
Abstract
Background:
Minimally invasive abdominal wall reconstruction, utilizing transversus abdominis release (TAR), has been described and shown to be beneficial for ventral hernia repair (VHR). Limited literature is available surrounding the hybrid robotic TAR (h-rTAR) approach, which combines robotic dissection and component separation with open fascial defect closure and mesh deployment. In this study, we describe our h-rTAR technique and present our center's postoperative and patient-reported outcomes (PROs).
Methods:
h-rTAR VHRs performed between 2013 and 2018 were examined. The h-rTAR technique was described. Patient characteristics and operative variables were analyzed. Perioperative results were presented according to European Hernia Society (EHS) classifications. Pre- and post-operative hernia-specific quality-of-life (QoL) assessments were conducted.
Results:
Twenty patients who underwent an h-rTAR were included in this study. All hernias were incisional. A bilateral TAR needed in 90% of patients. The average hospital stay was 1.8 days. Two patients experienced medical complications and 5 patients experienced surgical site events. None of the patients experienced a hernia recurrence throughout a mean postoperative follow-up period of 319 days. PROs showed improvement in all domains, especially cosmetic.
Conclusion:
The h-rTAR technique combines the benefits of robotic and open techniques when used for large incisional VHR with improvement in patient-reported QoL.
Introduction
Minimally invasive ventral hernia repair (VHR) allows for retromuscular (RM) repair, which is traditionally accomplished with a large incision. 1 For incisional hernias, reconstructing the abdominal wall by performing an open component separation with transversus abdominis release (TAR) offers wide mesh coverage with minimal recurrence.2,3 The same repair has been performed using the robotic platform, providing similar dissection capabilities with the added benefit of minimally invasive surgery. A recent study showed that robotic TAR (rTAR) was associated with a shorter hospital length of stay (LOS) than open TAR. 4 The hybrid technique combines robotic dissection and component separation with open fascial defect closure and mesh deployment. This study aimed to describe hybrid robotic TAR (h-rTAR) and report the early outcomes of this technique, including patient-reported outcomes (PROs).
Materials and Methods
A prospectively collected database of h-rTAR VHRs, performed between February 2013 and April 2020, was analyzed retrospectively. Patients who underwent nonhybrid VHR (fully robotic), such as robotic intraperitoneal onlay mesh (IPOM), transabdominal (TA) preperitoneal, robotic retromuscular (rRM), and rTAR were excluded from the study. Informed consent was obtained from all study participants.
The database included patient and hernia characteristics, patient comorbidities, operative variables, and postoperative results. Hernia-specific variables such as localization, size, and classification were presented in accordance with the recommendations of the European Hernia Society (EHS). 5
Postoperative complications were recorded as detailed in patient follow-up visits and by applying the Ventral Hernia Recurrence Inventory algorithm. 6 The Clavien–Dindo classification system was used to categorize all complications. 7 The Comprehensive Complication Index (CCI®) scale was used to determine morbidity scores. 8 Wound complications were further categorized as surgical site events (SSEs), including surgical site infections (SSIs) and surgical site occurrences (SSOs). Any SSO or SSI that necessitated interference, such as wound reopening, drain placement, or reoperation qualified as an SSO/I-PI. The severity of postoperative seromas was described according to the Morales-Conde classification. 9
Pre- and postoperative hernia-specific quality-of-life (QoL) assessments were performed using the European Hernia Society Quality of Life (EuraHS-QoL) questionnaire, which evaluates pain, activity hindrance, and cosmesis-related outcomes using a numerical-based system. 10 Questionnaires were filled both pre- and postoperatively at 3 weeks, 3 months, and yearly follow-up visits if applicable.
Surgical technique
Preoperative consideration
For large incisional ventral hernias there is a high degree of complexity and judicious physical examination and preoperative imaging is necessary. Ideally, risks factors that affect wound healing such as obesity, malnutrition, and diabetes mellitus should be optimized, and smoking cessation should be encouraged before elective procedures. Obtaining recent abdominopelvic imaging with computed tomography allows for cross-sectional and longitudinal images that are valuable to delineate the hernia.
Patient preparation
The patient is placed in the supine position (Fig. 1). Flexing the bed slightly allows for maximal space between the costal margin and iliac crest so as to lessen robotic arm interference.

rRM VHRs were conducted through either a TA or totally extraperitoneal (TEP) access.
Port access and positioning
TA access
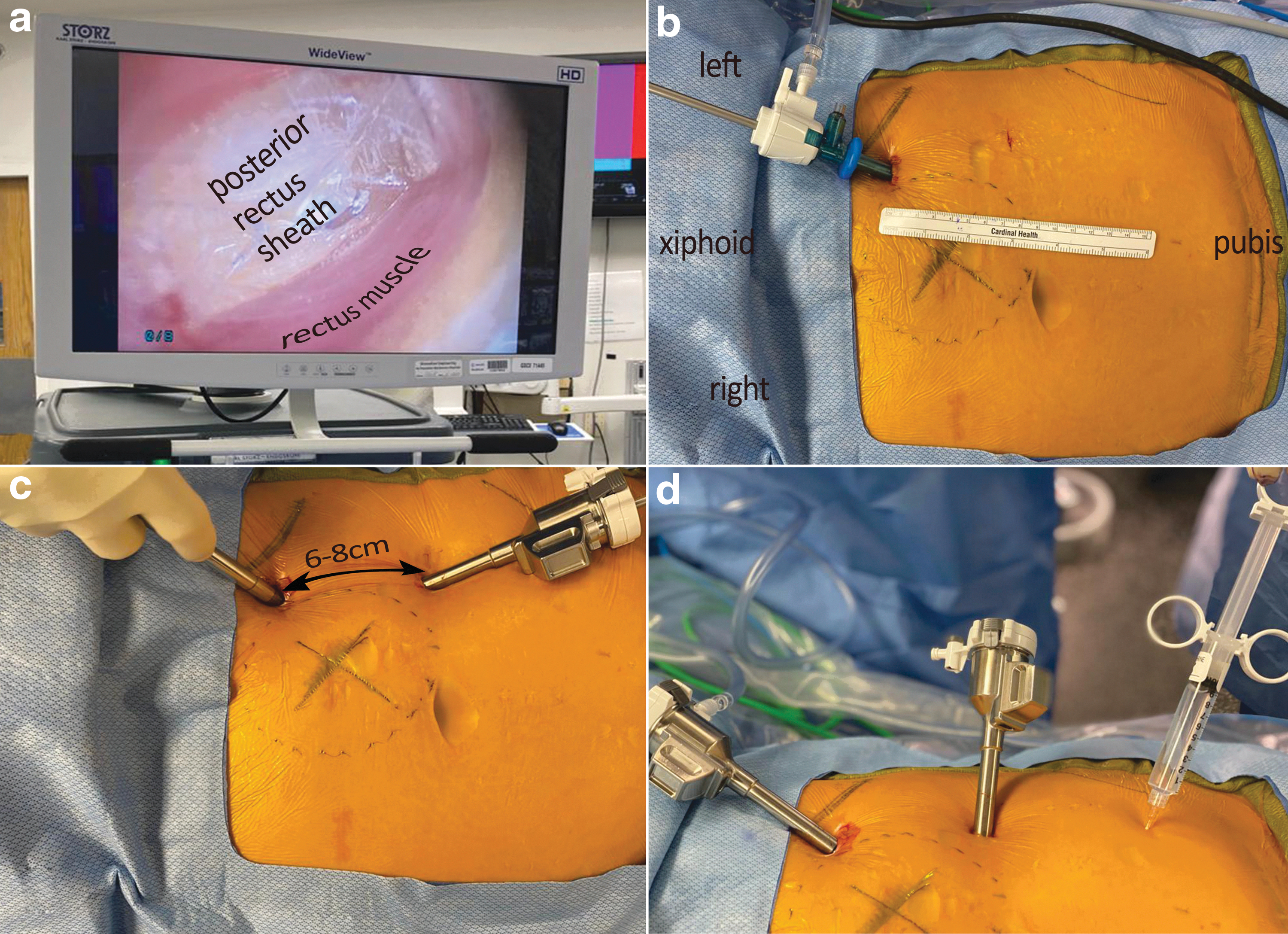
Initial access is obtained by inserting a Veress needle in the left upper quadrant (LUQ) (Fig. 2). An 8 mm port is inserted as lateral as possible within the rectus sheath in the LUQ. Two additional 8-mm ports are next inserted bluntly to prevent inadvertent bleeding, with an 8-cm spacing between ports. Adhesions are lysed as required. The posterior rectus fascia is then cut. The contralateral retrorectus dissection is first performed. Once this is completed, a TAR is performed as described earlier. The robot is undocked and three trocars are inserted similarly on the contralateral side.
TEP access
The first trocar is inserted through optical trocar entry in the LUQ, as lateral as possible within the rectus sheath. A 5-mm laparoscopic 0° camera is inserted into a 5-mm optical trocar. Under direct visualization, the trocar is advanced through the subcutaneous tissue and the anterior rectus sheath. Immediately after visualizing the rectus muscle fibers, the trocar is directed inferiorly to avoid penetration of the posterior layer. After using laparoscopic blunt dissection aided by high-pressure insufflation to dissect a sufficient area, the two remaining 8-mm trocars are inserted. With an 8-cm spacing between trocars, a lateromedial and angled advancement is used to insert trocars and minimize robotic arm mechanical interference. The initial 5-mm trocar is then substituted by an 8-mm trocar.
Docking and instruments
Once the trocars are placed, the patient-side cart of the da Vinci surgical system (model Xi) is docked (Fig. 3). The following instruments are used: a bipolar grasper and monopolar scissors, which are later substituted by a needle driver. The 30° scope is directed toward the surgical field of interest and the system uses a predetermined algorithm to optimize arm positioning.

RM dissection and crossover
Ipsilateral retrorectus dissection is performed and any previous transfascial sutures are cut if encountered (Fig. 4). Then a crossover technique is performed to reach its contralateral counterpart. 11 In large incisional hernias, the tissue adjacent to the hernia are often fused and hard to differentiate. We recommend beginning crossover in virgin tissue planes away from the hernia, if possible. The medial border of the retrorectus space is incised to reach the contralateral side, followed by craniocaudal dissection toward the incisional hernia site. If a very thin preperitoneal layer is encountered, any tears in the posterior layer will need to be sutured later. After performing the crossover, both retrorectus spaces are now partially merged. Circumferential dissection is performed to facilitate hernia content reduction. The hernia sac is then breached to directly visualize reduction of the contents. To facilitate midline reconstruction and reinforce the visceral sac, a posterior component separation, TAR is performed.

Transversus abdominis release
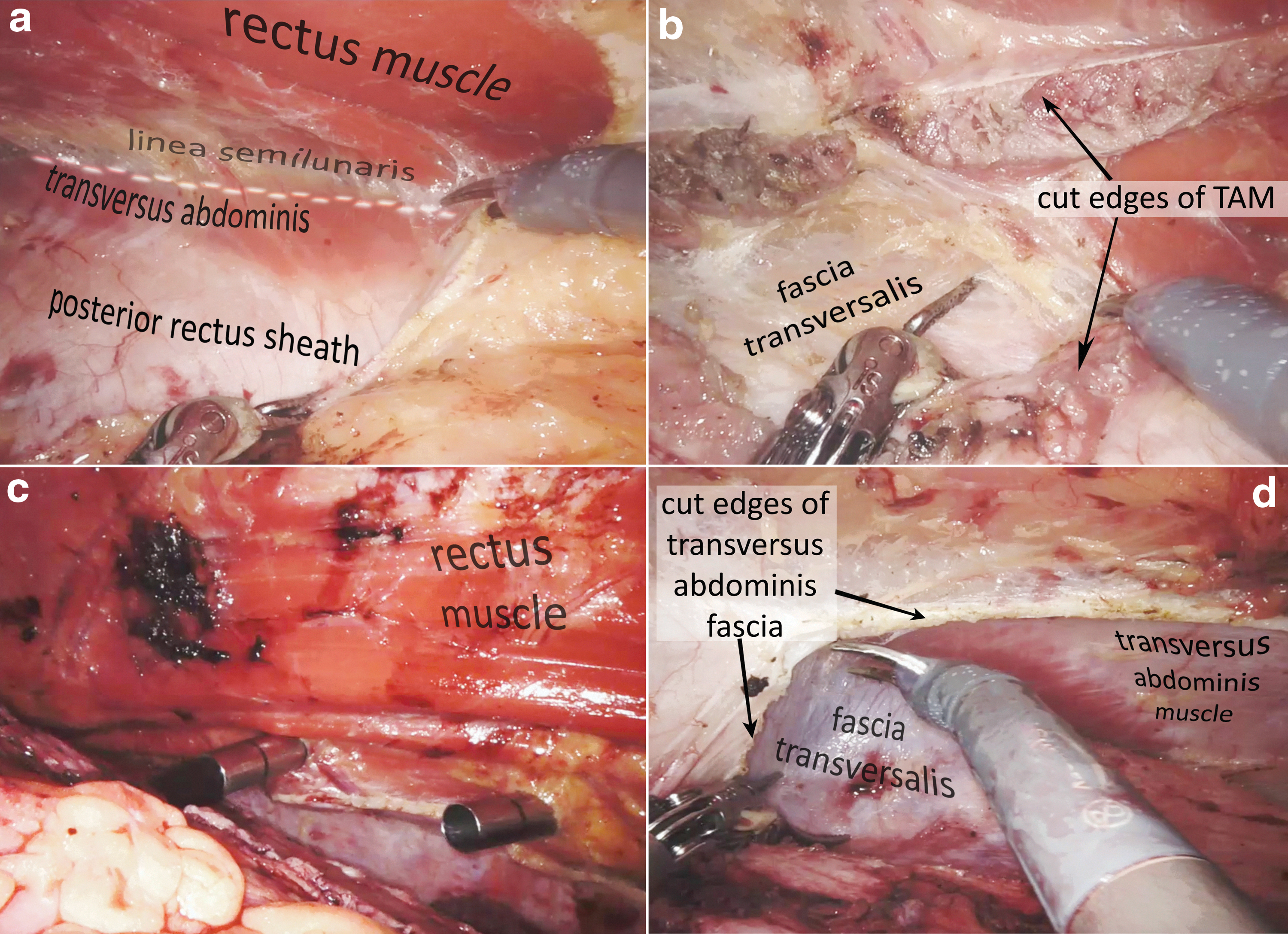
The transversus abdominis fibers are visualized along the contralateral rectus sheath (Fig. 5). Dissection is initiated along the contralateral rectus sheath, parallel and medial to the linea semilunaris (LS). It is crucial to avoid disruption of the LS, which is considered a technical error. Neurovascular structures are marked and preserved within the lateral edge of the retrorectus space. Next, the transversus abdominis muscle is separated from its fascia along the mid-axillary line using traction and conservative monopolar use. Under direct visualization, trocars are inserted in the contralateral right rectus space and TAR is performed similarly on the left side if needed.
Fascial reconstruction
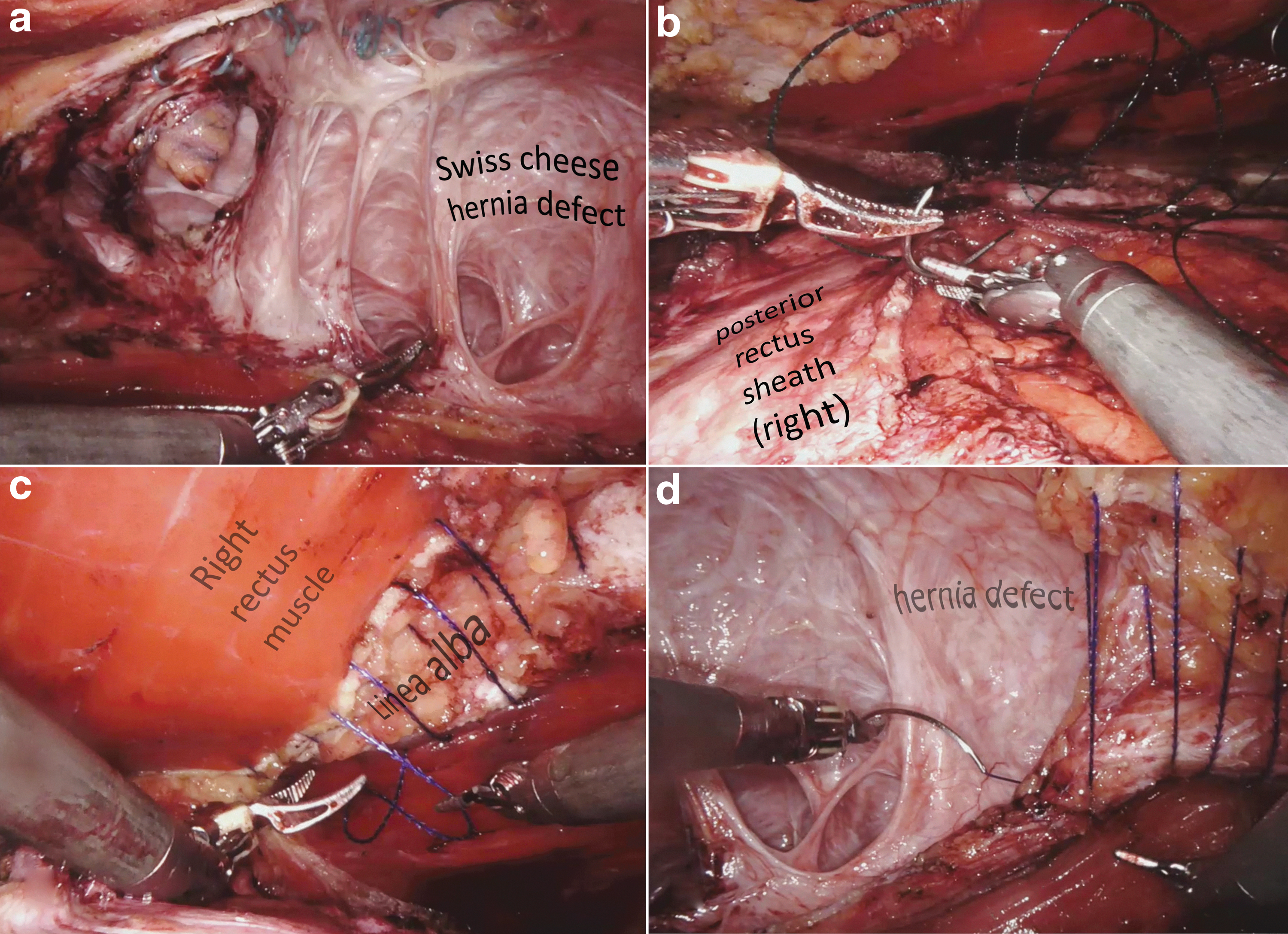
Reapproximation of the posterior rectus sheath edges is achieved with a 2-0 absorbable suture (Fig. 6). The anterior fascial defect closure is then started in a caudal to cranial direction, using absorbable barbed suture, taking 5–8 mm bites of the fascia with 5-mm spacing 12 and leaving a gap to allow for mesh insertion. Loose suturing is used to begin hernia defect closure, which will later be tightened after mesh deployment.
Mesh deployment
The skin is incised above hernia defect (Fig. 7). The mesh is inserted through the gap left during defect closure and is deployed to fully occupy the RM space. The remaining defect gap is closed through the open approach and the surgical field is re-insufflated, under low pressure, to assess the mesh positioning.

Technical considerations
Mesh fixation is usually not required since the mesh fully occupies the RM space and intra-abdominal pressure helps maintain the mesh position. In general, drain placement is not required and fascial defects at the trocar sites are not closed. Skin incisions are sutured after injecting local anesthesia. In cases with redundant skin and soft tissue or hernia sac, these may be excised during the open portion of the hybrid technique. This technique can also address cases with open wounds due to mesh erosions.
Postoperative course
Patients who underwent h-rTAR were expected to be discharged home after a one-night stay. Patients were instructed to continue with their regular activities postoperatively, but were counseled to avoid any strenuous activities for a minimum of 45 days.
Statistical analysis
Categorical variables were reported as a percentage (%), and continuous variables as a mean ± standard deviation (SD), median (interquartile range [IQR]), according to their distributions. Some ranges (min–max) were used to report outliers and to facilitate interpretation. A comparison of dependent non-normally distributed variables was performed using the Wilcoxon signed-rank test, which detects differences between variables from the same sample before and after surgery by calculating the differences between their ranks. Statistical analyses and graphics were rendered by SPSS (Statistical Package for Social Sciences for Windows) and Microsoft Excel 2019 (Microsoft Office for Windows). Any P value of .05 or less was regarded as statistically significant.
Results
Twenty patients who underwent h-rTAR were evaluated in this study. Patients demographics are summarized in Table 1. All hernias were incisional in nature. Fifteen (75%) patients underwent surgery due to a recurrent incisional hernia, and of these, 6 (30%) patients had a history of multiple recurrences (≥2 prior hernia repairs).
Patient Demographics
ASA, American Society of Anesthesiologists; BMI, body mass index; COPD, chronic obstructive pulmonary disease; h-rTAR, hybrid robotic transversus abdominis release; SD, standard deviation.
All repairs were performed in an elective setting, except for one emergent case. TA trocar access was used in 6 (30%) patients, whereas TEP-access was used in 14 (70%) patients. All patients required adjunctive TAR. A bilateral TAR was required in 18 (90%) patients and a unilateral TAR was required in 2 (10%) patients. In 1 patient, a bilateral inguinal hernia repair was performed concomitantly with the index procedure.
Hernia and intraoperative variables are presented in Table 2. The most frequent hernia locations were M3 and M4 according to EHS classification. 5 The median hernia defect width was 15 cm (min–max = 10–23 cm). All hernia repairs were performed using a Synecor Pre™ (W.L. Gore & Associates, Inc., Newark, DE) mesh except for one case involving a Bard® Soft Mesh (Bard-Davol, Inc., Warwick, RI). A serosal small bowel injury occurred in 1 (5%) patient during adhesiolysis and was sutured. In the postoperative recovery unit, the patients' median (IQR) pain score was 5 (4–6.5), assessed verbally on a 0–10 scale. The mean ± SD morphine milligram equivalent was 11.9 ± 6.7. The average LOS was 1.8 days (min–max: 1–11 days), indicating that the majority of patients were discharged on POD-1 (70%).
Hernia Characteristics and Operative Variables
h-rTAR, hybrid robotic transversus abdominis release; IQR, interquartile range; SD, standard deviation.
Thirty-day hospital readmission was observed in 2 (10%) cases due to pneumonia and acute kidney injury. All postoperative complications were low grade (CD grades I and II), except for 1 patient who experienced a grade-IVa complication (acute kidney injury without the requirement of dialysis). Regarding SSEs, a superficial SSI was noted in 2 cases, whereas a seroma occurred in 3 cases. Two seromas were incident (type-2a) and one was a type-4b complication according to the Morales-Conde classification. 9 Complications are presented in Table 3. No recurrences were observed throughout the mean postoperative follow-up of 319 days (min–max: 32–1023).
Postoperative Complications Profile
For patients who experienced more than one complication, the highest-grade complication was presented.
CCI, comprehensive complication index; h-rTAR, hybrid robotic transversus abdominis release; IQR, interquartile range; SSE, surgical site event; SSI, surgical site infection; SSO, surgical site occurrence.
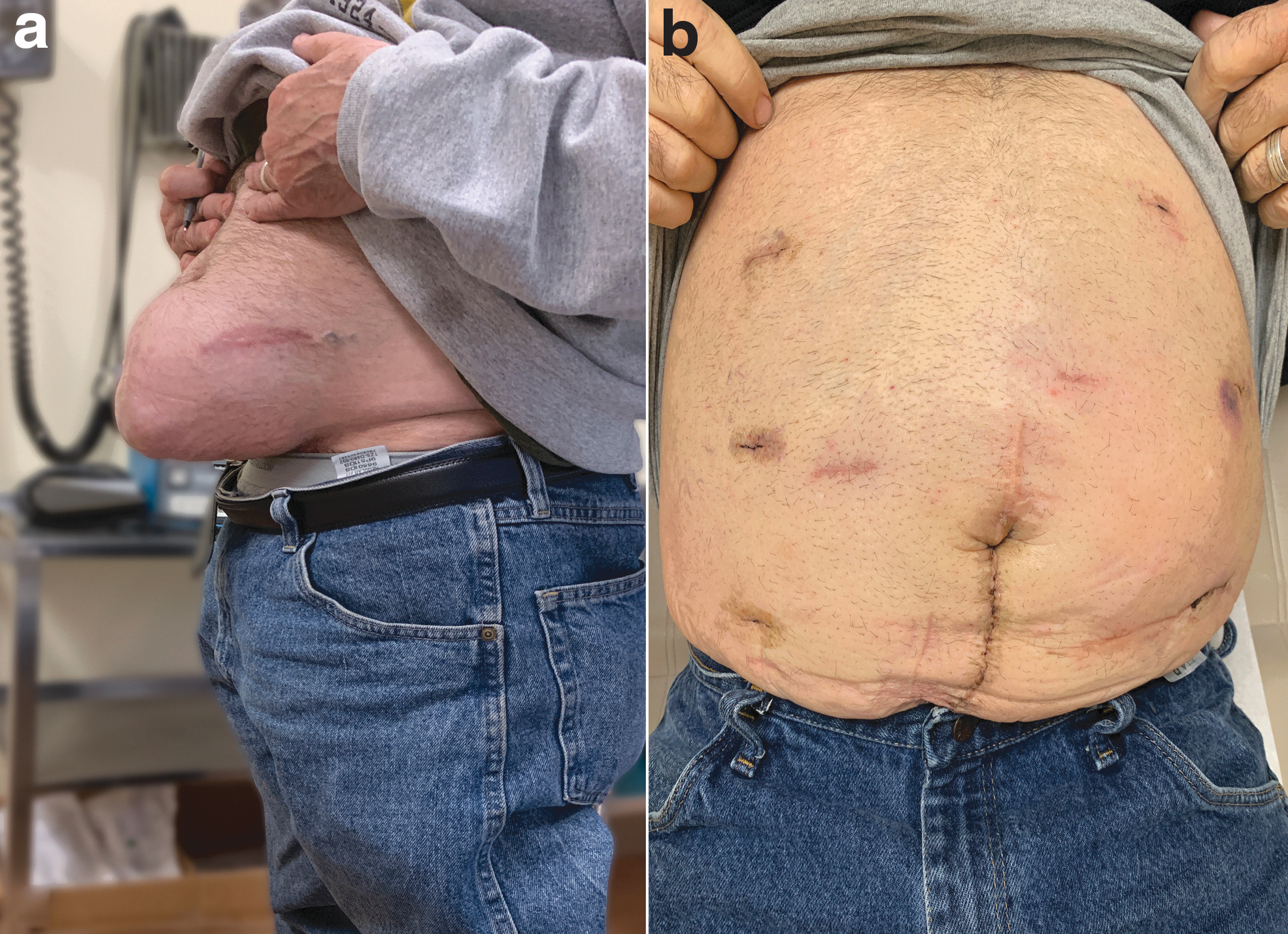
EuraHS-QoL questionnaires were completed by 18/20 patients. When comparing the preoperative to the most recent postoperative PRO questionnaires, all domains showed improvement, especially the cosmetic domain (Fig. 8). The results for each question are shown in Table 4 and Figure 9.
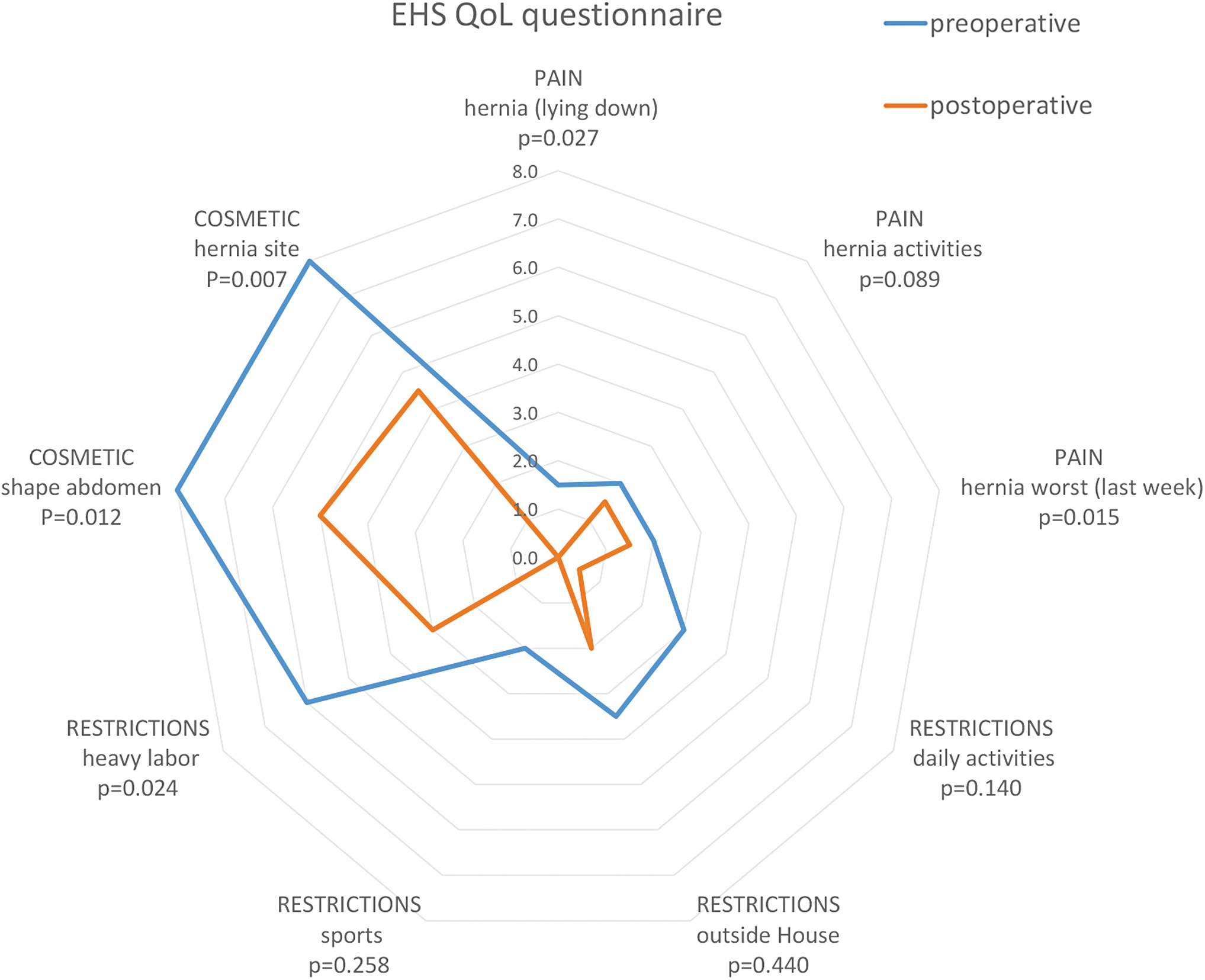
Web graph of the patient-reported outcomes assessed before and after the operation.
Patient-Reported European Hernia Society Quality-of-Life Outcomes
Bold p-values are significant.
IQR, interquartile range.
Discussion
The Rives–Stoppa technique is often inadequate for repairing large defects since it is confined by the lateral borders of the retrorectus space, which may prohibit the use of a large mesh. A posterior component separation technique, which uses TAR, creates adequate space for a mesh sublay due to increased lateral dissection and posterior rectus fascia advancement, which are beneficial in larger abdominal wall defects. 3 TAR has been successfully performed using the robotic platform and multiple studies between open TAR and rTAR revealed that both the LOS and wound morbidity were lower in rTAR VHR.4,13,14 The LOS is likely decreased due to less postoperative pain for rTAR repair.4,13
Hybrid repairs have been described in laparoscopic IPOM and may be accomplished by laparoscopic lysis of adhesions followed by open mesh insertion and primary closure with subsequent laparoscopic mesh fixation. 15 A hybrid robotic procedure, where the hernia sac is opened after robotic component separation to allow for mesh deployment and closure of the anterior fascia, has been previously described and compared with rTAR. Halka et al. 16 studied hybrid TAR versus rTAR, and among 25 patients in the hybrid TAR group, the mean defect width was 14.24 cm (±4.82 cm) and the mean procedure time was 344 minutes. Conversely, the mean defect size in our study was 15.9 cm (±3.70 cm) and the majority of cases were performed using TEP access. Another study by the same authors compared h-rTAR with open TAR. 17 The median LOS after 49 h-rTARs was 3 days, as compared with our study's mean LOS of 1.8 days (median = 1 days).
There are a few study limitations. Despite a fairly small sample size, this single-center study reflects a single surgeon's experience. There is also a selection bias of which patient will undergo h-rTAR. This technique requires extensive familiarity with the relevant anatomical landmarks and complex hernia repair techniques, as well as proficiency with the robotic platform.
In conclusion, the h-rTAR technique combines the advantages of robotic and open techniques, with notable improvements in patient-reported QoL. This technique may be beneficial for the repair of large incisional ventral hernias.
Ethical Approval
The current database has received approval from the IRB.
Human and Animal Rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all study participants.
Footnotes
Disclosure Statement
COI: Dr. Kudsi receives a teaching and consultancy related fees from Intuitive, Bard, Gore, unrelated to this study. Drs. Chang, Bou-Ayash, and Gokcal have no COIs to divulge.
Funding Information
No funding was received for this study.