
Abstract
Background:
Anastomotic leak (AL) rates gradually decreased with surgical skills and perioperative management progression, but it is still inevitable. As the traditional management of AL after the pull-through procedure of Hirschsprung's disease (HD), enterostomy could lead to multiple surgeries, repeated hospitalizations, increased costs, and enterostomy-associated complications. This study aimed to explore the safety and feasibility of resuturing without enterostomy treating early AL after the laparoscopic Soave procedure.
Methods:
From October 2014 to June 2019, 10 patients who had AL after the laparoscopic Soave procedure were included. Six patients underwent simply resuturing with presacral drainage; the reoperation time was 1–5 days after primary surgery. Four patients who had diffused peritonitis or severe inflammations received resuturing with an ileostomy, and the reoperation time was 6–11 days.
Results:
Common early symptoms of AL included persistent fever, sacrococcygeal pain, and abdominal pain. The median delay to reoperation was 1.0 (0–2.25) day. Five patients had leaks at the 3–6 o'clock position, two had leaks at the 6–9 o'clock, and the other three had leaks at the 6 o'clock. The median postoperative fever durations were similar in patients without or with an ileostomy, and the median length of intensive care unit (ICU) stays, duration of antibiotic use, and postoperative length of stay were significantly longer in patients with ileostomy. The mean follow-up time was 38.5 ± 16.7 months (15–69 m). As of the time of writing, no reoccurrence was identified.
Conclusion:
For patients without diffuse peritonitis, severe inflammations, early diagnosis and timely resuturing of AL within 5 days after the laparoscopic Soave procedure of HD could be a safe, effective, and pleasing treatment.
Introduction
Orvar Swenson and colleagues first developed the open pull-through surgery to treat Hirschsprung disease (HD) patients in 1948. In recent years, several modified techniques such as laparoscopic-assisted, transanal, and robotic-assisted surgery have been widely used in many centers, which lead to better prognoses.1–6 However, even for experienced surgeons, postoperative complications are inevitable. 7 Anastomotic leak (AL) is one of the most severe postoperative complications of HD, which may cause life-threatening abdominal cavity infection. 8 AL in postoperative HD patients has an incidence ranging from 1.3% to 8% and is more commonly seen in neonates or delayed diagnosed older patients.9,10 Persistent fever, sacrococcygeal pain, abdominal pain, bloody stools, abdominal distension, and vomiting are common symptoms of AL patients.
At present, the traditional management is enterostomy, which could avoid contamination of stools with anastomoses and the leak would heal spontaneously. However, enterostomy has several disadvantages, including multiple surgeries, repeated hospitalizations, increased hospital costs, growth failure, and enterostomy-associated complications.11–14 Chronic presacral sinus formation or retraction of the pull-through bowel would also appear in AL patients after enterostomy, which also increased the difficulty of the redo surgery.13,15 In the era of minimal invasive surgery, people have higher requirements for beauty, while enterostomy is usually associated with poor cosmetic appearances.
Although resuturing challenges the traditional view that inflammation will cause unhealing anastomoses, previous studies have established the feasibility of resuturing in patients who had AL after pull-through procedure. Jester et al. performed an early postoperative rectoscopy and resutured clinically asymptomatic AL patients after primary surgery, while Peng et al. performed a diverting enterostomy covering the resutured anastomosis.16,17 Whether resuturing for early symptomatic AL patients without enterostomy is practicable remains largely undefined. This study summarizes the treatment experiences of AL occurred after the pull-through procedure and provides new insights into the safety and feasibility of resuturing without enterostomy in treating early-stage symptomatic AL patients after laparoscopic Soave procedure in HD.
Materials and Methods
Study design and patients
This was a retrospective single-center study approved by the Research Ethics Board of the Union Hospital, Tongji Medical College, Huazhong University of Science and Technology (number: 2016[S180]).
According to the 1991 United Kingdom Surgical Infection Study Group, AL was defined as the leak of luminal contents from a surgical joint between two hollow viscera. Patients were diagnosed by clinical manifestations, regular blood tests, ultrasound, or intraoperatively. Between October 2014 and July 2019, a total of 416 patients were diagnosed with HD and underwent laparoscopic Soave procedure in our center; among them, 352 were rectosigmoid HD, and 64 were long-segment HD. Thirteen postlaparoscopic Soave pull-through procedure AL patients (11 from our center and 2 referral patients from other centers) were treated in our center (Fig. 1). Two patients who had AL after redo-surgery and one patient who had anastomosis ischemia were excluded. Finally, 10 patients were included.
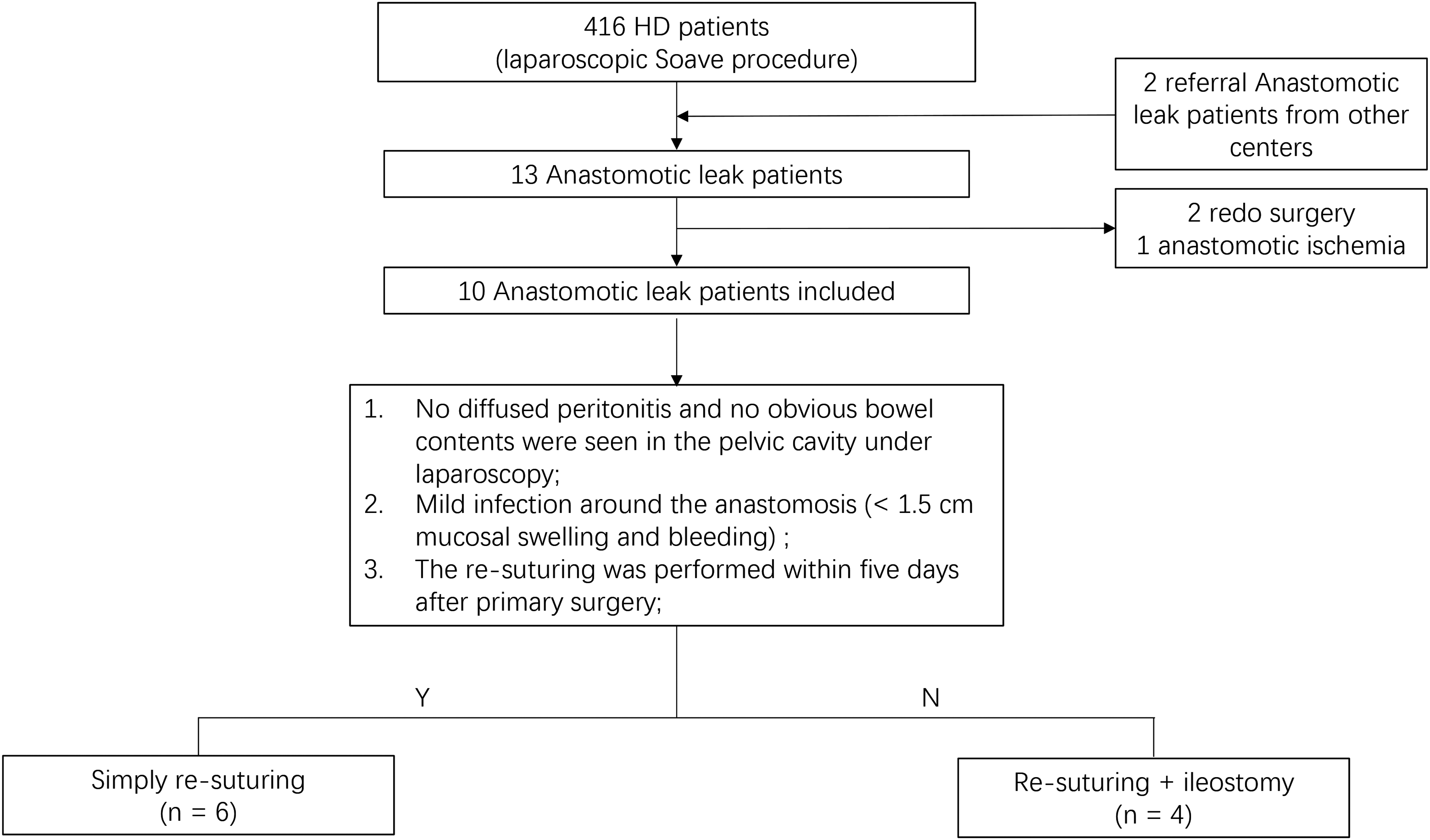
The inclusion and treatment protocol. HD, Hirschsprung disease.
Once patients showed persistent postoperative fever or repeated fever, sacrococcygeal pain, abdominal pain, elevated white blood cell count, elevated C-reactive protein (CRP) level, or ultrasound showed retrorectal or pelvic pneumatosis or fluid collection. Anastomosis examinations with colorectal retractor (Lone Star, US, Cooper Surgical) under anesthesia would be performed. If AL were identified under direct vision, resuturing with or without ileostomy would be performed directly. Laparoscopy was used to observe the pelvic cavity and determine whether an ileostomy should be performed.
Six patients underwent simply resuturing with presacral drainage; the reoperation time was 1–5 days after primary surgery. Four patients who had diffused peritonitis or severe inflammations received resuturing with an ileostomy, the reoperation time was 6–11 days. The medical records of the 10 included patients were reviewed, including HD type, age at surgery, sex, onsets of symptoms, reoperation time, postoperative fever duration, postoperative length of stay (LOS), abdominal ultrasound findings, and laparoscopic abdominal exploration findings.
Surgery plan and postoperative treatments
Laparoscopic-assisted Soave pull-through procedure
A three-trocar endorectal Soave pull-through technique was used. Also, the detailed surgical plan was described in a previously published article. 18
Treatment strategy of ALs
Patients who met all the following three criteria received simply resuturing with presacral; otherwise, resuturing with an ileostomy would be performed. (1) Patients did not show any symptoms of diffused peritonitis and no obvious bowel contents were seen in the pelvic cavity under laparoscopy. (2) The infection around the anastomosis was mild (defined as those with <1.5 cm mucosal swelling and bleeding). (3) The resuturing was performed within 5 days after primary surgery (Fig. 1).
The resuturing procedure was performed as follows. The patient was placed in the lithotomy position with the buttocks elevated. A colorectal retractor (Lone Star, US, Cooper Surgical) was used to open the anus. Hydrogen peroxide and physiological saline were used to irrigate the region around the anastomoses, and the retrorectal space and the pelvic cavity. We cleared tissues with poor blood supply at the anastomosis and irrigated the abdominal and pelvic cavity by laparoscopic visualization through the same ports as the primary surgery. Then, the anastomotic dehiscence was resutured transanally using 3–0 or 4–0 Vicryl. Patients with severe inflammation or peritonitis received double-barrel terminal ileostomy. Presacral drainage was placed from the abdomen by laparoscopy.
The urinary catheter was removed after 24–48 hours, and patients received 5–7 days of intravenous antibiotics postoperatively. Patients received intravenous total parenteral nutrition for 7–10 days. The diet will be changed from deep hydrolyzed formula to normal gradually. Patients with ileostomy received stoma closure 4–8 months later.
Recovery criteria and follow-up
Recovery of AL was identified when patients met the following criteria. (1) No extravasation of bowel contents or gas through the drainage. (2) No fever (<37.5°C). (3) Normal regular blood tests and CRP results. (4) Rectal examination: the examiner's finger could smoothly go into the rectum, and the anastomosis was smooth without leaks or dehiscence. (5) Barium enema showed no contrast agent spill from the bowel.
Statistical analysis
The data were analyzed by SPSS 26.0. The data were reported as mean ± standard error of the mean or median (interquartile range) and were compared using independent samples t-test; P < .05 was used to determine significance.
Results
Our clinical practice of resuturing started from a 28-month-old patient, who had fever, abdominal pain, and anal pain on the second day after surgery. Emergency surgery was performed, and loose sutures were found at the 3–6 o'clock position intraoperatively. The inflammation was localized and mild, and no bowel contents were seen in the pelvic cavity under laparoscopy. Therefore, resuturing was performed, and presacral drainage was placed from the abdomen. The patient had an uneventful healing and was discharged after 15 days.
Table 1 shows the demographics and postoperative outcomes of AL patients. The average age at surgery was 36.7 months, and 60% of the included patients were male. The median delay to treatment was significantly shorter in patients without ileostomy than patients with ileostomy (0.5 vs. 2.5, P = .009). Positive findings identified by abdominal ultrasound suggesting AL, such as retrorectal or pelvic pneumatosis or fluid collection, were only identified in 40% of patients. Five of the six patients who underwent simply resuturing did not have intestinal contents in the pelvic cavity, some bowel contents were seen in the pelvic cavity of one patient. For four patients who received resuturing after five postoperative days, bowel contents were found in the pelvic cavity of three patients. After separation of the adhesion around the rectum, bowel contents were found in the pelvic cavity in another patient with severe inflammation around the anastomosis. Ileostomy was performed in these patients.
Demographics and Postoperative Outcomes of Anastomotic Leak Patients
HD, Hirschsprung disease; LOS, length of stay.
Five patients had leaks at the 3–6 o'clock position, two had leaks at the 6–9 o'clock position, and the other three had leaks at the 6 o'clock position. Table 2 shows that the postoperative fever durations were similar between two groups. The median length of intensive care unit (ICU) stays, duration of antibiotic use, and LOSs were significantly longer in patients with ileostomy. Two of the 10 patients had complications after resuturing. One patient who underwent simply resuturing had anastomosis stenosis. With the help of daily anal dilation, the obstructive symptoms relieved after 1 month. Another patient who underwent resuturing with an ileostomy had stoma prolapse. The average follow-up time was 38.5 ± 16.7 months. As of the time of writing, no reoccurrence was identified.
Differences in Postoperative Outcomes of Anastomotic Leak Patients Who Underwent Different Surgeries
Significant differences, p ≤ 0.05.
ICU, intensive care unit; LOS, length of stay.
Table 3 shows the specific presenting symptoms of the 10 patients. Common symptoms included persistent fever (>39°C), abdominal pain, sacrococcygeal pain, abdominal distension, and bloody stools. All 10 patients showed persistent fever, followed by abdominal pain (90%) and sacrococcygeal pain (90%).
Presenting Symptoms of Anastomotic Leak Patients
Figure 2A shows an AL at the 3–6 o'clock position with mild inflammation on postoperative day 5. Figure 2B shows the appearance of anastomosis after resuturing.
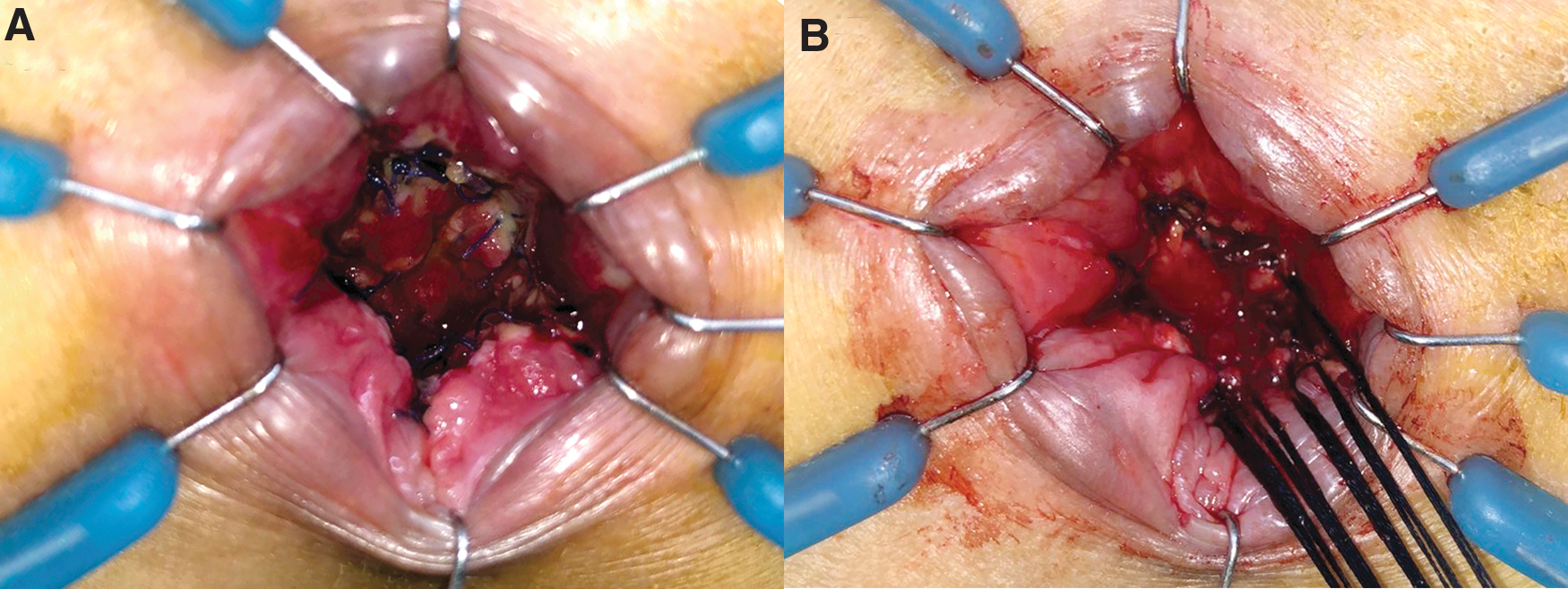
Resuturing of the AL.
Discussion
Very little was found in the literature on AL's treatment after the pull-through procedure of HD patients. Our findings suggested that if timely resuturing was performed, with the help of presacral drainage, symptomatic ALs within five postoperative days could be treated without enterostomy.
The average symptom onset time was 4.3 days in the current study, which was slightly shorter than that reported in the previous studies (5.7 and 7 days).10,17 The shorter symptom onset time could be attributed to the different criteria. We defined the symptom onset time as the time that fever, abdominal pain, or sacrococcygeal pain started, which happened before peritonitis or drainage outflow contains bowel contents. Chronic sinus formation was found in nearly one-third of the AL adult patients who underwent conservative treatment.19,20 In our series, no patients after resuturing had presacral sinus formation. A possible explanation for the inconsistency may be that resuturing could prevent sinus formation.
With the development of aseptic technique, postoperative management, and antibiotic routine application, some early-stage ALs were not caused by severe infections. Patients who received simply resuturing were found to have no or mild pelvic inflammation under laparoscopic observation. Besides, laparoscopic-assisted surgery caused little damage to tissues around the rectum than open surgery, which also meant that the infection caused by the possibly existing bowel contents would be milder. Early detection and shorter delays to management were also key to successful resuturing.
In this study, the average delay to management days in patients who underwent simply resuturing was significantly shorter (0.5 days) than in patients with an ileostomy (2.5 days). However, the diagnostic sensitivity of AL by abdominal ultrasound was only 40%. Thus, abdominal ultrasound was not suitable for the early diagnosis of AL. Besides, plain abdominal radiography was limited by the required patient's transfer, which might make the patient's situation worse. To reach a shorter delay to reoperation, immediate anastomosis examinations with colorectal retractor under general anesthesia for symptomatic AL patients were suggested, which was consistent with the suggestion in a previous study. 17 The extended observation time could lead to severe inflammation around the anastomosis and pelvic infection, making it hard to avoid the ileostomy.
The group simply resuturing had a significantly shorter length of ICU stay, duration of antibiotic use, and LOS, which suggested that the simply resuturing group had more stable vital signs, better short-term postoperative outcomes, and lower hospital costs. Simply resuturing was successfully performed in six early AL patients after the laparoscopic-assisted Soave pull-through procedure of HD without recurrence. Therefore, we believe that for leaks without severe inflammation, enterostomy could be avoided. It can thus be suggested that for patients with early symptoms of AL, timely detection and simply resuturing are safe and could be an optional treatment plan for early AL (<5 postoperative days).
The limitation of this study is that it is a retrospective, single-center, and nonrandomized study. The sample size is relatively small, due to the low incidence rate of AL. General anesthesia is needed when performing anastomosis examinations. The resuturing was performed for up to five postoperative days; whether simply resuturing could treat symptomatic AL over five postoperative days still needs further research.
Conclusion
For early detected and timely diagnosed AL, simply resuturing within 5 days after the laparoscopic Soave procedure of HD could be a safe, effective, and pleasing treatment.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Public Welfare Research, and special funds were received from the National Health and Family Planning of China (Grant No. 201402007).