
Abstract
Objective:
To evaluate rates of postoperative infection in patients with acute purulent appendicitis or gangrenous perforated appendicitis after laparoscopic appendectomy (LA).
Methods:
In this retrospective cohort study the medical records of patients who had undergone LA for acute appendicitis at Yijishan Hospital of Wannan Medical College between January 2015 and December 2019 were reviewed. The patients were divided into 2 groups based on the sequential order in which peritoneal irrigation, suction, and extraction of appendix had been performed. In Group 1 peritoneal irrigation and suction had been performed before extraction of the appendix, and in Group 2 they had been performed after extraction of the appendix. Demographic details, surgery duration, time to first flatus, length of hospital stay, total hospitalization expenses, and postoperative complications were analyzed.
Results:
The final study sample included 571 patients, 116 (20.3%) in Group 1 and 455 (79.7%) in Group 2. There were no significant differences in demographic characteristics, preoperative white blood cell counts, surgery durations, lengths of hospital stay, or total hospitalization expenses between the 2 groups (P > .05). Time to first flatus was significantly shorter in Group 1 (2.1 ± 0.5 days) than in Group 2 (2.3 ± 0.6) (P = .016), and the incidence of surgical wound infection was lower in Group 1 (6.9%) than in Group 2 (14.1%) (P = .038). There were no significant differences in the rates of intra-abdominal abscess, small bowel obstruction, or readmission within 30 days between the 2 groups (P > .05).
Conclusion:
Patients with acute purulent appendicitis or gangrenous perforated appendicitis are at high risk of surgical wound infection. Peritoneal irrigation and suction before appendix extraction may reduce the incidence of postoperative wound infection.
Introduction
Due to the associated advantages of shorter hospital stays, reduced postoperative pain, more rapid recovery times, and reduced superficial infection at the surgical site, laparoscopic appendectomy (LA) has replaced open appendectomy in recent years.1,2 Surgical site infections (SSIs) after LA do still occur in some cases, however. These SSIs are categorized as incisional or organ/space. SSI is the most common postoperative complication after LA, and it has been associated with prolonged operation times and increased medical expenses, and evidently affects patients' overall prognoses. 3
Most surgeons agree that the use of a retrieval bag can protect wound surfaces from direct contact with an infected organ and reduce the risk of wound infection.4,5 Some studies suggest that peritoneal irrigation and drainage can also reduce the incidence of surgical incision infection during surgery for acute appendicitis. 6 Determining risk factors for postoperative SSI may improve perioperative prognosis. Few studies have assessed surgical technique as a potential risk factor, thus, it is unclear whether the incidence of SSIs is related to the sequence of peritoneal irrigation and the use of a specimen bag. The aim of the current study was to investigate relationships between SSIs and the order of peritoneal irrigation and suction and the utilization of a specimen bag during surgery for acute appendicitis.
Methods
The medical records of patients who underwent LA for acute appendicitis at the Yijishan Hospital of Wannan Medical College from January 2015 to December 2019 were retrospectively reviewed. The diagnostic criteria for acute appendicitis were based on preoperative history, physical examination, and their postoperative pathology report. The exclusion criteria were postoperative pathology suggestive of other diseases of the appendix such as carcinoid of the appendix or appendiceal mucinous cystadenoma, and any other surgery performed during the operation to treat appendicitis (Fig. 1). This study was approved by the Institutional Review Board (IRB) of the Yijishan Hospital of Wannan Medical College.
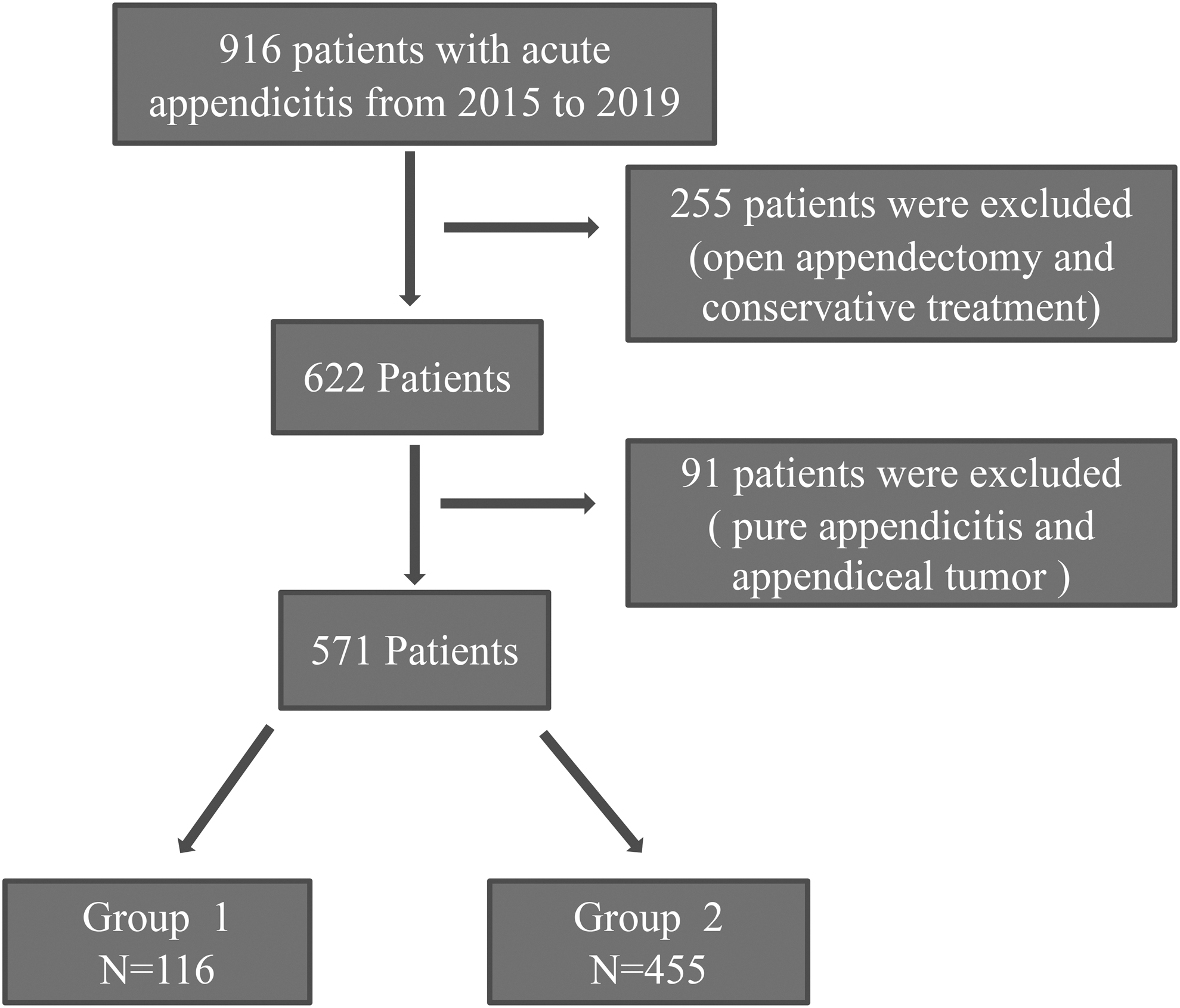
Flowchart of patients who underwent laparoscopic appendectomy from 2015 to 2019.
Based on the sequential order of peritoneal irrigation, suction, and the utilization of a specimen bag after treatment of the appendix stump during the operation, the patients were divided into 2 groups. In Group 1 peritoneal irrigation and suction were performed first then the appendix was retrieved using a specimen bag. In Group 2, the appendix was retrieved using the specimen bag first, then peritoneal irrigation and suction were conducted. The data obtained from patients' medical records included sex, age, appendicitis type, diabetes status, preoperative white blood cell count, degree of peritonitis, surgery duration, length of hospital stay, time to first flatus, total hospitalization expenses, and postoperative complications such as SSI, intra-abdominal abscess, small bowel obstruction, reoperation, and readmission within 30 days.
All patients were administered the antibiotics cephalosporin and metronidazole postoperatively unless they were allergic to cephalosporin, in which case they were administered quinolones and metronidazole. Intravenous antibiotics were ceased when the patient was afebrile and exhibited a normal white blood cell count. All patients were followed up for 1 month after discharge.
Surgical technique
LA was performed using a three-trocar protocol. The camera trocar (10 mm) was located at the umbilicus, the main operation trocar (10 mm) was located at the level of the umbilicus beside the right rectus abdominis, and the auxiliary operation trocar (5 mm) was located at the position of the anti-McBurney point. After entering the peritoneal cavity the pus was suctioned with an aspirator to prevent bacterial dissemination. The appendix mesentery was ligated with Hem-o-lok clips (Teleflex Medical) depending on the surgeon's preference. If the diameter of the appendix root was <10 mm, two Hem-o-lok clips were used. If the diameter of the appendix root was >10 mm, stitching with 3-0 absorbable suture was used. In Group 1, after treating the appendix root, the appendix was placed in the right iliac fossa, then the pus in the peritoneal cavity was irrigated and suctioned until the drainage fluid was clear. The appendix was then retrieved with a specimen bag through the incision of the main operation trocar, then the peritoneal cavity was irrigated and suctioned again until the drainage fluid was clear. In Group 2, the appendix was first retrieved with a specimen bag through the incision of the main operation trocar, followed by irrigation and suctioning in the peritoneal cavity until the drainage fluid was clear. A pelvic drainage tube was placed in all patients at the end of the operation, through the incision of the main operation trocar. The rinsing solution was 0.9% NaCl, and the irrigation volume was ∼500–1000 mL.
Statistical analyses
Student's t-test and Pearson's chi-square test were used for statistical analyses, which were conducted with SPSS version 22.0 (SPSS, Inc., Chicago, IL). P < .05 was considered statistically significant.
Results
Baseline characteristics
A total of 916 patients with acute appendicitis were initially screened for inclusion, of which 345 were subsequently excluded (Fig. 1), leaving a total of 571 patients who were included in the final analysis (Fig. 1). The final analysis sample included 253 male patients (44.3%) and 318 female patients (55.7%). Their mean age was 43.0 years (range 14–85 years), and there were 116 patients in Group 1 and 455 in Group 2. There were no statistically significant differences in sex, age, appendicitis type, diabetes status, white blood cell count, or degree of peritonitis between the 2 groups (P > .05) (Table 1).
Patient Characteristics in the Two Groups
WBC, white blood cell.
Perioperative and postoperative parameters
The mean time to first flatus in Group 1 (2.1 ± 0.5 days) was significantly lower compared with Group 2 (2.3 ± 0.6 days) (P = .016). There were no significant differences in surgery duration, length of hospital stay, or total hospitalization expenses between the 2 groups (Table 2).
Comparisons of Surgery Durations and Postoperative Parameters in the Two Groups
Postoperative complications
There were 8 cases of incision infection in Group 1 (6.9%) and 64 in Group 2 (14.1%), and this difference was statistically significant. There were no significant differences in the incidences of intra-abdominal abscess, small bowel obstruction, or readmission with 30 days between the 2 groups. No reoperation was performed in either group (Table 3). All patients with complications were successfully treated through dressing changes and antibiotic treatment.
Postoperative Complications in the Two Groups
Discussion
Acute appendicitis is the most common abdominal surgical emergency worldwide, 7 and the most common complication after appendectomy is SSI in the complicated appendicitis. Since the advent of LA, it has gradually become the standard operation for acute appendicitis due to associated advantages such as the reduced pain, more rapid recovery, and a lower rate of wound infection. 8 In patients with acute simple appendicitis there is no pus in the abdominal cavity, and incision infection and abdominal infection are comparatively less likely. Postoperative complications after surgery for acute purulent or gangrenous perforated appendicitis such as small bowel obstruction and SSI formation are reportedly associated with a high morbidity rate. 9 Talha et al. 10 reported that the incidence of wound infection after LA for perforated appendicitis was 8.3%. Realizing a reduction in the rate of SSIs and an improvement in the postoperative quality of life after LA has become a concern for surgeons.
After LA the appendix is usually retrieved by (1) extracting it directly through the 10-mm trocar, which is suitable if the diameter of the appendix and mesentery is <10 mm; (2) taking the specimens out directly through the incision if the appendix is too thick to be taken out through the trocar (this method is rarely used); and (3) using a specimen bag. In one single-center study, the risks of wound infection and intra-abdominal abscess were greater in patients who underwent LA without the use of a specimen bag. 11 In another study, SSI occurred in 80% of patients in whom a specimen bag had not been used. 12 Specimen bags can reduce the risk of postoperative intra-abdominal abscess and should be used in LAs. 5 Notably however, Turner et al. 4 reported that the method of retrieving the appendix with a specimen bag after appendectomy did not reduce the incidence of postoperative SSI. Despite this, we believe that a specimen bag should be used when retrieving the appendix after LA unless the diameter of the appendix and mesentery is <10 mm and the appendix can be retrieved from the trocar directly, for two main reasons. One pertains to the possibility of misdiagnosis, and the other pertains to the fact that if the diameter of the appendix is larger than the main operation trocar (10 mm), retrieval without a specimen bag will entail direct contact between the appendix and the incision, increasing the likelihood of SSI.
With regard to misdiagnosis, other diseases are sometimes present in patients with acute appendicitis before an operation intended to treat acute appendicitis is initiated. Some of these conditions are not readily apparent during the operation, such as appendiceal adenocarcinoma and appendiceal carcinoid, among others. If these conditions are not detected during the operation, extracting the appendix without using a specimen bag may result in iatrogenic implanting of the abdominal incision. Some surgeons use scissors in the peritoneal cavity to segment the appendix, then remove it through the trocar, but this could cause iatrogenic implantation of a malignant tumor derived from the appendix into the peritoneal cavity.
With regard to appendixes with diameters larger than that of the main operation trocar (10 mm), removal through that incision without a specimen bag will inevitably result in direct contact between the appendix and the incision, increasing the likelihood of SSI. Appendiceal carcinoid is often detected incidentally after appendectomy, through the subsequent pathology report. 13 In one study, the incidence of mucinous appendix was reportedly ∼0.29%–0.40% in all appendectomies. 14 In addition, Lobeck et al. 15 reported that 30 of 8382 patients (0.36%) who had appendiceal carcinoid underwent appendectomy. In the present study, 2 (0.35%) patients' postoperative pathology reports indicated acute purulent appendicitis with appendiceal carcinoid. Although the incidence of appendiceal tumors is very low, iatrogenic implantation during surgery can have disastrous consequences for patients. Therefore, in view of the abovedescribed reasons, we believe that a specimen bag should always be used when retrieving the appendix after LA, to reduce the occurrence of complications and improve the postoperative quality of life.
When specimen bags are introduced into the peritoneal cavity to take out the dissected appendix, there is a possibility of infectious complications associated with the use of the specimen bag. This is because the surface of the specimen bag may be contaminated by pus after it enters the peritoneal cavity, particularly if pus abounds in the peritoneal cavity. After a specimen bag becomes contaminated by pus in the peritoneal cavity, it will contaminate the incision site and increase the possibility of SSI when it is extracted. Therefore, we put the dissected appendix in the right iliac fossa and suction the pus out of the peritoneal cavity, then irrigate and drain the pus in the peritoneal cavity with saline—especially in the liver and kidney fossae, right iliac fossa, and the pelvic cavity—to reduce intra-abdominal pus.
Recent reports suggest that there is debate about whether to irrigate the peritoneal cavity. Some opponents argue that doing so may cause uncontaminated areas of the peritoneal cavity to become contaminated, 16 and in one study irrigation and suction reportedly increased the risk of postoperative complications and the duration of surgery. 17 Notably, peritoneal irrigation and drainage are still used by many surgeons. One meta-analysis suggests that peritoneal irrigation does not reduce the incidence of postoperative wound infection, intra-abdominal abscess, or the length of hospitalization during appendectomy. 18 Escolino et al. 19 reported that the use of peritoneal irrigation was associated with a lower rate of intra-abdominal abscess, but had no significant effect on wound infection. In the present study, peritoneal irrigation and suction using only saline solution was utilized. A drainage tube was placed into the pelvic cavity through the 10-mm trocar orifice. In the current study, in Group 1, intraperitoneal irrigation and drainage were performed both before and after the appendix was removed.
In the present study, irrigating and suctioning in the peritoneal cavity before appendix removal reduced the incidence of wound infection, and surgery times and total hospitalization expenses were not increased compared with the control group. We believe that this is because the total number of incision infections is not very large and does not have a significant effect on the outcome. Only 8/116 patients (6.9%) developed wound infection in Group 1 compared with 64/455 patients (14.1%) in Group 2, therefore irrigating the pus in the peritoneal cavity first can reduce the incidence of wound infection.
The current study was the first to comparatively investigate the effects of the sequence of abdominal flushing and appendix removal on SSI. The study had some limitations. It was a retrospective single-center study, and some patients who developed SSI after discharge may have been treated at a different local hospital. This may have affected the infection rate analyzed.
In conclusion, the results of the current study suggest that irrigation and suction before appendix removal is associated with a lower rate of SSI in patients who undergo LA.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.