
Abstract
Background/Objective:
Thoracoscopic repair of esophageal atresia (EA) is gaining popularity, but it is a highly technically demanding procedure. The aim of our study is to evaluate our outcomes in the management of type C EA comparing the thoracoscopic and the open (thoracotomy) approaches.
Methods:
This is a retrospective bicentric study of two major pediatric surgery centers, reviewing all the patients operated for EA with distal tracheoesophageal fistula. Only patients who underwent primary anastomosis were included. From 2008 to 2018, 187 patients were included.
Results:
Forty-seven patients were operated thoracoscopically (TS group) and 140 by the open approach (TT group). Mean gestational age was 38 ± 2.4 weeks in TS group and 36.4 ± 3.3 weeks in TT group (P = .005) with a mean birth weight of 2785 ± 654 g and 2404.9 ± 651 g in TS and TT groups, respectively (P = .003). The mean operative time was 127.6 ± 35 minutes in TS group and 105.7 ± 23 minutes in TT group (P = .0005). The mean postoperative ventilation time and the mean length of stay were significantly shorter in the thoracoscopic group (P = .004 and P < .0001, respectively).
The incidence of anastomotic leak was 8.9% in TS group versus 16.4% in TT group (P = .33). Anastomotic stenosis occurred in 33.3% of TS group and in 22.4% of TT group (P = .17).
Conclusions:
Surgical outcome of thoracoscopic repair of EA is comparable to the open repair with no higher complication rate with the expected skeletal and cosmetic benefits. However, possible bias regarding prematurity, weight at surgery, and associated anomalies must be taken into consideration.
Introduction
Esophageal atresia with tracheoesophageal fistula (EA/TEF) is a rare congenital anomaly, estimated to affect 1/2500–4000 live births. 1 The outcome and survival have improved over the past few decades with the improvement in surgical skills and the advances in neonatal care. 2 Although thoracotomy was considered to be the gold standard approach for EA/TEF repair for years, it was found to be associated with potential musculoskeletal dysfunctions that may interfere later with one's daily activities. 3 The first successful thoracoscopic repair for isolated EA was done in 1999 in a 2-month-old girl. 4 One year later, the first successful neonatal thoracoscopic repair of EA with distal TEF was published. 5 Since that date, thoracoscopic repair of EA started to gain popularity among pediatric surgeons.
A literature review comparing both approaches for EA repair showed that chest asymmetry in the horizontal plane was significantly less pronounced after thoracoscopic surgery. In addition, the incidence of grade I scoliosis was about 10%, which was significantly lower than that after thoracotomy that reached 54%. 6 For this reason, thoracoscopic repair for EA/TEF was adopted by increasing number of surgeons during the last two decades despite being a very technically demanding procedure. 7 Moreover, thoracoscopy was thought to be more advantageous in terms of better visualization of the anatomy which, for example, may help more for proper TEF detection and ligation at the optimal site. 8
In contrast, the CO2 insufflation and the duration of the surgery that may lead to hypercapnia and acidosis were showed to be limitations of this approach, especially for the newborns because of their lung immaturity. Thus, despite the expected benefits, the safety and feasibility of this thoracoscopic approach in neonates remained controversial. 9 Therefore, this study aimed to compare the early outcome of this approach compared to the conventional open surgery.
Materials and Methods
The study was approved by the Institutional Review Board of Necker Enfants Malades Hospital (20200622172921).
This is a retrospective bicentric review of all patients admitted for repair of EA in two major centers for pediatric surgery in Paris between 2008 and 2018. To have a homogenous population, only patients with distal TEF who underwent successful primary anastomosis were included.
In that period, 187 patients were included. One hundred and forty patients were operated by open approach during the whole period from 2008 to 2018 (TT group), and 47 were operated by thoracoscopic approach starting from 2013 to 2018 (TS group). All patients received entire physical examination. Chest X-ray, abdominal ultrasound, and echocardiography were done. Comparison between both groups was made regarding the patients' demographic data, operative data, postoperative course, and length of hospital stay. All patients were followed up till at least the age of 1 year.
Collected data included patient's gestational age (GA), birth weight, age at surgery, and associated congenital anomalies. Operative data were collected, including operative time, conversion from thoracoscopic to open surgery, blood loss, or other intraoperative events. End-tidal CO2 (EtCO2) was recorded at the start and at the end of the procedure. The maximum EtCO2 also was recorded. Collected postoperative data included duration of ventilation, occurrence of anastomotic leaks, anastomotic strictures, recurrent TEF, and need for fundoplication. Anastomotic stricture was defined as the need for at least one endoscopic dilatation session.
Surgery
Preoperative laryngo-tracheoscopy was done in the operative theatre for all patients to confirm the site of distal fistula and to exclude coexistence of a proximal fistula. The surgical approach was chosen according to the surgeon in charge.
Thoracoscopic approach
Patient was placed in left lateral position (70°) or semiprone position. First trocar 5 mm was inserted for the optic below the tip of the scapula. Other two 3 mm trocars were inserted for the working instruments. Rarely, a fourth trocar was needed for lung retraction. Insufflation was started at 5 mmHg and was lowered later on during the procedure if needed. Azygos vein was ligated and divided or controlled with bipolar diathermy in all cases. Closure of the fistula was done using absorbable sutures. Esophageal anastomosis was done in single layer of interrupted sutures after passage of nasogastric tube. Chest drain was inserted in all cases (Fig. 1).
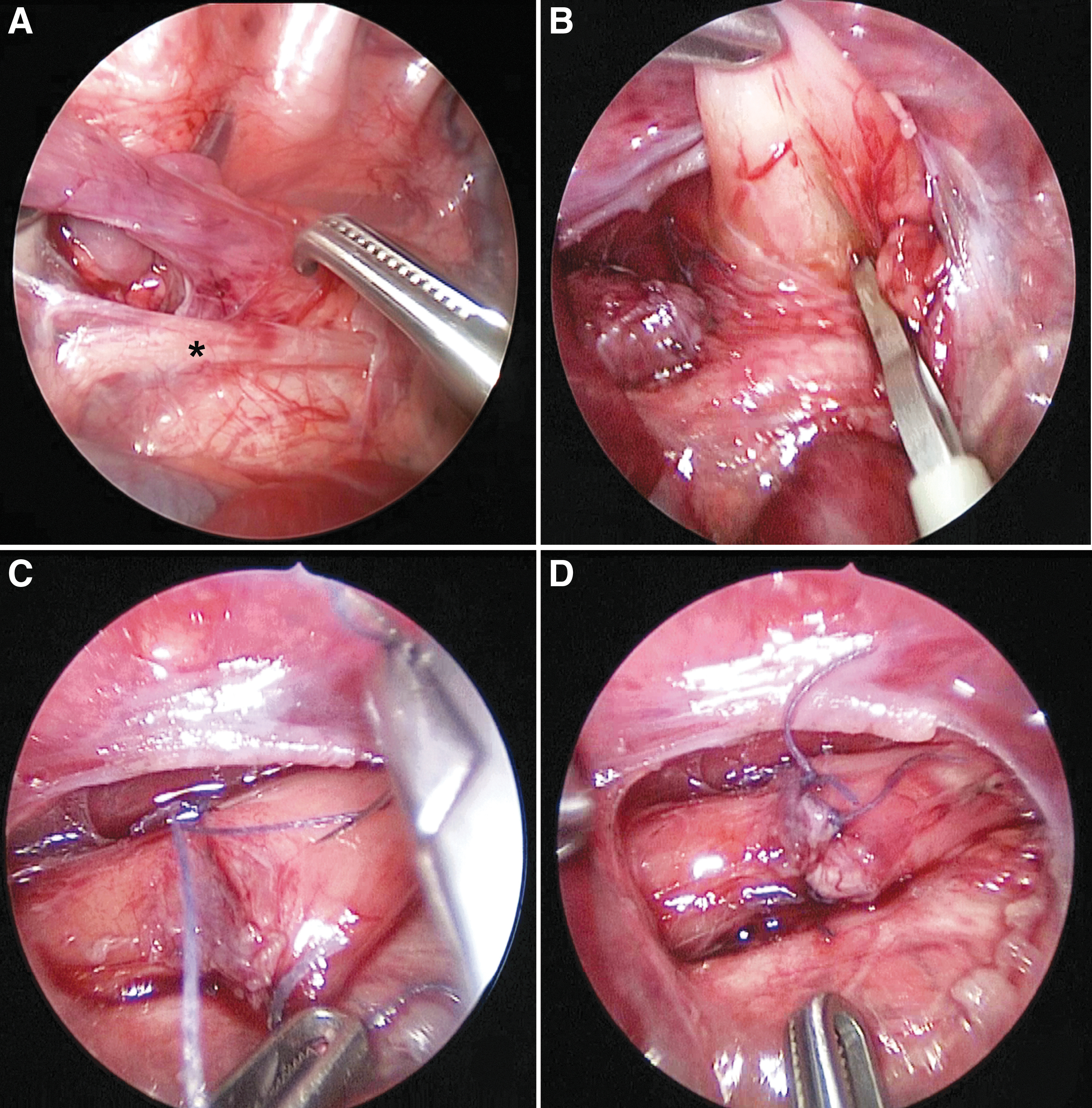
Steps of thoracoscopic approach for EA/TEF repair. Thanks to the camera magnification the anatomic elements are well-visualized.
Thoracotomy approach
Patient was placed in left lateral position. Right posterolateral thoracotomy was done through 4th or 5th intercostal space either extra-pleural or trans-pleural, depending on the surgeon appreciation. Azygos vein division was done in all cases. Section of the fistula and esophageal anastomosis were done using absorbable or nonabsorbable sutures according to surgeon's preference. Chest drain was inserted in all cases.
Postoperative course
All patients were transferred from the operative theatre to neonatal intensive care unit while remaining intubated. Pressure controlled ventilation was used without muscle relaxant. Midazolam was used for sedation, and Sufentanil was used for analgesia during the period of mechanical ventilation in both groups. Enteral feeding was started through the nasogastric tube on the 2nd or 3rd postoperative days if there is no contradiction. Proton pump inhibitors were used in all patients. Oral feeding could be started upon removal of the nasogastric tube after making sure that there is no anastomotic leakage. Considering this point, the two centers have different protocols. Esophagogram was routinely done in one center to rule out anastomotic leakage before oral feeding, whereas in the second center, oral feeding was started if there were no detected respiratory problems on clinical evaluation and chest X-ray.
Statistical analysis
Results were expressed as mean and standard deviation or median and range, according to the data variations. Continuous variables were compared using Mann–Whitney–Wilcoxon test. Discrete variables were compared using Fisher's exact test. P value <.05 was considered significant.
Results
Among the 187 patients, 47 were operated thoracoscopically (TS group) and 140 were operated by the thoracotomy (TT group).
There were 2 deaths in neonatal period in TS group (4.26%). Both were due to multiple congenital malformations, including complex cardiac diseases. Six patients died in TT group (4.29%). All of them suffered from severe forms of cardiac problems: pulmonary atresia, aortic atresia, transposition of great vessels, tetralogy of Fallot, and double outlet right ventricle. There was no significant difference in death rate between the two groups (P = 1). Consequently, statistical analysis of data included 45 patients in TS group and 134 in TT group.
Median age at surgery was 1 day in both groups with range (0–29 days) in TS group and (0–7 days) in TT group (P = .99). There were four conversions from thoracoscopic to open approach (8.9%). The causes for conversion were ventilatory problems that necessitated frequent right lung reinflation in two cases, intolerable hypercarbia with CO2 insufflation in one case, and long gap between the upper and the lower esophageal pouches (more than three vertebral bodies) that entailed open anastomosis in one case.
There was a significant difference between both groups in terms of GA, birth weight, and prematurity. The mean GA was 38 ± 2.42 versus 36.4 ± 3.34 (P = .005), and mean birth weight was 2785.2 ± 654.4 versus 2404.9 ± 650.6 (P = .003) in TS group and TT group, respectively. About 22% of patients in TS group were premature (less than 37-week gestation) versus 45.5% in TT group (P = .008).
There were associated congenital anomalies in 47% (21 cases) in TS group versus 48% (64 cases) in TT group (P = 1), while cardiac anomalies were found in 24% (11 cases) versus 28% (37 cases) in TS and TT groups, respectively (P = .85).
There were no intraoperative complications in both groups. The operative time was significantly longer in TS group with mean 127.6 ± 35.4 minutes compared to 105.7 ± 22.9 minutes in TT group (P = .0005). In addition, the recorded end-tidal CO2 (EtCO2) values during operation were significantly higher in the TS group although there was no statistically significant difference at the start of operation. The mean maximum EtCO2 recorded was 49.3 ± 6.4 for TS group versus 36 ± 2.5 for TT group (P < .0001). Although the CO2 values declined at the end of the operation in both groups, they were still significantly higher in TS group with a mean EtCO2 of 39.7 ± 6.31 versus 32 ± 2.8 in TS and TT groups, respectively (P < .0001) (Table 1).
Comparison of Operative Time and Intraoperative CO2 Values
Statistically significant.
TS, thoracoscopic repair; TT, thoracotomy repair.
Patients in TS group had significantly shorter time to extubation compared to TT group with median of 4 days (2–40) versus 5 days (1–94), respectively (P = .004). After excluding babies with cardiac malformations, median duration was still different with 3.5 days (2–7) in TS group versus 4 days (1–49) in TT group (P = .046). However, with adjustment of the analysis to include only full-term babies, median intubation duration became comparable with 4 days (2–6) in TS group versus 4 days (1–94) in TT group (P = .45).
Hospital stay was significantly shorter in TS group. Median hospitalization period was 25 days (9–98) for TS group versus 42 days (8–130) for TT group (P < .0001). After excluding babies with cardiac malformation, median duration was again still different with 23.5 days (9–98) in TS group versus 32 days (8–115) in TT group (P = .009). With inclusion of full-term babies only, median duration was no more significantly different with 25 days (9–98) in TS group versus 27 days (8–115) in TT group (P = .05) (Table 2).
Postoperative Course Comparison
Statistically significant.
TS, thoracoscopic repair; TT, thoracotomy repair.
The incidence of postoperative complications carried no significant difference between the two groups. Anastomotic leakage occurred in 4 cases (9%) in TS group compared to 22 cases (16%) in TT group (P = .33). All leaks healed spontaneously in TS group, but three cases in TT group (2.2%) needed secondary thoracotomy for toilet and drainage after leakage. These surgeries were performed on the 10th postoperative day in one case and on the 14th day in the other two cases.
Anastomotic strictures that required at least one endoscopic dilatation occurred in 15 cases (33%) of TS group compared to 30 cases (22%) in TT group (P = .17). The median number of needed dilatation sessions was 2 in both groups (range 1–5) (Fig. 2).

Postoperative contrast study after open EA repair. The contrast study shows an anastomotic stenosis at the proximal third of the esophagus with a subsequent proximal dilatation.
Six cases (13%) in TS group suffered from significant reflux that required fundoplication where this happened in 10 cases (7.5%) in TT group (P = .24). Gastrostomy button placement was done at time of fundoplication in 2 cases of 6 (33%) in TS group and in 5 cases of 10 (50%) in TT group. The median age at fundoplication was 3.5 (1.7–14) months in TS group compared to 4 (1.5–78) in TT group (P = .59).
There was recurrent TEF in 3 cases (2.2%) in TT group that were managed with second thoracotomy. All of them were premature babies, while two of them (66%) suffered from cardiac problems. However, this complication was not observed in TS group (P = .57) (Fig. 3).
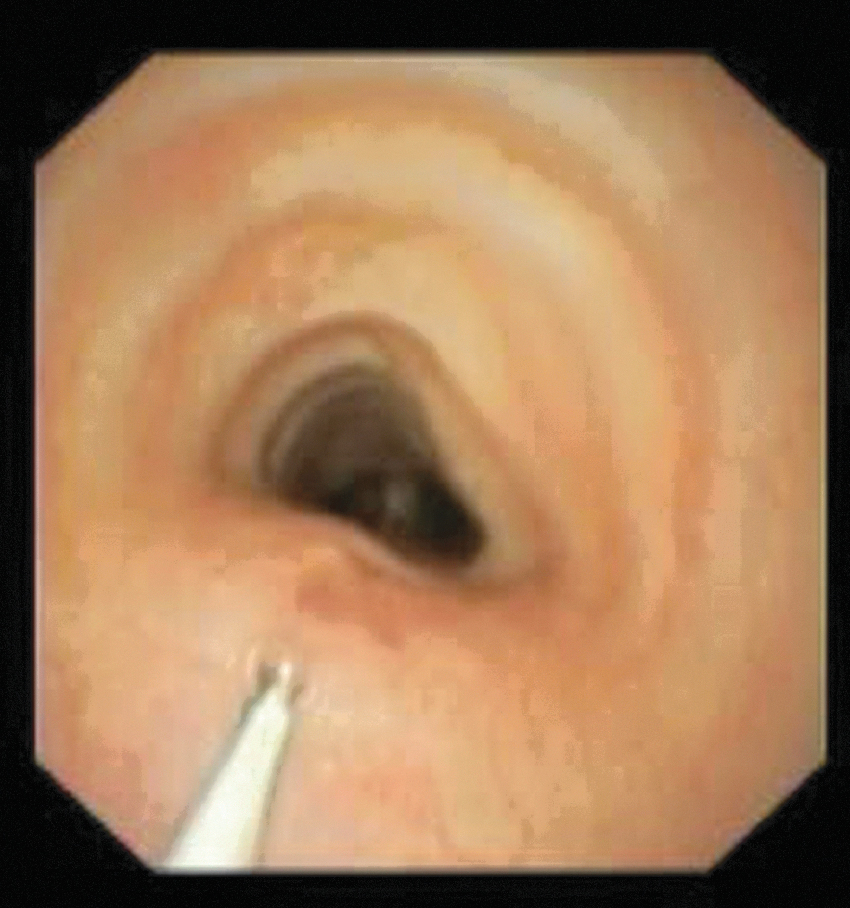
Endoscopic view of the trachea for recurrent fistula. The anterior wall of the trachea is identified by the cartilage rings. The posterior wall is partially collapsed because of mild tracheomalacia. The tracheoesophageal fistula is confirmed by the introduction of a catheter. The distal part of the catheter has to be visualized in the esophagus.
Aortopexy was done in 5 cases (3.7%) of TT group due to severe tracheomalacia associated with life-threatening events, while this was not required in TS group (P = .33). Two of the 5 cases were cardiac and premature babies, while 1 of them was neither cardiac nor premature. In addition, there was 1 cardiac baby and 1 premature baby. Median age at aortopexy was 14 months ranging from 4.5 to 72 months.
Discussion
The main aim of the thoracoscopic approach was to avoid the skeletal deformities that may follow thoracotomy for EA/TEF repair. In one review of 322 EA/TEF patients, about 60% of them had skeletal sequelae after repair by thoracotomy. 10 Another study compared chest deformities following thoracoscopy versus thoracotomy for EA/TEF. They found significantly higher incidence of chest asymmetry, narrow intercostal spaces, and scoliosis after thoracotomy compared to thoracoscopy. 6 Moreover, thoracoscopy for EA repair has the great advantage of excellent visualization of posterior mediastinal structures. 11 In addition, it provides better visualization of esophageal pouches and mucosal layer during anastomosis. 12 But on the other hand, thoracoscopic repair of EA is considered a technically demanding procedure particularly for the anastomosis in a relatively narrow working space. Consequently, with gaining more experience, there was improvement in terms of operative time and incidence of anastomotic leaks and strictures. 13 This concept was proved by a study comparing the first and second 5-year experience in thoracoscopic EA repair. 14
With the emergence of this technique, thoracoscopic approach was not recommended in some circumstances. For example, in 2005, Rothenberg considered that significant prematurity (< 1500 g) was an absolute contraindication. 15 In another study comparing thoracotomy with thoracoscopy, neonates with body weight >2000 g only were considered as good candidates for thoracoscopic approach. 11 However, in another study, outcome in patients <2000 g was shown not to be statistically different from those weighing >2000 g. 16 Although, in our study, there was a significant difference between body weight in the two groups, we did not use selection criteria to determine the surgical approach. Moreover, we had one patient in TS group who weighed only 1420 g with uneventful perioperative and postoperative courses. To go further, a randomized control study is now needed.
The time needed till extubation after thoracoscopy was found to be significantly shorter in previous comparative studies.7,11 This may be explained by the uniform collapse of the lung by pneumothorax during thoracoscopy compared to mechanical lung manipulation and retraction during thoracotomy and also by the less postoperative pain. 7 However, another study found no significant difference in the postoperative ventilation duration. 17 In our study, the time needed till extubation was significantly shorter in TS group than TT group in the whole population, but we did not find a significant difference in the duration of ventilation and hospital stay after excluding preterm neonates from the statistical analysis of this point.
Apart from the technical hurdle, the two other main drawbacks of thoracoscopic approach are the longer operative time and the effect of CO2 insufflation. In our study, as well as other comparative studies, the operative time was significantly longer in TS group. 17 One meta-analysis that included 6 comparative studies also concluded that operative time was longer in TS group. 18 However, other studies concluded that there was no significant difference.7,11 With the use of thoracoscopy in pediatric surgical procedures, the tolerability of neonates to CO2 insufflation was questioned. It was found that CO2 absorption from induced pneumothorax in thoracoscopy is more than that from induced pneumoperitoneum in laparoscopy. 19 Szavay et al. reported significantly higher intraoperative CO2 levels in thoracoscopy compared to thoracotomy. 17 This comes in line with our findings. However, Yamoto et al. and Bishay et al. found no significant difference in intraoperative CO2 levels between thoracoscopy and thoracotomy.11,19 We would however mention that the longer operative time and higher intraoperative CO2 values in our study did not have burden on the postoperative ventilation time and length of hospital stay in TS group compared to TT group.
Regarding the common complications after EA repair, including the rate of anastomotic leakage and stricture, two meta-analyses concluded that there was no significant difference between thoracoscopy and thoracotomy, the finding that comes in agreement with our results.18,20 So, thoracoscopy is comparable to thoracotomy in this point and does not carry higher risk for postoperative complications.
For exclusion of anastomotic leakage, one of the two included centers adopted doing contrast esophagography as a routine in every patient before starting oral feeds. This meets with the recommendations of Lovvorn Iii et al. 12 However, one study investigated the value of early postoperative esophagography and concluded that it is not systematically necessary, showing that major leaks are usually apparent clinically and that the radiological detection of minor asymptomatic leaks does not affect the management. 21 In the same vein, Patkowski et al. found that anastomotic leak was almost always detected before having esophagography in 5th or 6th postoperative day, making the esophagography not essential unless to have an idea about the size of anastomosis. 22 In our second center, contrast esophagography was done only when leak was suspected. It depended on the clinical assessment of chest condition and chest radiograph to suspect a leak. With this protocol, all leaks were successfully suspected before starting oral feeds (15 cases), and esophagography was avoided in 82 (84.5%) of the patients.
The first limitation of this study is that it was a retrospective one. In addition, the study population was not completely homogenous knowing that there was a significant difference between the two groups regarding birth weight and GA. Furthermore, the approach in our study was mainly selected according to the surgeon's personal preference with no obvious objective criteria. For these reasons, a prospective randomized study is considered necessary for better judgment on feasibility and safety of thoracoscopic approach compared to the conventional open one.
Surgical outcome of thoracoscopic repair of EA/TEF is comparable to the open repair with no higher complication rate and with the expected benefits of avoiding skeletal deformities and better cosmesis. The additional probable advantages of thoracoscopy are shorter time of postoperative ventilation and shorter hospital stay. However, randomized control trial on large number of cases is needed to support these results, controlling the possible bias regarding prematurity, weight at surgery, and associated anomalies.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.