
Abstract
Purpose:
Evaluate the clinical efficacy and safety of minimally invasive surgery (MIS) and open surgery in the treatment of neuroblastoma (NB) in children by a meta-analysis.
Materials and Methods:
This is a meta-analysis. We searched for random or nonrandomized controlled study of MIS group and OPEN surgery group for the treatment of childhood NB included in PubMed, ClinicalTrials, EMBASE, and Cochrane library before January 31, 2020. Data extraction was performed in a standard format for the included studies, including tumor diameter, operation time, intraoperative bleeding, length of hospital stay (LOHS), complications, recurrence, and MYCN.
Results:
Seven retrospective studies were finally included, with a total of 571 children, including 162 in MIS group and 409 in the OPEN surgery group. Compared with the OPEN surgery group, the MIS group had reduced intraoperative bleeding (mean difference [MD] = −12.72, 95% CI: −24.84 to −0.61, P < .05), and reduced l LOHS (MD = −3.35, 95% CI: −5.55 to −1.15, P < .05) and decreased postoperative recurrence (MD = 0.20, 95% CI: 0.05–0.75, P < .05). The differences between the groups were statistically significant. There was no significant difference between groups in tumor diameter (MD = −18.84, 95% CI: −48.12 to 10.43, P > .05), operation time (MD = −21.7, 95% CI: −97.52 to 54.13, P > .05), and MYCN results (odds ratio = 2.27, 95% CI: 0.56–9.18, P > .05).
Conclusions:
Preliminary evidence indicates that the treatment of NB with MIS has the advantages of less intraoperative bleeding, shorter LOHS, and less postoperative recurrence compared with open surgery.
Introduction
Neuroblastoma (NB) is the most common extracranial solid tumor in infants and young children, accounting for 8%–10% of malignant tumors in children. 1 Currently, treatment for children's NB include surgery, radiotherapy, systemic chemotherapy, and immunotherapy. 2
Whether the tumor can be removed safely and effectively is an important factor that affects the survival of children. The prognosis of children with NB is related to the risk stratification of the Children's Oncology Group. Children in the low-risk group can obtain a good prognosis only by surgery. Parikh et al. reported that the 3-year OPEN surgery rate of this group was close to 97%. 3 Children in the middle-risk group can also achieve a good long-term prognosis using a combination of surgery and chemotherapy. 4 The treatment of high-risk children is still controversial. Studies by De Ioris et al. have shown that local resection is safe and can prevent local recurrences. 5 However, other studies have shown that tumor resection does not have a substantial survival benefit. 6
Surgical methods of NB in children include minimally invasive surgery (MIS) and open surgery. MIS has the characteristics of less trauma and faster postoperative recovery. It has been widely used in many pediatric diseases such as appendectomy, fundoplication, bowel resection and anastomosis, and nephrectomy. 7 The earliest application of minimally invasive technology to children's malignant tumors was in the 1990s. After more than 20 years of development, MIS has gradually become popular among children's malignant tumors. However, the indications and therapeutic effects of MIS are still controversial. This meta-analysis aims to use the principles of evidence-based medicine to evaluate the safety and effectiveness of MIS and open surgery in the treatment of childhood NB, and provide a strong basis for the selection of clinical procedures.
Materials and Methods
Search strategy
According to the search strategy developed by Cochrane-assisted network, a combination of subject words and free words was used to search in the four databases of PubMed, ClinicalTrials, EMBASE, and Cochrane library with the following keywords: laparoscopic, thoracoscope, minimally invasive, surgery, and NB. The language restriction is English, and the search date is from the establishment of the database to January 31, 2020.
Inclusion criteria
The study included a comparison of MIS and open surgery in the treatment of NB in children.
Intervention measures include MIS and open surgery.
Include preoperative and postoperative information in children.
Types of study, including randomized controlled trials (RCT), cohort studies, and case-control studies.
Exclusion criteria
Abstracts without primary data, editors or expert opinions, reviews, case reports, and studies without control groups.
Studies that cannot extract data, such as poor quality, unclear, or incomplete comparative data.
Studies with the same data source or repeated research.
Unable to obtain full text.
Newcastle Ottawa Scale (NOS) scores <5.
Literature screening, quality assessment, and data extraction
Two researchers screened the literature according to the inclusion criteria and exclusion criteria by reading the title, abstract, and full text. After deleting duplicate, irrelevant, and unqualified literature, two researchers conducted quality assessment and data extraction independently. The NOS 8 was used to evaluate the literature quality. NOS, including selection (4 points), comparability (2 points), and exposure (3 points), with a full score of 9 points, of which 7 to 9 points is low risk (level A), 4 to 6 points is medium risk (level B), and 1 to 3 points is high risk (level C). Data extraction was carried out independently by two researchers and cross-checked. Insufficient data were contacted by the authors for supplementation. When there were disagreements, consultations with relevant experts and joint discussions were conducted to resolve them. Extracted content: the basic characteristics of the study, including the first author, year, source of literature, and study design; the baseline characteristics of the included cases, including age, gender, and weight; and the sample size of the study, intervention methods, preoperative status, outcome indicators, and follow-up time. The preoperative status include whether chemotherapy, radiation therapy, bone marrow transplantation before surgery, tumor diameter, International Neuroblastoma Staging System (INSS) staging, International Neuroblastoma Risk Working Group (INRG) staging, and risk grade. Outcome indicators include operation time, intraoperative bleeding, intraoperative residuals, complications, recurrence, length of hospital stay (LOHS), and 1–5-year survival rate.
Statistical analysis
Data analysis was performed with RevMan 5.3 software. First, heterogeneity tests were performed on each study (testing criterion P = .1). If P > .1, I2<50%, the heterogeneity among multiple studies can be considered small, and a fixed effect model is used; if P ≤ .1, I2 ≥ 50% that the heterogeneity among multiple studies is large, and a random effect model is used. Subgroup analyses of factors that may affect outcomes are performed if necessary. Observation index effects are measured by interval estimation and hypothesis test, continuous variables are expressed as mean difference (MD), and binary variables are expressed as odds ratio (OR) value. Calculate the 95% CI of the combined effect. When P ≤ .05, the difference between two groups was statistically significant. Publication bias was analyzed using a funnel plot.
Results
Literature search results and quality assessment
A total of 552 studies were retrieved in this study, including 199 in PubMed, 339 in EMBASE, 9 in Cochrane library, 0 in ClinicalTrials, and 2 were obtained through references. Three hundred fifty-three duplicate studies were excluded, 179 studies were excluded after reading the title and abstract, 13 studies were excluded after reading the full text, and 7 studies were included in this mete-analysis finally. All were retrospective case–control studies in English. The details of literature screening are shown in Figure 1. The quality assessment of seven studies is shown in Table 1.
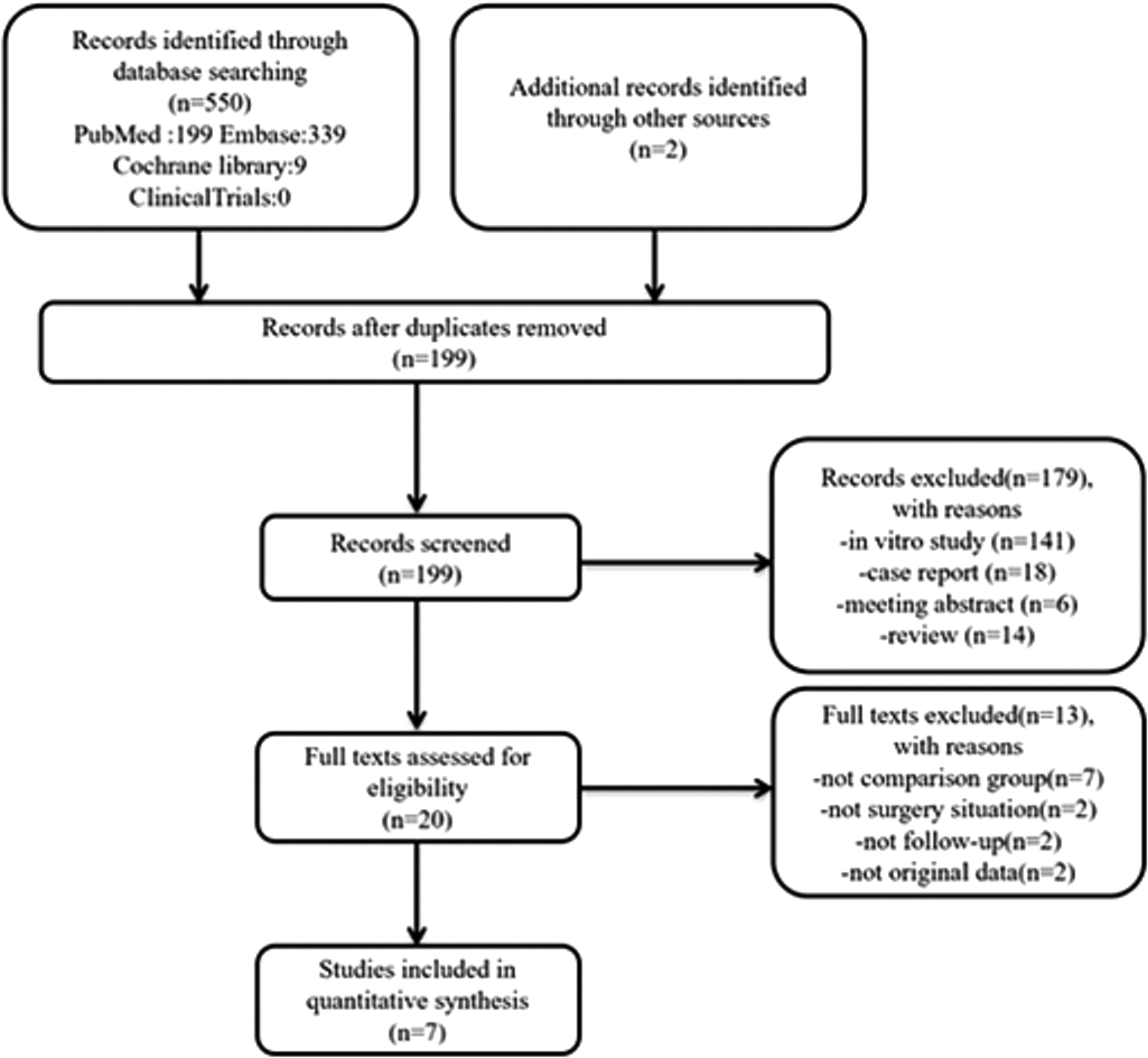
The flowchart of the meta-analysis.
Quality Assessment of the Inclusion of Study
General characteristics of the included studies
A total of seven original literatures were included in this study, with a total of 571 children, including 162 in the MIS group and 409 in the open surgery group (OPEN group). The characteristics of the included studies are shown in Table 2.
Summary of All Included Studies
Risk group: high (H), low/intermediate (L/I); INSS stage: I, II, III, IV; INRG stage: L1, L2, M, Ms; IDRFs: positive: +, negative: −.
Statistical differences between data (P < .05).
INRG, International Neuroblastoma Risk Working Group; INSS, International Neuroblastoma Staging System; LOS, length of stay; M, minimally invasive surgery; MYCN, N-myc proto-oncogene protein; N/A, not applicable.; O, open surgery.
Meta-analysis results
Clinical evaluation index
The meta-analysis statistics included clinical evaluation indexes such as tumor diameter, operation time, intraoperative bleeding, LOHS, recurrence, and MYCN.
Tumor diameter
A total of three studies reported the tumor diameter in children with NB in the MIS group and OPEN group. Meta-analysis results showed that there was statistical heterogeneity between the included studies (P < .00001, I2 = 98%), and a random effect model was used. The combined statistical analysis showed that there was no statistically significant difference in the tumor diameter before surgery between the two groups (MD = −18.84, 95% CI: −48.12 to 10.43, P > .05, Fig. 2).
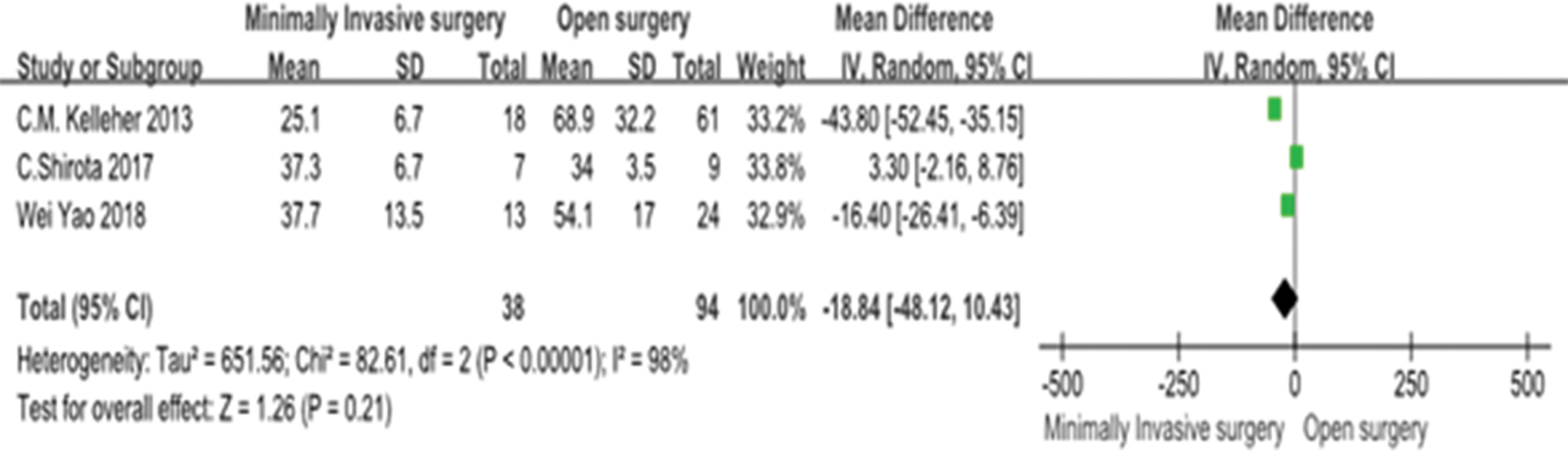
Forest plot of tumor diameter between MIS and open surgery. MIS, minimally invasive surgery. Color images are available online.
Operation time
A total of six studies reported the operation time of children with NB in the MIS group and OPEN group. Meta-analysis results showed that there was statistical heterogeneity between the included studies (P < .00001, I2 = 98%), and a random effect model was used. The combined statistical analysis showed that the difference in operation time between the two groups was not statistically significant (MD = −21.7, 95% CI: −97.52 to 54.13, P > .05, Fig. 3).

Forest plot of operation time between MIS and open surgery. MIS, minimally invasive surgery. Color images are available online.
Intraoperative bleeding
A total of four studies reported the intraoperative bleeding in children with NB in the MIS group and OPEN group. Meta-analysis results showed that there was statistical heterogeneity between the included studies (P < .00001, I2 = 92%), and a random effect model was used. The combined statistical analysis showed that the intraoperative bleeding of the MIS group was significantly reduced compared with the OPEN group, and the difference was statistically significant (MD = −12.72, 95% CI: −24.84 to −0.61, P < .05, Fig. 4).

Forest plot of operation bleeding between MIS and open surgery. MIS, minimally invasive surgery. Color images are available online.
Length of hospital stay
A total of five studies reported the LOHS of children with NB in the MIS group and OPEN group. Meta-analysis results showed that there was statistical heterogeneity among the included studies (P < .00001, I2 = 98%), and a random effect model was used. The combined statistical analysis showed that the LOHS of the MIS group was significantly reduced than the LOHS of the OPEN group, and the difference was statistically significant (MD = −3.35, 95% CI: −5.55 to −1.15, P < .05, Fig. 5).
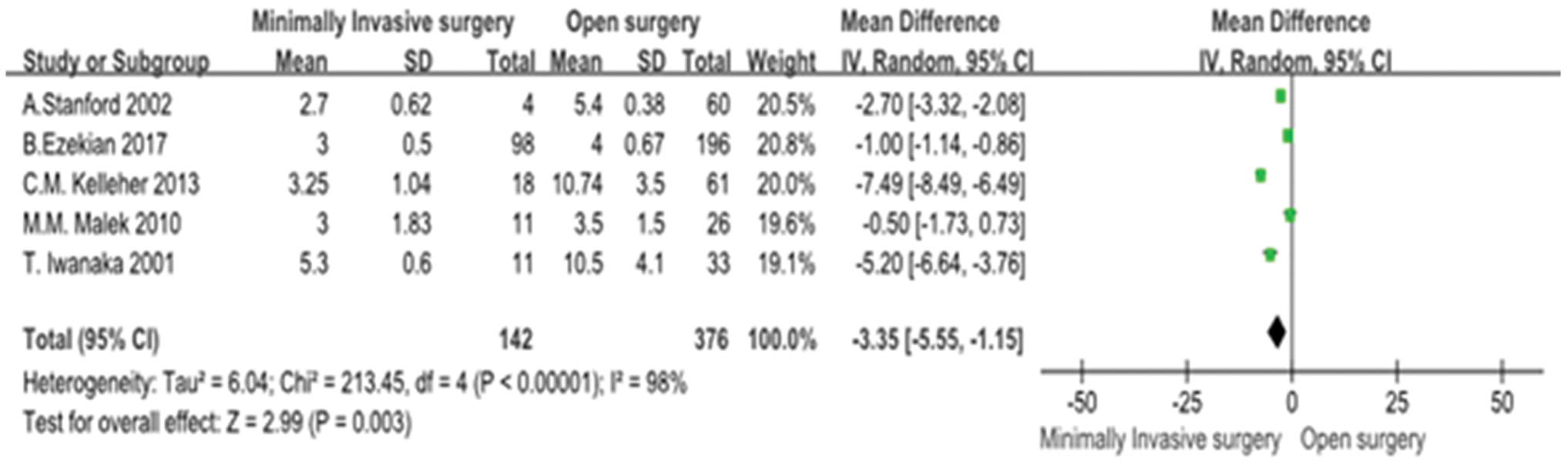
Forest plot of LOS between MIS and open surgery. LOS, length of stay; MIS, minimally invasive surgery. Color images are available online.
Recurrence
A total of four studies reported the postoperative recurrence in children with NB in the MIS group and OPEN group. Meta-analysis results showed that there was no statistical heterogeneity between the included studies (P = .71, I2 = 0%), and a fixed effect model was used. The combined statistical analysis showed that the postoperative recurrence in the MIS group was significantly reduced compared with the OPEN group, and the difference was statistically significant (MD = 0.20, 95% CI: 0.05–0.76, P < .05, Fig. 6).
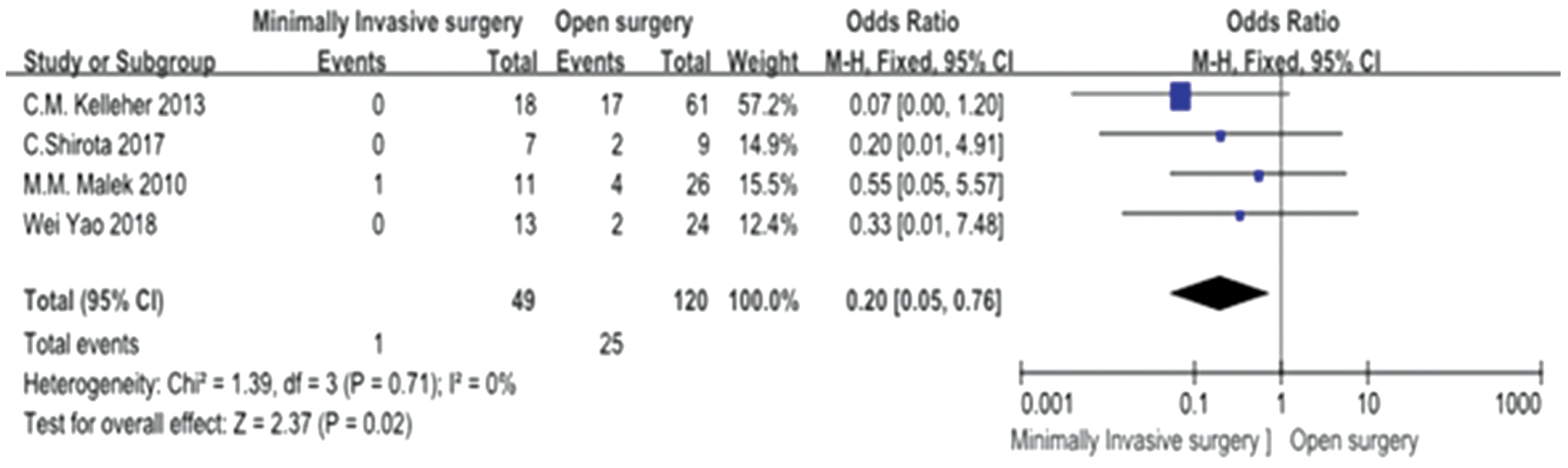
Forest plot of recurrence between MIS and open surgery. MIS, minimally invasive surgery. Color images are available online.
MYCN results
A total of three studies reported the results of MYCN in children with NB in the MIS group and OPEN group. Meta-analysis results showed that there was no statistical heterogeneity between the included studies (P = .34, I2 = 6%), and a fixed effect model was used. The combined statistical analysis showed that there was no significant difference between the two groups of MYCN results (OR = 2.27, 95% CI: 0.56–9.18, P > .05, Fig. 7).

Forest plot of MYCN between MIS and open surgery. MIS, minimally invasive surgery. Color images are available online.
Age of children
A total of five studies reported the age of children with NB in the MIS group and the open group. Meta-analysis results showed that there was statistical heterogeneity among the included studies (P = .04 < 0.1, I2 = 64%), and a random effects model was used. The combined statistical analysis showed that the children in the MIS group were significantly older than the open group, and the difference was statistically significant (MD = 11.74, 95% CI: 1.58–21.90, P = .02 < 0.05, Fig. 8).
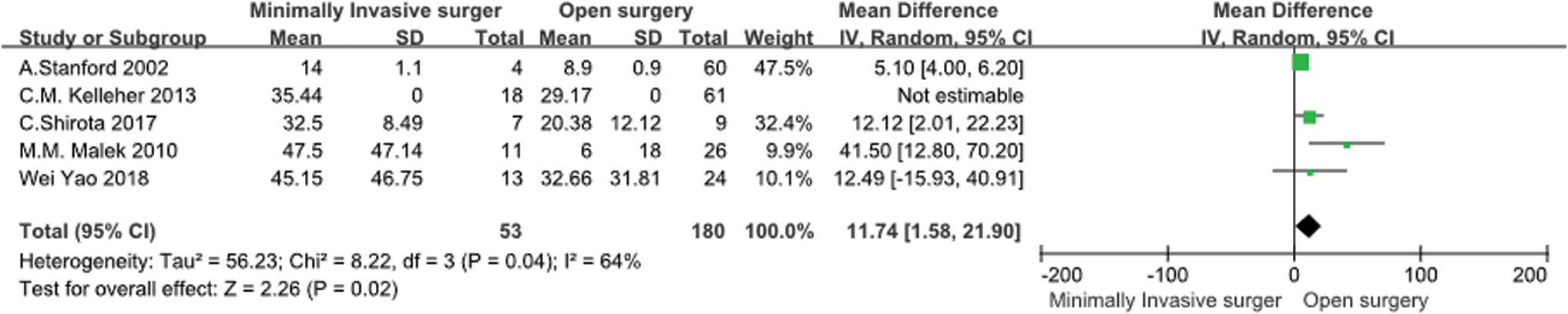
Forest plot of age between MIS and open surgery. Color images are available online.
Publication bias
The funnel plot does not show any obvious signs of publication bias (Fig. 9).
The risk of bias map (Fig. 10) and the summary risk of bias map (Fig. 11) suggest that there are defects in selection bias, which cannot be avoided in retrospective studies, but there is no obvious defect in publication bias.

Funnel plot of LOS

Risk of bias graph. Color images are available online.
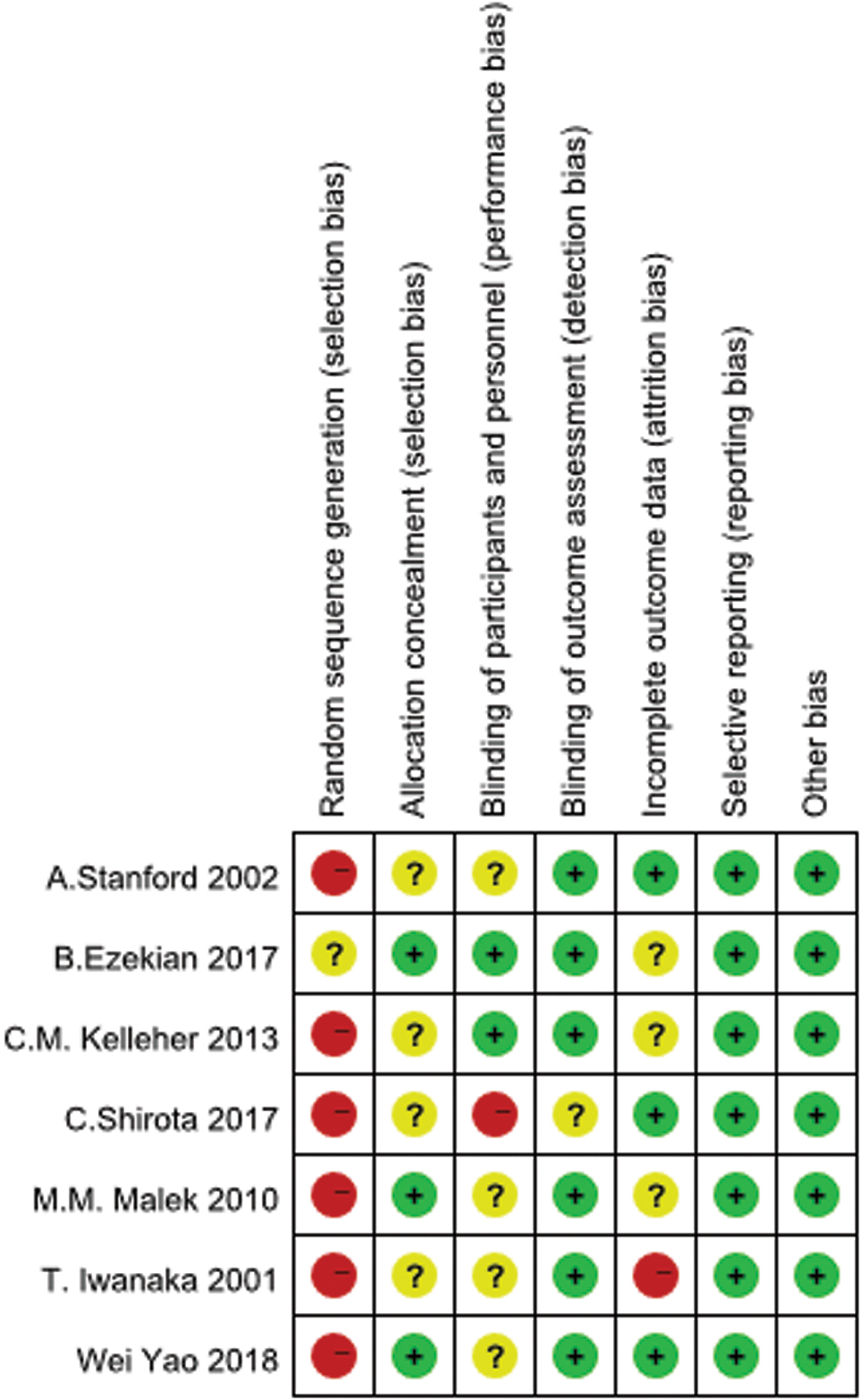
Risk of bias summary. Color images are available online.
Discussion
For most NBs, open surgery to remove the tumor is still the main procedure, but with the development of medical technology, doctors around the world are pursuing better results with less and less traumas. Nowadays, MIS is no longer an emerging technology, and adult surgery has widely applied minimally invasive techniques to many malignant tumors of solid organs.16,17 However, its application in children with solid tumors, especially malignant tumors, has been slow to be developed. The reason is that there is a lack of RCT or controlled clinical trials that comparing MIS with open surgery for the treatment of childhood malignancies. The deeper causes may be related to the low incidence of malignant tumors and the wide range of violations in children. van Dalen et al. 18 conducted a second review in the Cochrane database and still did not find enough evidence to support the application of MIS in children with solid tumors.
Only three studies reported the preoperative tumor diameter in the MIS group and the OPEN group in this meta-analysis. The statistical results show that there is no significant difference in the preoperative tumor diameter of the MIS group and the OPEN group. This result may be affected by the low number of included references. Our additional statistics found that the average diameter of the MIS group was 31.6 mm, and the average diameter of the open group was 61.7 mm. The results looked very different, but they were not statistically significant. The main reason was that the number of patients included was small. According to our clinical experience, the diameter of the tumor is relatively small in patients who can undergo laparoscopic surgery. It is reported in the literature that open surgery is less affected by the diameter of the tumor, but MIS is more affected by the diameter of the tumor. Iwanaka et al. 19 reported their experience in resection of abdominal NB in 2007. They believe that one of the indications for MIS is that the size of the tumor is between 4 and 6 cm. At the same time, Japanese scholars also set the size of the tumor up to 6 cm as the standard for minimally invasive removal of abdominal (including adrenal and retroperitoneal) tumors. 20 The International Pediatric Endoscopy Group also suggests a diameter of less than 6 cm as an indication of minimally invasive resection in the “Guidelines for the Surgical Treatment of Adrenal Masses in Children,” published in 2010. 21
At the same time, five studies reported the age of children with NB in the MIS group and the open group. The results suggest that the children in the MIS group are significantly older than the open group, and the difference is statistically significant. This result is in line with our habit of carrying out MIS. Older children have relatively large operating space, which reduces the difficulty of surgery to a certain extent. In addition, older children have matured organs and are more tolerant of surgery. At present, our center has carried out a lot of MIS of benign abdominal masses, many of which are also young, and some are newborns. Based on the experience of our center, there is no great difficulty in performing endoscopy in young children. Therefore, we believe that age should not be an obstacle to MIS of tumors. Of course, this also requires each center to choose according to its own technical conditions. This idea also needs further evidence-based medicine to support it.
Another widely reported indication for MIS is imaging-defined risk factors (IDRF) negative. In 2009, the INRG proposed a staging system (INRGSS) based on IDRF, aimed at predict the risk of surgery by staging NB in children without preoperative pathological results. 22 In 2011, INRG issued new guidelines for evaluating IDRF, which included “tumor only in contact with renal blood vessels” considered to be IDRF positive. 23 According to the new staging system, Italian scholars conducted a prospective one-arm study in 2014, 24 They used IDRF negative as an indication for MIS. The results showed that all children undergoing surgery did not develop serious complications. Only one minor bleeding occurred, no blood transfusion was required, and all operations were completed by MIS. There was no local recurrence, and distant transfer was observed after an average follow-up of 27 months. Therefore, they believed that if IDRF was negative or IDRF was negative after chemotherapy, MIS can be used to treat NB effectively. In 2016, another study showed 25 that the new guidelines increased the proportion of IDRF-positive patients from 31% to 71%, and also increased the sensitivity of IDRF to predict surgical complications from 47% to 100%, but the specificity decreased from 75% to 32%, and the accuracy decreased from 71% to 46%. They believe that the new guidelines will improve the stage of some children who can be safely cured only by surgery, and these children have not decreased the incidence of complications after receiving preoperative chemotherapy. Therefore, these Japanese scholars suggested conducting large prospective studies to verify the effectiveness of the new guidelines. In 2019, the Japan Childhood Cancer Group Neuroblastoma Committee (JNBSG) reported that the results of a prospective phase 3 clinical trial (JN-L-10) based on IDRF's surgical decision-making to treat low-risk NB can bring a good prognosis and reduced the incidence of long-term complications. 26 We are also trying to evaluate the impact of staging systems (including IDRF, INRGSS, INSS staging system) on the choice of MIS strategies for childhood NB. But as the staging systems used in various studies are not uniform, the available data are too small to make a meta-analysis. We regret about it.
It is well known that MIS not only causes less trauma and quick postoperative recovery after surgery but also expands the surgeon's field of vision, so that the deep local anatomy can be clearly observed. 27 The statistical results of this meta-analysis show that there is no significant difference between MIS group and OPEN group in the operation time of treatment of NB, that is, the operation time of MIS group is not higher than that of OPEN group, and the intraoperative bleeding and LOHS of MIS group significantly lower than that of OPEN group. This satisfactory result is closely related to the continuous practice of minimally invasive techniques by pediatric surgeons around the world in recent years. As the surgeon's proficiency improves in minimally invasive techniques, the surgical process increases, surgical trauma decreases, and accelerated postoperative recovery is reasonable. Some researchers believe that open surgery is usually performed in high-risk patients more than MIS, including nephrectomy, retroperitoneal or para-aortic lymph node dissection, partial resection of the liver or lungs, and so on. These procedures increase the operation time directly, so the operation time cannot be simply compared. 9
At the same time, some scholars also proposed the risk of MIS. Jacobi et al. 28 and Pentek et al. 29 reported the transfer of endoscopic incisions, but after improving the technique, none of the recently reported studies found the occurrence of endoscopic incision. Seven studies included in our research also did not find metastasis of endoscopic incision. Metzelder et al. 30 reported that in NB mice, CO2 pneumoperitoneum increased intrahepatic metastasis, but did not increase local recurrence. Reismann et al. 31 found in vitro experiments that simulating CO2 pneumoperitoneum significantly overexpressed C-MYC and HMGB-1 oncogenes in NB cells exposed to it, and reduced apoptosis, which affected. The behavior of tumor cells may increase the malignancy of tumor cells. In addition, early MIS cannot completely remove the tumor, which is also considered a major disadvantage. Although some studies believe that resection range of ≥90% can significantly improve event-free survival, 32 other studies have found that complete resection in advanced children does not significantly improve OPEN surgery. 5 The German scholar Decarolis 33 does not advocate complete radical resection of the tumor, and even suggests that tumor remnants <2 cm are acceptable. The statistical results of this meta-analysis show that the postoperative recurrence in the MIS group is significantly reduced compared with the OPEN group, which is consistent with the report of Luo et al. 32
Our study showed that the MYCN amplification results of the MIS group are not significantly different from the OPEN group, excluding the impact of MYCN on the prognosis. MYCN exists in a haploid state in normal human cells, it can promote cell proliferation, inhibit cell differentiation, and apoptosis. Studies by Kang et al. 34 and Woo et al. 35 show that reducing the expression of MYCN can induce cell differentiation and apoptosis, thereby inhibiting the growth and proliferation of tumor cells. MYCN is widely involved in the occurrence and development of NB, and MYCN gene amplification is more common in advanced high-risk children. The treatment effect of such children is poor. Studies by Anderson et al. 36 showed that MYCN gene amplification was negatively correlated with the prognosis of most children. Therefore, drugs targeting the MYCN gene are under development, and the amplification of the MYCN gene is listed as one of the high-risk factors in the clinic.
For the publication bias of our study, we produced a funnel chart (Fig. 9) and found no obvious publication bias. At the same time, we also used the Cochrane risk bias assessment tool to conduct an overall bias evaluation, and produced a bias risk map (Fig. 10) and a bias risk summary map (Fig. 11). The results show that although there is selection bias, there is no obvious flaw in report bias. Because the included studies are all retrospective case-control studies, selection bias definitely exists, which also leads to a low level of evidence for the results, but combined with the current analysis we have done, the results of this study are credible. This result also suggests that pediatric surgeons can continue to conduct more in-depth research in the field of MIS of pediatric solid tumors, such as exploring surgical indications and conducting multicenter prospective RCT.
In summary, the preliminary evidence of this meta-analysis shows that compared with open surgery, MIS for NB has the advantages of less intraoperative bleeding, shorter hospital stay, and less postoperative recurrence. In view of the limited number of studies included in this meta-analysis and the studies are all retrospective, the above conclusions may have certain selection bias and publication bias, and further multicenter prospective RCT are still needed to confirm it.
Footnotes
Disclosure Statement
No competing financial interests exist.
Level of evidence: Level III.
Funding Information
There is no financial support for this study.