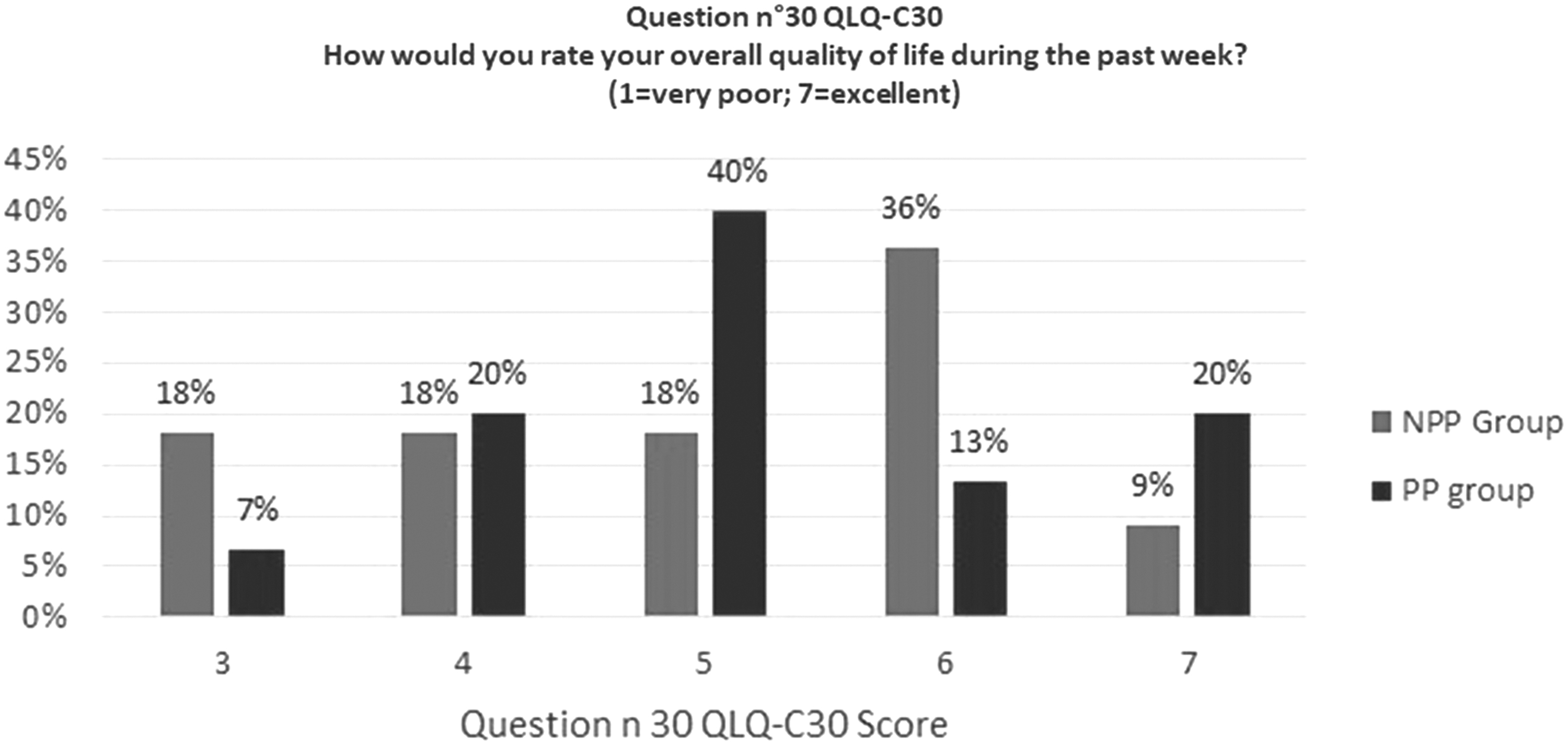
EORTC questionnaires QLQ-C30 and OES-18
Because of the small sample size, we decided to report four questions: question Nos. 38, 44, and 45 from OES-18 and question No. 30 from QLQ-C30. The results are given in Table 2 and in Figure 1. We did not observe differences between the groups with regard to problems with eating (Question No. 38 OES-18: “Have you had trouble with eating?”), episodes of indigestion/heartburn (Question No. 44 OES-14: “Have you acid indigestion or heartburn?”), and troubles with acid or biliary reflux (Question No. 45 OES-18: “Have you had trouble with acid or bile coming into your mouth?”). Furthermore, when considering their overall QoL through Question No. 30 from QLQ-30 (“How would you rate your overall quality of life during the past week?”), patients had similar results in both groups: no patient scored his QoL as very poor (scores 1 and 2), whereas the majority reported their QoL as good–very good (scores 5 and 6).
EORTC questionnaire QLQ-C30. EORTC, European Organization for Research and Treat of Cancer.
European Organization for Research and Treat of Cancer Questionnaire OES-18
NPP, nonpyloroplasty; PP, pyloroplasty.
Timed barium swallow
The results of the timed barium swallow test are listed in Table 3. There were no significant differences in the mean width of the gastric conduit (PP group 5.3 ± 0.8 cm versus NPP group 5.3 ± 1.3 cm, P = .46). The mean value of the area of the barium column after 1 and 5 minutes was slightly higher in the PP group, without statistically significant differences. The area of the barium column at 45 minutes after the swallow was comparable between the groups (PP group 10 ± 5.8 cm2 versus NPP group 10 ± 6.4 cm2, P = .94).
Timed Barium Swallow Results
Measured as width of the barium column.
NPP, nonpyloroplasty; PP, pyloroplasty.
Scintigraphy
Table 4 gives the scintigraphy results. The mean half time was 10 minutes shorter in the PP group, without statistical significance (PP group 29 ± 22.3 minutes versus NPP group 40.6 ± 15.5 P = .5); we did not observe any difference in residual radioactivity after 30 and 90 minutes.
Scintigraphy Results
NPP, nonpyloroplasty; PP, pyloroplasty.
Twenty-four-hour pH-metry
The results of the pH-metry test are listed in Table 5. No difference was observed in percentage of time with a pH <4 in both the esophagus and the gastric tube. Patients in the NPP group experienced a slightly smaller number of acid reflux episodes, without statistically significant difference (PP group 41.3 ± 10.7 versus NPP group 23.2 ± 9.5; P = .29)
Twenty-Four Hours pH-Metry Results
NPP, nonpyloroplasty; PP, pyloroplasty.
Discussion
The usefulness of a pyloric drainage procedure during esophagectomy is, till today, a matter of debate among upper GI surgeons, and even in very recent guidelines no specific recommendations on the role of pyloroplasty are provided. 15 Many articles focusing on this topic have been published, but their results are contradictory. In 2002, Urschel 16 published a meta-analysis of nine randomized controlled trials (RCTs), concluding that pyloric drainage procedures reduced the occurrence of early gastric outlet obstruction, even if the authors did not find difference in respiratory complications rate, anastomotic leak rate, and mortality. However, in a more recent meta-analysis, Akkerman 2 did not report differences in DGE or complications rate with or without a pyloric procedure. A possible explanation for these different results is that, in about half of the patients comprised in the RCTs analyzed by Urschel, the integrity of the digestive tract had been restored using the whole stomach, whereas in the most recent articles, a narrow gastric tube is usually preferred. According to several authors, when the whole stomach is used, the risk of DGE is higher compared with using a narrow gastric tube. 17 Interestingly, Arya 18 conducted a pooled analysis considering only articles published after 2000 (thus analyzing almost only patients with a narrow gastric tube), showing no difference in DGE and in complications. Other possible explanations for these contrasting findings are that most of the studies in the literature analyze together patients with different type/site of anastomosis (manual versus mechanical; cervical versus intrathoracic) and different reconstructive routes (retrosternal versus posterior mediastinal), which are probably equally important determinants of the functional outcomes after esophagectomy.
Moreover, almost all the studies analyzing the role of pyloroplasty have a short follow-up period and the main outcome usually considered are postoperative complications rates, especially the incidence of DGE. As a consequence, very little is known about the long-term functional status after surgery. However, this is a point of great interest since it has been proven that gastric tube mobility can recover even many years after surgery.19,20 It is important to remember that, as a consequence of the improved long-term prognosis of patient with esophageal cancer,21–23 long-term functional outcomes after surgery have become in the past years of primary importance too.
In our study, we tried to overcome some of the limitations of the previous literature. To have a cohort as homogeneous as possible, we analyzed patients treated with the same neoadjuvant protocol and were subjected to the same surgical operation, apart from the pyloric drainage procedure, by the same surgical team. Moreover, we investigated the long-term outcomes with subjective methods, by subjecting the patients to questionnaires to evaluate their perceived QoL but also with objective tests such as barium swallow test, scintigraphy, and 24-hour pH-metry.
In our patients, we did not observe significant differences between the two groups in terms of perceived QoL, as testified by the almost identical scores of the questionnaires.
In addition, the timed barium swallow test and the scintigraphy showed very similar results, being the mean area of the barium column at 1, 5, and 45 minutes and the residual activity at 30 and 120 minutes comparable between the groups. Interestingly, even if the difference was not statistically significant, patients in PP group experienced a number of episodes of acid reflux in the esophagus, double that in the NPP group (mean number of episodes per 24 hours was 23.2 ± 9.5 in the NPP group versus 41.3 ± 10.7 in the PP group, P = .29), and they had accordingly a longer mean time with pH <4 in the esophagus than patients in the NPP group (PP group 3.1 ± 2.1 versus NPP group 0.89 ± 1.6; P = .24). However, the mean time with pH <4 in the gastric tube, which can be considered as a surrogate for gastric remnant activity, 24 was comparable between the groups. In our opinion, this suggests that, after a long enough period since surgery, the gastric tube acid production, and probably its mobility too, recovers and that the patients who had not undergone a pyloric drainage procedure at least did not present long-term sequela in gastric emptying.
This study has some limitations. First, it is a retrospective single-center study comparing patients subjected to surgery over a long period and, as a consequence, patients in the PP group had a longer interval surgery tests. Consequently, it is possible that some late function recovery might have been observed among PP patients and not in the NPP group. Moreover, a selection bias exists, because only patients with no recurrence after a long period since surgery could have been analyzed. However, some of the limitations are also points of strength of the study, because we compared patients treated in the same way, by the same team. The result is that we analyzed the long-term outcomes of a homogeneous group of patients, in terms of operative (anastomosis site, technique, and route of reconstruction) and perioperative care. In addition, we chose to consider both subjective and objective parameters, to have an evaluation of the gastric tube function as wide as possible.
In conclusion, our results suggest that performing a pyloric drainage procedure during Ivor Lewis esophagectomy does not result in better long-term functional outcomes, in particular, with regard to gastric conduit emptying. Further studies are needed to confirm these findings.
Footnotes
Authors' Contributions
C.A.D.P. and J.W. gave substantial contribution to the conception, acquisition, and analysis of the study, contributed to drafting, and approved the final version of the article. L.G., L.A. and A.V. gave substantial contribution to the conception and analysis of the study and approved the final version of the article. S.G. and G.d.M. gave substantial contribution to conception and interpretation of the data, contributed to revising of the article, and approved the final version of the article.
Informed Consent
Informed consent was obtained from all patients included.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.