
Abstract
Aim:
To clarify the characteristics of patients with rectal prolapse after laparoscopically assisted anorectoplasty (LAARP), estimate the causes, and evaluate its impact on postoperative bowel function.
Methods:
The medical records of patients who underwent LAARP for high- or intermediate-type anorectal malformation between 2000 and 2019 were retrospectively reviewed. Clinical data were compared between patients with (Group P) and without prolapse (normal, Group N). Fecal continence was evaluated using the clinical assessment score for fecal continence developed by the Japanese Study Group of Anorectal Anomalies. For patients who underwent pelvic magnetic resonance imaging (MRI) before LAARP, atrophy, or asymmetry of the anal sphincter and levator ani was evaluated by a radiologist.
Results:
Of the 49 patients, 29 (59%) had rectal prolapse after LAARP (Group P) and 20 did not (Group N). We found no significant difference in gender, type of malformations, incidence of associated spinal or lumbosacral anomalies, procedure time, and postoperative bowel function at ages 4, 8, 12, and 16 years. However, LAARP was performed significantly earlier in Group N (median [range], 180 [123–498] days) than in Group P (210 [141–570] days). In Group P, 18 patients (62%) developed prolapse before colostomy takedown. Eight of 26 patients who underwent surgical prolapse repair required redo procedures. Twenty-five patients who underwent preoperative pelvic MRI showed no significant relationship between the muscular abnormalities and the incidence of postoperative rectal prolapse.
Conclusions:
Although recurrence is common, performing LAARP at a younger age might prevent postoperative prolapse development.
Introduction
Rectal prolapse is one of the common postoperative complications of anorectoplasty for anorectal malformations (ARMs). Laparoscopically assisted anorectoplasty (LAARP), which was introduced in 20001 and has been implemented widely, is no exception to the problem. Although both meta-analyses published so far concluded that the occurrence of rectal prolapse was comparable between the patients who had undergone LAARP and those who had undergone the conventional procedure,2,3 several studies showed that the incidence of rectal prolapse was higher in patients after LAARP (9.4%–50%) than in those after the conventional procedure (0%–29%),4–9 even though most of them showed no statistically significant difference. Moreover, clinical research in patients who suffered from rectal prolapse after LAARP remains scarce, and little is known about the characteristics, etiology, and relationship of bowel function with rectal prolapse after LAARP.
The aim of this study was to clarify the characteristics of patients with rectal prolapse after LAARP, estimate the causes, and evaluate its impact on postoperative bowel function.
Materials and Methods
Our hospital introduced LAARP as a standard procedure for repairing high- and intermediate-type ARMs in 2000. Our procedure was detailed previously 10 and some minor modifications were made over time, such as introducing an intraoperative measurement of the residual rectourethral fistula to cut the fistula flush with the urethra11,12 and creating the pull-through route using simple dissection of a “potential tunnel” in the muscle complex with a mosquito forceps and repetitive electrostimulation.13–15 We fixed the rectum from the perineum with four stitches between the pull-through rectum and the external sphincter but did not tack the rectum to the presacral fascia laparoscopically.
The medical records of the patients who underwent LAARP between 2000 and 2019 were retrospectively reviewed. Data on patient characteristics, such as gender; type of ARM; associated anomalies, including sacral deformity, spinal pathology, and mental disorder; age and weight at LAARP; and procedure time were collected. The occurrence of postoperative rectal prolapse was examined and if identified, the period from LAARP to manifestation of the prolapse, whether it occurred before or after stoma closure, the indication, timing, and type of surgical correction for rectal prolapse were also reviewed. Fecal continence was evaluated using the clinical assessment score for fecal continence developed by the Japanese Study Group of Anorectal Anomalies.4,16 The total score is 1–8, with higher scores suggesting better fecal continence, and is calculated as the sum of the urge to defecate (0–2 points), the smaller score of either constipation (1–4) or incontinence (0–4), and soiling (0–2). Clinical data, including postoperative fecal continence, were compared between patients with (Group P) and without prolapse (normal, Group N).
In our institute, pelvic magnetic resonance imaging (MRI) has been performed both pre- and postoperatively for all LAARP patients since we experienced cases with remnant of the original fistula in 200817 For those who underwent MRI before LAARP, atrophy or asymmetry of the anal sphincter and levator ani was re-evaluated by a radiologist who was given only the information that all images were obtained from patients with ARM and was blinded as to the presence or absence of postoperative prolapse.
Statistical analysis was performed by the Steel–Dwass method for nonparametric multiple comparisons and Fisher's exact test for contingency tables using a commercially available software (JMP_ Pro 11.0.0; SAS Institute Japan Ltd., Tokyo, Japan). P values <.05 were considered statistically significant. All data are shown as median (range).
This retrospective observational study was approved by the research ethics committee of Saitama Children's Medical Center, and the requirement for written informed consent was waived because of the retrospective nature of this study.
Results
Of the 49 patients who underwent LAARP during the study period, 29 (59%) had a rectal prolapse after LAARP (Group P) and 20 did not (Group N). The results of comparison between the two groups are shown in Table 1. No significant difference was found in gender, type of ARM, incidence of associated spinal or lumbosacral anomalies, and procedure time. However, LAARP was performed significantly earlier in Group N (median [range], 180 [123–498] days) than in Group P (210 [141–570] days). Postoperative bowel function assessed at the ages of 4, 8, 12, and 16 years was comparable between the two groups with no statistically significant difference (Fig. 1).
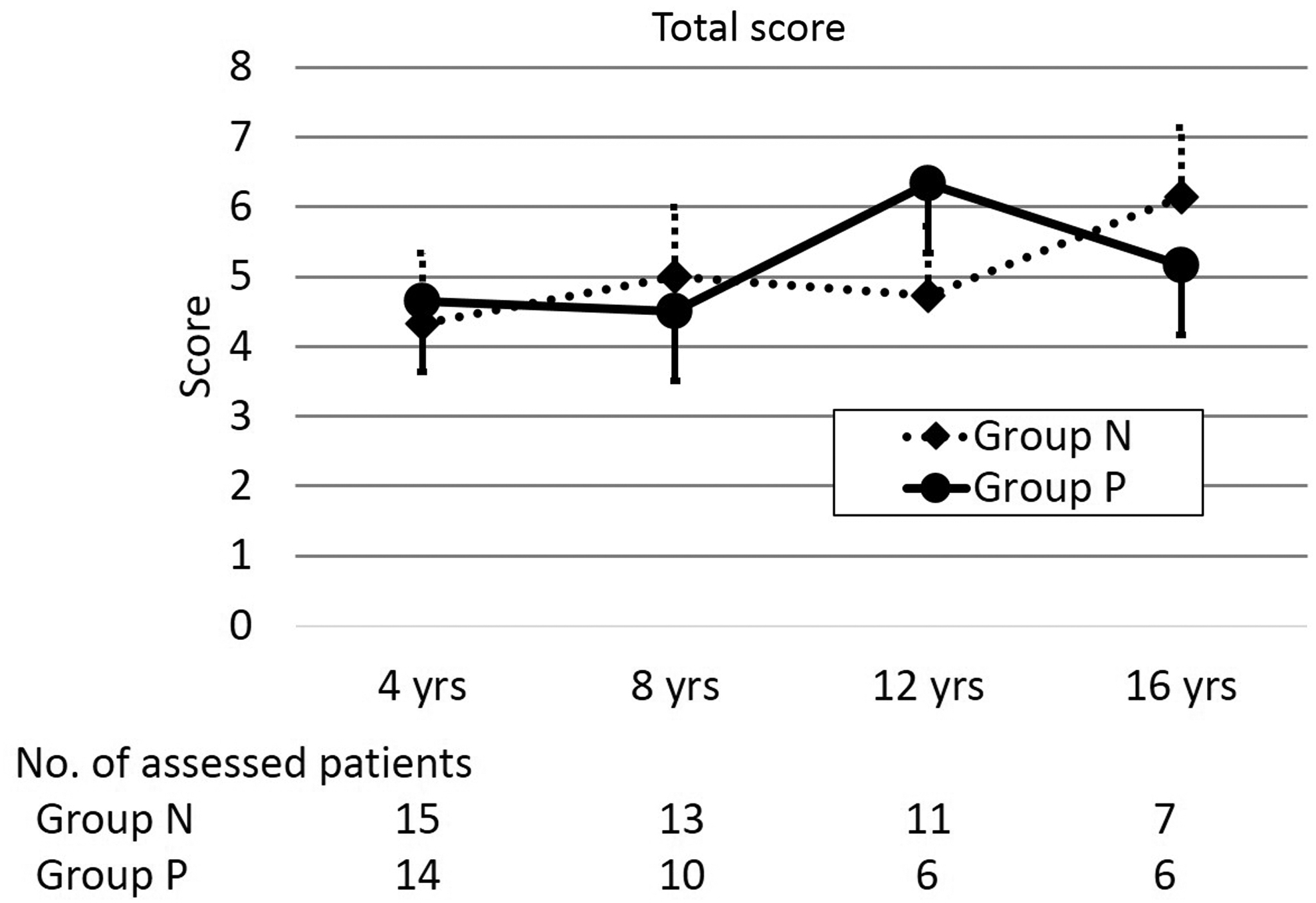
Total score of the clinical assessment for fecal continence. Group N, normal patients without prolapse; Group P, patients with prolapse.
Comparison of Patients With and Without Postoperative Rectal Prolapse
Group N, normal patients without prolapse; Group P, patients with prolapse.
The characteristics of patients with postoperative rectal prolapse (Group P) are summarized in Table 2. The median (range) onset was 20 (5–1130) days after LAARP, and 18 patients (62%) developed prolapse before colostomy takedown. Twenty-six patients (90%) underwent surgical prolapse repair, but 8 (31%) of them required redo procedures. Moreover, 2 out of those who underwent reoperation needed additional surgical correction. The indications for surgery varied from bleeding, increased prolapse size, stenosis, circumferential prolapse, incarceration, to mucous discharge. About one-third of patients underwent prolapse repair concurrent with stoma reversal. The procedures were decided by the surgeons' preferences and varied such as Gant-Miwa procedure, full-thickness resection, mucosal resection, and laparoscopic fixation.
Characteristics of 29 Patients with Rectal Prolapse After Laparoscopically Assisted Anorectoplasty
LAARP, laparoscopically assisted anorectoplasty.
The results of re-evaluation of the levator ani and anal sphincter in preoperative MRI by a radiologist and the association of the findings with the occurrence of prolapse after LAARP are shown in Tables 3 and 4. Among the 25 patients who underwent preoperative pelvic MRI, 22 (88%) and 12 (48%) had abnormalities (atrophy and/or asymmetry) of the sphincter muscle or levator ani, respectively. No significant relationship was found between the muscular abnormalities and the incidence of postoperative rectal prolapse.
Relationships of Postoperative Rectal Prolapse with Anomalies (Atrophy and/or Asymmetry) of the Levator Ani Detected by Magnetic Resonance Imaging
P = .55 (Fisher's exact test).
Relationships of Postoperative Rectal Prolapse with Anomalies (Atrophy and/or Asymmetry) of the Anal Sphincter Detected by Magnetic Resonance Imaging
P = 1.0 (Fisher's exact test).
Discussion
This study retrospectively reviewed the characteristics of patients with rectal prolapse after LAARP and compared them with those of patients without prolapse to estimate the cause, consider preventive measures, and evaluate its impact on fecal continence.
As a result, LAARP was performed significantly earlier in patients without prolapse than in those with prolapse. Our team made it a rule to perform LAARP on patients aged at least 6 months, and who weighed >6 kg. The detected time difference in performing LAARP was unexpected and may have happened by chance. However, this suggests that performing LAARP at a younger age can prevent postoperative rectal prolapse. An advancement of our treatment schedule for LAARP candidates much earlier would be feasible in future clinical practice because a Chinese group that performed LAARP in the neonatal period to repair the anomaly earlier achieved better outcomes and reported its safety and effectiveness.18,19
The definitive cause for postoperative rectal prolapse is unclear, but severe ARMs, poor muscle quality, tethered cord, vertebral anomalies, colostomy, and LAARP are considered to be risk factors for the prolapse.20,21 Our series did not show a significant difference in the spectrum of ARM types, lumbosacral deformity, and spinal pathology between the patients with and without prolapse. Meanwhile, more than half of our patients and about one-fourth of Brisighelli et al.'s cases 20 had rectal prolapse before colostomy closure and this implies that the prolapse might be caused by congenital or procedural factors rather than postoperative bowel control, including constipation. However, the preoperative MRI scans showed no relationship between the congenital abnormalities in the pelvic muscles and the incidence of prolapse, which is inconsistent with the findings of Belizon et al. 21 where intraoperative assessment revealed lower muscle quality in the patients with prolapse compared with that in patients without prolapse. Our higher incidence of prolapse might be attributed to the surgical technique.
The number of studies addressing the prevention and management of postoperative prolapse after LAARP is scarce, but some authors suggest that the length of rectal dissection tends to be longer in LAARP than in posterior sagittal anorectoplasty (PSARP), which might lead to a more frequent occurrence of rectal prolapse in LAARP compared with that in PSARP, and minimal rectal dissection might improve its incidence.7,22 The usefulness of laparoscopic anchoring stitches that fix the rectum to the presacral fascia has been reported,6,7,14 and Leung et al. reported that the application of anchoring stitches decreased the incidence of rectal prolapse after LAARP from 64% (9/14 cases) to 20% (4/20 cases). 23 In contrast, studies showing a higher incidence of postoperative rectal prolapse had a tendency of not tacking the rectum to the presacral fascia.4–9 Through this review, we began to incorporate laparoscopic suture rectopexy.
The indications and the optimal timing of surgical correction for postoperative rectal prolapse remain unclear. Our patients underwent surgical repair for various reasons, and asymptomatic cases were also included. Brisighelli et al. stated that symptomatic patients with a deteriorating quality of life should be considered for surgical treatment, but the application of surgical correction to asymptomatic patients is not recommended even if their prolapses are evident. 20 It is also debatable when to correct the prolapse. Jung et al. described that mucosal excision to correct the prolapse should be delayed until >6 months after LAARP, with expectations to adhere the rectum to the muscle complex. 22 However, Brisighelli et al. performed the prolapse repair before colostomy closure, even if the size of the prolapse was small, because the prolapse identified before colostomy closure often needs surgical repair later. Belizon et al. also recommended surgical correction before stoma reversal because the diversion of fecal stream assists wound healing. 21 Reported interventions for the prolapse varied, including hip bath with warm hyperosmotic saline, 9 injection sclerotherapy or submucosal injection of hypertonic saline, 24 Gant-Miwa procedure, 5 mucosal resection,5,23 full-thickness resection,5,20,21 Thiersch anal encircling procedure, 24 proctosigmoidectomy, 24 and laparoscopic posterior mesh rectopexy with concurrent perineal mucosal excision. 25 The pathogenesis of the prolapse after ARM repair might be different from that of rectal prolapse in adults due to anatomical abnormalities of the levator muscle and sacrum. 25 Although no ideal secure radical procedure for prolapse has been identified and acknowledged, the indication and appropriate timing of surgical correction are uncertain, and it is clear that the prolapse often relapses. In our series, approximately one-third of patients required redo surgery and others reported that recurrence is not so rare (9%–22%).20,21 Before surgery, surgeons should inform the patients' families of the relatively high risk of recurrence rate, 26 because surgery cannot remove all causative factors for prolapse development and only aims to eliminate symptoms.20,21
This study has a few limitations. Its sample size was small and the data were collected retrospectively. Fecal continence was similar regardless of having experience of postoperative rectal prolapse, but a further study would be needed to confirm this finding. In addition, we did not have a follow-up protocol for postoperative rectal prolapse, and we enrolled patients whose medical records described that prolapse occurred or mucosa was visible. Therefore, it was impossible to classify our patients using Brisighelli's criteria. Finally, preoperative MRI was not performed in all patients, and such patients were reassessed by a single radiologist who was well-versed in ARMs. These issues could have introduced bias to our data and findings.
Despite these limitations, this study showed that more than half the patients had rectal prolapse before stoma reversal, and congenital abnormalities of the levator muscle and the sphincter muscle re-evaluated by preoperative MRI did not correlate with the development of postoperative rectal prolapse. In addition, LAARP was performed earlier in patients without prolapse than in those with prolapse. Although the definitive cause of rectal prolapse after LAARP remains unexplained, performing LAARP at a younger age with concurrent laparoscopic rectopexy might be useful to prevent postoperative prolapse.
Footnotes
Acknowledgment
We thank Editage for English language editing.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.