
Abstract
Objective:
This retrospective study aimed to present our surgical experience in patients with primary retroperitoneal tumors (PRTs) who underwent laparoscopic surgery and to compare the results with those of patients who underwent an open operation.
Materials and Methods:
We analyzed the medical data of patients who underwent retroperitoneal tumor resection through laparoscopic surgery or open operation between February 2014 and November 2019.
Results:
In total, 77 patients were enrolled. In total, 37 patients underwent open surgery and 40 patients underwent laparoscopic surgery. The tumor size in the open surgery group (10.2 ± 5.4 cm) was more significant than that in the laparoscopic surgery group (6.5 ± 3.1 cm) (P < .001). No difference was observed in operative time, blood loss, and transfusion between the two groups. Postoperative hospitalization in the open group (8.43 ± 2.77 days) was longer than that in the laparoscopic group (5.63 ± 2.16 days) (P < .001). The patients with PRTs in the IV area had minimal bleeding (16.67 ± 40.82 mL) and minimum postoperative hospitalization (3.83 ± 1.60 days).
Conclusions:
Laparoscopic resection of PRT is feasible in the selection of appropriate cases. The advantages are small trauma, light pain, quick recovery, and short hospital stay. It is especially suitable for benign PRTs with small size and cystic or small adhesion with vital organs or great vessels.
Introduction
A
Materials and Methods
The institutional review board of The First People's Hospital of Changzhou approved this study. Informed consent was not required for this retrospective study.
Patients and methods
We reviewed the medical records of patients who underwent surgery (both open and laparoscopic) for PRT between January 2014 and November 2019 at the department of general surgery of The First People's Hospital of Changzhou. Regarding preoperative radiologic assessments, abdominal computed tomography (CT) and/or magnetic resonance imaging (MRI) were performed based on the surgeons' decision. The demographic characteristics, symptoms, history of abdominal surgery, perioperative data, the nature of the tumor, and postoperative hospitalization were recorded and analyzed. First, patients were divided into an open group and laparoscopic group according to different types of surgeries to analyze. Then the patients in the laparoscopic group were divided into five groups according to the retroperitoneal area divided by the mesentery. The division of the retroperitoneal area (I, II, III, IV, and V area) is shown in Figure 1.
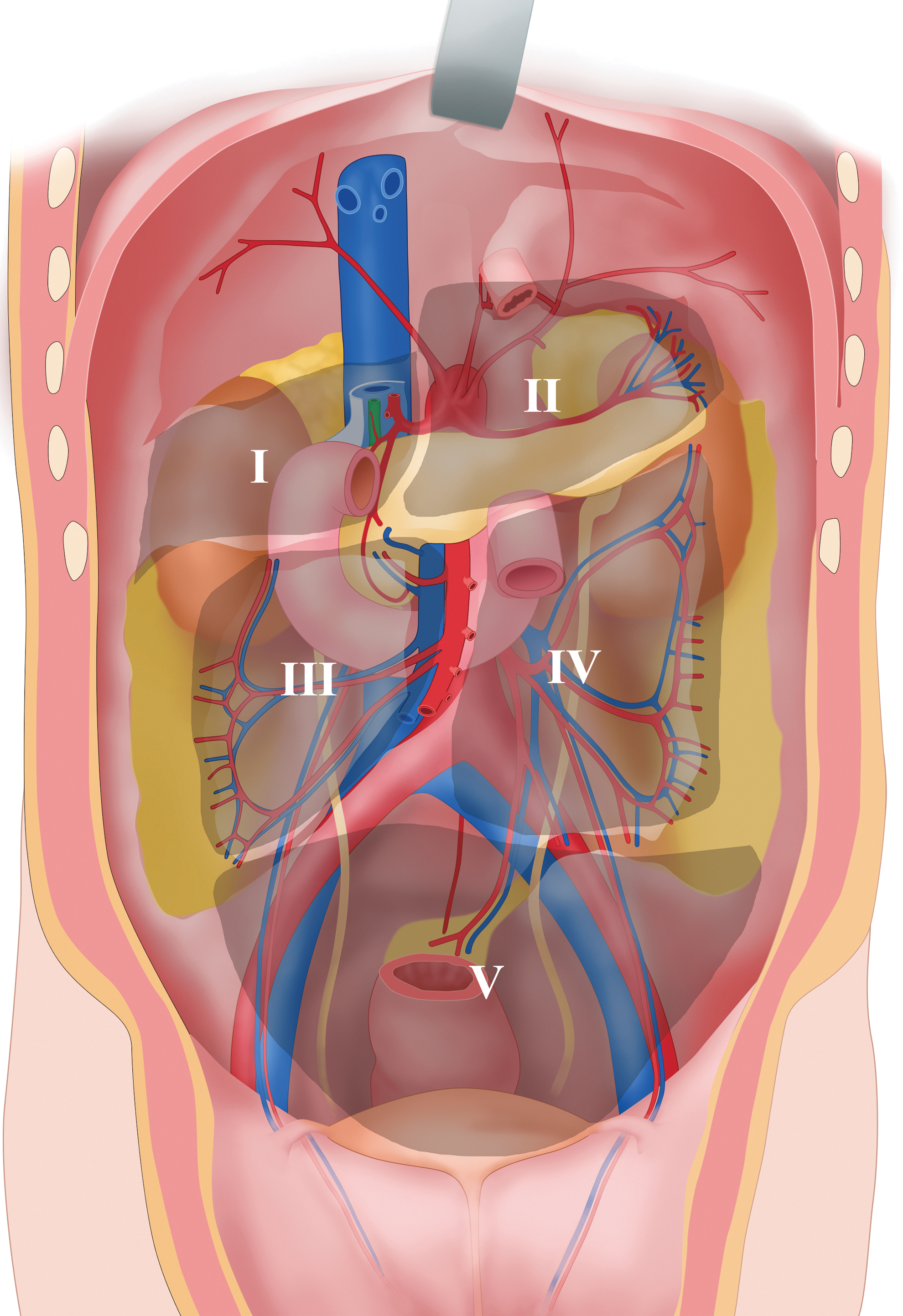
The division of the retroperitoneal area (I, II, III, IV, and V area).
Operative technique
The procedures were performed according to the results of CT or MRI before surgery. The primary considerations were the age and general condition of the patient and the size and location of the tumor. For open surgery, an abdominal midline incision was first selected for the operation. For laparoscopic surgery, the periumbilical region was preferred for observation. If the tumor was just below the umbilicus, the viewing hole was adjusted up and down along the median line to get the best view.
Statistical analysis
Statistical analysis was performed with SPSS 22.0 for Windows (SPSS, Inc., Chicago, IL, USA). For continuous variables, the differences between groups were analyzed by independent samples t-test. For categorical variables, the differences between groups were analyzed by the chi-square test. For all statistical tests, P < .05 was considered significant.
Results
Surgical outcomes
A total of 77 patients underwent resection of PRTs. Among them, 37 patients underwent open surgery and 40 patients underwent laparoscopic surgery. The characteristics of patients with PRTs are given in Table 1. There was no statistical difference in the characteristics for patients undergoing both open surgery and laparoscopic surgery, except for the tumor size. The tumor size in the open group (10.2 ± 5.4 cm) was more extensive than that in the laparoscopic group (6.5 ± 3.1 cm) (P < .001). As a result, 2 patients were converted to open laparotomy. All patients were discharged with no complications. The characteristics for the patients converted to open surgery in the laparoscopic group are given in Table 2. The 2 patients were both obese, with a history of abdominal surgery and with a sizeable solid tumor in the V area.
Characteristics of Patients with Retroperitoneal Tumors
The division of location (I, II, III, IV, and V area) is shown in Figure 1.
Continuity correction.
HOAS, history of abdominal surgery.
Characteristics of the Patients Converted to Open Surgery in Laparoscopic Group
The division of location (I, II, III, IV, and V area) is shown in Figure 1.
HOAS, history of abdominal surgery.
The perioperative data for open and laparoscopic retroperitoneal tumor resection are given in Table 3. No difference was observed in operative time, blood loss, and transfusion between the two groups. The postoperative hospitalization in the open group (8.43 ± 2.77 days) was longer than that in the laparoscopic group (5.63 ± 2.16 days) (P < .001).
Perioperative Data for Open and Laparoscopic Retroperitoneal Tumor Resection
Fisher's exact test.
The features and outcomes of PRTs undergoing laparoscopic surgery in different positions are summarized in Table 4. The patients with PRTs in the IV area had minimal bleeding (16.67 ± 40.82 mL) and minimum postoperative hospitalization (3.83 ± 1.60 days).
Summary of Retroperitoneal Tumors Undergoing Laparoscopic Surgery in Different Positions: Features and Outcome
The division of location (I, II, III, IV, and V area) is shown in Figure 1.
HOAS, history of abdominal surgery.
Discussion
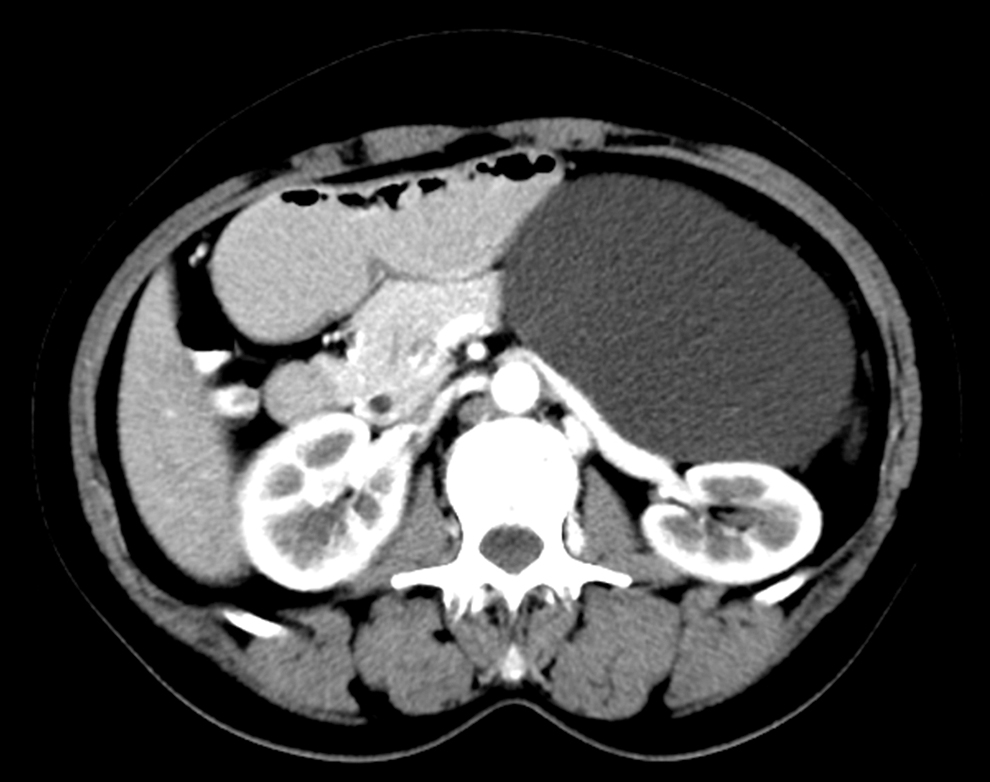
PRT is a complex and rare disease. It comprises different types of tumors that appear in different parts of the retroperitoneum. Owing to the low incidence and complexity of the disease, few studies have summarized it. 4 A few urologists divided the retroperitoneal space based on renal pedicle and para-aortic/paracanal vessel.1,2,5 Here as general surgeons, we divided the retroperitoneal space based on mesentery as shown in Figure 1. Tumors in the same region were similar in the design of the trocar holes. Such a method is suggestive for surgeons to flip abdominal contents and expose tumors during surgery. For instance, it is often necessary to conduct Kocher maneuver to flip the duodenum and pancreas when the tumor is located in the I or III area. The retroperitoneal space in the I area is small with relatively more and fixed organs. Moreover, the tumor is often closely related to the vena cava, as shown in Figure 2. The space behind the pancreas often needs to be exposed, when the tumor is located in the II area. The area behind the left/right colon may need to be revealed along the lateral peritoneum, when the tumor is located in the IV/III area.

The tumor in I area was closely related to the vena cava (arrow).
The normal anatomy of the retroperitoneum contains fascial planes, retroperitoneal compartments, and their contents. The retroperitoneal space is divided into three distinct compartments: the anterior pararenal space, the perirenal space, and the posterior pararenal space. 6 This classification scheme is beneficial for performing retroperitoneal laparoscopic management. 2 However, for transperitoneal laparoscopic management, the five-area method, as the partition method used by general surgeons, would be more appropriate.
The preoperative diagnosis of PRTs mainly depends on imaging examinations. In general, CT is usually the preferred workhorse for assessing the location and texture of PRTs. The relationship between the tumor itself and adjacent organs and blood vessels can be shown by CT vascular reconstruction, which is the key to the smooth operation. 7 As supplementary, MRI is used to evaluate the nature of tumors. 8 For example, MRI typically contains T1-weighted images (to assess fat, lymphadenopathy, and tumoral vascular invasion), T2-weighted fat-suppressed images (to assess lymphadenopathy, tumoral muscle invasion, cystic change, or necrosis, and bone marrow edema), and venous-phase contrast-enhanced T1-weighted images (to differentiate reliable from nonenhancing cystic or necrotic lesions).9,10
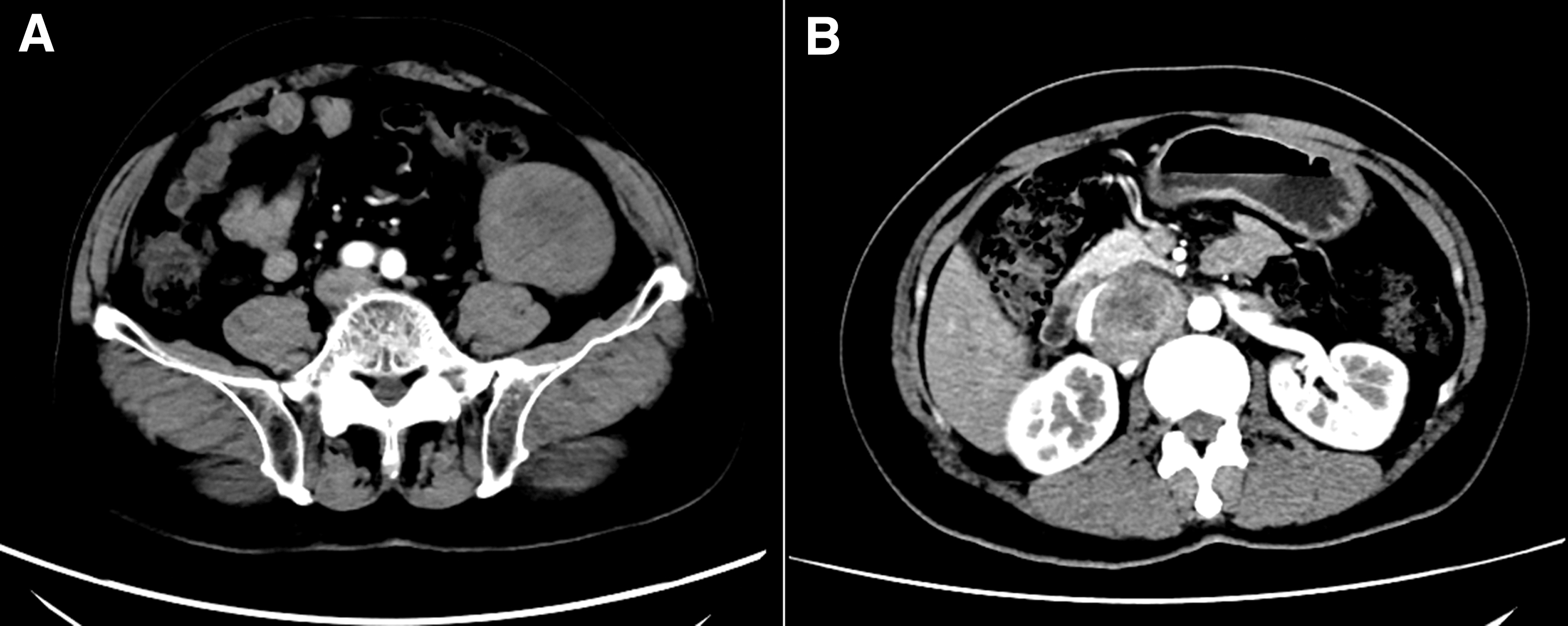
Preoperative imaging has a vital role in surgery. The limiting of tumor size for laparoscopic operation can be relaxed moderately when imaging findings strongly suggest benign cystic lesions. As shown in Figure 3, the cystic PRT in front of the left renal artery with 15 cm size was treated with laparoscopic management. For large cystic lesions, surgical decompression is beneficial for operation. For solid lesions, it is crucial to assess the edge of the tumors. As shown in Figure 4, although both tumors shown in Figure 4A and B were in the same area and depth, the envelope of the tumor shown in Figure 4B was not clear. It was indicative of unclear boundaries around the tumor, which was always high in fibers and nourishing vessels (Fig. 5A). During surgery, cellulose and blood vessels are sometimes indistinguishable from each other, so conservative ligation is the safest treatment (Fig. 5B, C). Laparoscopic surgery is preferred for tumors with a complete capsule (Fig. 4A, C). In addition to the integrity of the envelope, the relationship between the tumor and the surrounding blood vessels greatly influenced the difficulty of the operation. As shown in Figure 4D, the tumor is covered with several blood vessels, which may significantly increase the difficulty of laparoscopic surgery, and result in massive intraoperative bleeding.
A cystic primary retroperitoneal tumor was located in front of the left renal artery.
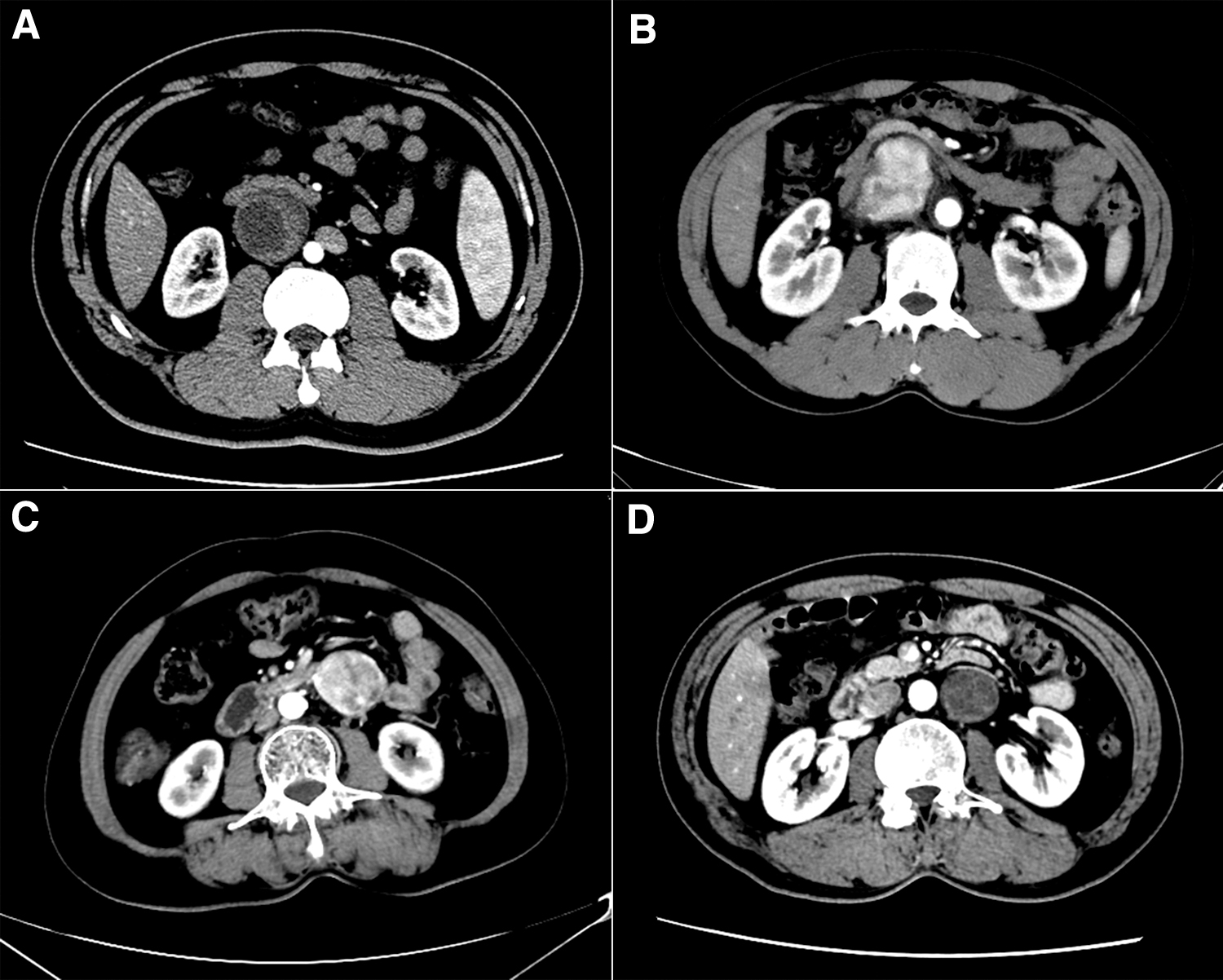
Imaging features of retroperitoneal tumors.

The condition surrounding the tumor during surgery.
In this study, we discover that surgeons are more likely to choose younger patients with small tumor size or cystic tumor for laparoscopic surgery, by comparison of clinical data between the two groups. Compared with retroperitoneal laparoscopic surgery, although transperitoneal laparoscopic surgery has a more extensive operation space, 11 the indications for it should be strict due to the interference of intraperitoneal viscera and the inflexibility of laparoscopic instrument, especially for the old patients with a history of abdominal surgery or with the big tumor. For some patients with tumors in the V area, the indications are stricter due to the narrow operation space in the pelvic cavity, as like the 2 patients who were transferred to laparotomy.
A retrospective study demonstrated that laparoscopy in comparison with open surgery was associated with a shorter postoperative hospital stay. 12 For the unique positional characteristics of PRTs, retroperitoneoscopic approach was used by some surgeons.13–16 Lee et al. demonstrated that posterior retroperitoneoscopic surgery was a safe procedure and the approach for small tumors can provide very favorable surgical outcomes compared with the transperitoneal approach. 13 In contrast to transperitoneal laparoscopic surgery, the key advantages of the retroperitoneal approach include direct accessing to the tumor, requiring little dissection without violating the peritoneal cavity. 14 However, many surgeons prefer the transperitoneal approach for the larger operating space, better vision, and more familiar anatomy. In addition, some researchers have proposed the use of single-port laparoscopic surgery, but this approach increases the difficulty of surgery and limits the indications for surgery. 17 This procedure is merely suitable for tumors of 3–4 cm in size, located around the umbilicus.
Laparoscopic resection of retroperitoneal malignancy is still controversial. 18 In this study, 2 cases of retroperitoneal malignant tumors underwent laparoscopic resection (both well-differentiated liposarcoma), and no recurrence or metastasis was found during a 3-year follow-up. Well-differentiated liposarcoma can be identified by preoperative imaging examination and is considered to be a low-grade malignancy with a good prognosis.19,20 We consider that for some malignant tumors with an intact capsule and no invasion of adjacent organs, laparoscopy itself does not increase the difficulty of surgery, as shown in Figure 6.
Imaging manifestations of malignant tumor.
There were several potential limitations to this study. First, this was a small retrospective study. Second, as already described, further follow-up is still needed to answer the question of whether laparoscopic surgery is feasible for malignant PRTs.
In conclusion, laparoscopic resection of PRTs is feasible in the selection of appropriate cases. The advantages are small trauma, light pain, quick recovery, and short hospital stay. It is especially suitable for benign PRTs with small size and cystic or small adhesion with vital organs or great vessels.
Footnotes
Acknowledgments
We thank all our colleagues at the department of hepatopancreatobiliary surgery, The Third Affiliated Hospital of Soochow University.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Natural Science Foundation of China (81971504), Post-Doctoral Special Foundation of China (2020M670065ZX), Post-Doctoral Foundation of Jiangsu Province (2020Z021), the clinical technology development foundation of jiangsu university (JLY20180079), Young Talent Development Plan of Changzhou Health Commission (CZQM2020118).