
Abstract
Purpose:
To compare the relative clinical efficacies of radioactive and normal stent insertion methods as a means of treating patients suffering from malignant esophageal obstruction (MEO).
Materials and Methods:
The Pubmed, Embase, and Cochrane Library databases were searched for relevant randomized controlled trials (RCTs) from the date of inception through to July 2020. RevMan v5.3 was used for all data analyses.
Results:
This meta-analysis included six RCTs that included a total of 194 patients who had undergone radioactive stent insertion and 209 who had normal stent insertion. There were no significant differences in pooled improvement of dysphagia scores (P = .40), rates of stent restenosis (24.7% versus 28.7%, P = .35), stent migration (3.3% versus 4.4%, P = .61), severe chest pain (22.8% versus 20.3%, P = .61), hemorrhage (11.0% versus 9.8%, P = .80), or fistula formation (6.1% versus 4.2%, P = .55) between two groups. The pooled time to restenosis (P < .00001) and survival (P < .00001) were significant longer in the radioactive stent group. Significant heterogeneity was detected in the endpoint of improvement of dysphagia score (I2 = 89%; P = .0002). Funnel plot analyses did not detect any evidence of publication bias pertaining to the selected study endpoints.
Conclusions:
Our meta-analysis demonstrated that radioactive stent insertion can prolong stent patency and survival for patients with MEO compared with normal stent insertion.
Introduction
Malignant esophageal obstruction (MEO) is usually secondary to esophageal and other chest cancers,1–4 and >80% of cases with MEO were found to be caused by esophageal cancer. 2 In one study, when patients were diagnosed with MEO, >80% of the cases missed the chance for curative resection. 5 In addition, patients with MEO had a poor quality of life during their limited survival time because of dysphagia.
Stent insertion is typically employed as a first-line palliative treatment in patients with incurable MEO.1–4 Normal stent insertion, however, does not directly affect the primary tumor. Thus, the prolongation of stent patency and overall survival time typically necessitates further intervention with anticancer treatments.6,7 To combine the treatment effects of radiotherapy and stent insertion on MEO, researchers have developed a form of radioactive stent loaded with 125I seeds.8–10 Although many studies regarding of esophageal radioactive stents have been published, the number of randomized controlled trials (RCTs) are limited.11–16
To come to a definite conclusion on the effectiveness of the esophageal radioactive stent, we conducted a meta-analysis of RCTs to compare the relative clinical efficacies of radioactive and normal stent insertion methods for the treatment of patients suffering from MEO.
Materials and Methods
Study selection
This meta-analysis was approved by our institutional review board. The Pubmed, Embase, and Cochrane Library databases were searched for relevant studies from the date of inception to July 2020 using the following search strategy: (((stent[Title/Abstract]) OR (SEMS[Title/Abstract])) AND ((((irradiation[Title/Abstract]) OR (seed[Title/Abstract])) OR (radioactive[Title/Abstract])) OR (iodine[Title/Abstract]))) AND ((esophageal[Title/Abstract]) OR (esophagus[Title/Abstract])).
The following study inclusion criteria were used:
(a) Type of study: RCTs (b) Disease: MEO (c) Types of intervention: radioactive versus normal stent insertion (d) Language: any.
Studies were excluded if they were any of the following:
(a) Noncomparative studies
(b) Non-RCT studies
(c) Animal or other preclinical studies
(d) Review articles.
Data extraction
Two investigators independently extracted the data from all identified articles, with the corresponding author helped to resolve any inconsistencies in the data. The extracted items included three data types: study baseline data, patient baseline data, and treatment-associated data.
Quality and bias assessment
The eight-point Jadad composite scale was used to gauge the quality of all the included RCTs, 17 and RCTs with scores ≥4 points were considered to be high quality. Potential biases were assessed using the Cochrane risk of bias tool.
Endpoints
The primary endpoints for this meta-analysis were stent restenosis and survival, whereas the secondary endpoints included improvement of dysphagia score, stent migration, severe chest pain, hemorrhage, and fistula formation.
Statistical analyses
The software RevMan v5.3 was used for all data analyses. The Mantel–Haenszel method was used to measure pooled odds ratios (ORs) and 95% confidence intervals (CIs) for dichotomous variables, whereas continuous variables were analyzed based on the mean difference (MD) and 95% CIs. We used the hazard ratio (HR) with a 95% CI to measure the pooled survival times. Study heterogeneity was assessed through χ 2 and I2 tests, with I2 > 50% being indicative of significant heterogeneity. Random-effects models were used in the presence of significant heterogeneity, whereas fixed-effects models were used for analyses when significant heterogeneity was not detected. The causes of heterogeneity were evaluated through sensitivity and subgroup analyses, and funnel plots were used to assess the risk of bias.
Results
Study characteristics
Our initial search strategy identified 154 potentially relevant studies, and 6 RCTs were ultimately included in our meta-analysis (Fig. 1). The Jadad composite scale of the six RCTs ranged from 2 to 5 (Table 1). Three RCTs had a high risk of random sequence generation and allocation concealment,11,14,15 and none of the RCTs were double-blind studies (Fig. 2). Fluoroscopic-guided stent insertion was used in five studies,11,12,14–16 and endoscopic-guided stent insertion was used in one study. 13 The six RCTs involved a total of 194 patients who had undergone radioactive stent insertion and 209 who had undergone normal stent insertion (Table 1). The outcome data are shown in Table 2.
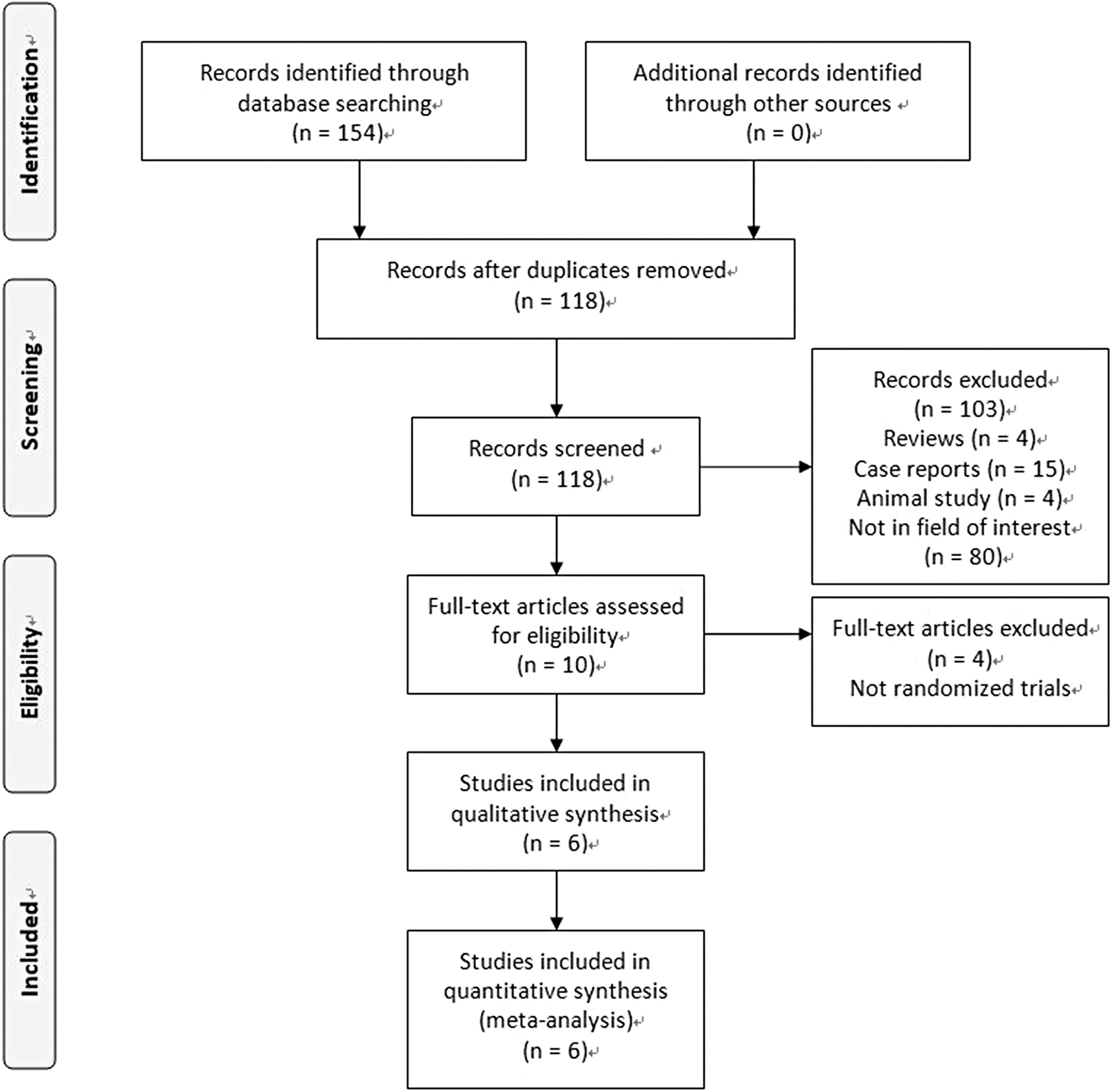
The flowchart of this study.
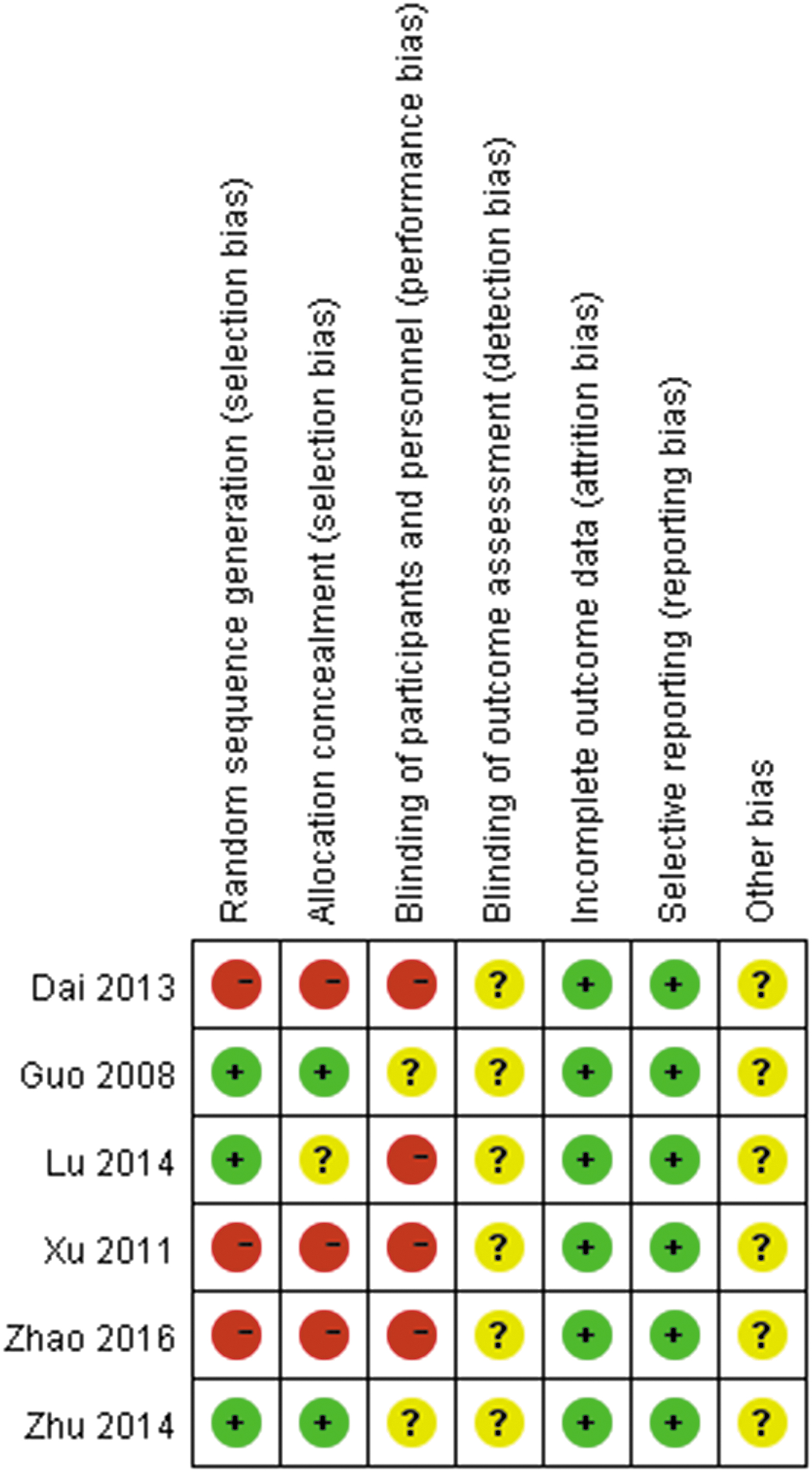
Cochrane's risk of bias assessment tool.
Characteristics of the Included Studies
Characteristics of the Treatment Outcomes
The stent diameter data were reported in three articles and had values of 18–20 mm.12,14,15 The lengths of the stents were chosen based on the obstructed length (obstructed length plus 2 cm at both ends of the tumor).11–16
Dysphagia score
Two of the study reports provided data for the improvement of dysphagia scores,12,16 and we found that the two groups exhibited similar Δdysphagia scores (MD: 0.01; 95% CI: −0.38, P = .40, Table 3). We detected significant dysphagia score heterogeneity between the two studies (I 2 = 89%; P = .0002).
Meta-Analytic Pooled Results of the Secondary Endpoints
CI, confidence interval; MD mean difference; OR, odds ratio.
Stent restenosis
The data of stent restenosis rates were extracted from all studies. We found that there were comparable pooled stent restenosis rates between the two groups (24.7% versus 28.7%, OR: 0.81; 95% CI: 0.51–1.26; P = .35, Fig. 3), and no significant heterogeneity was apparent among the six studies (I 2 = 0%; P = .49).
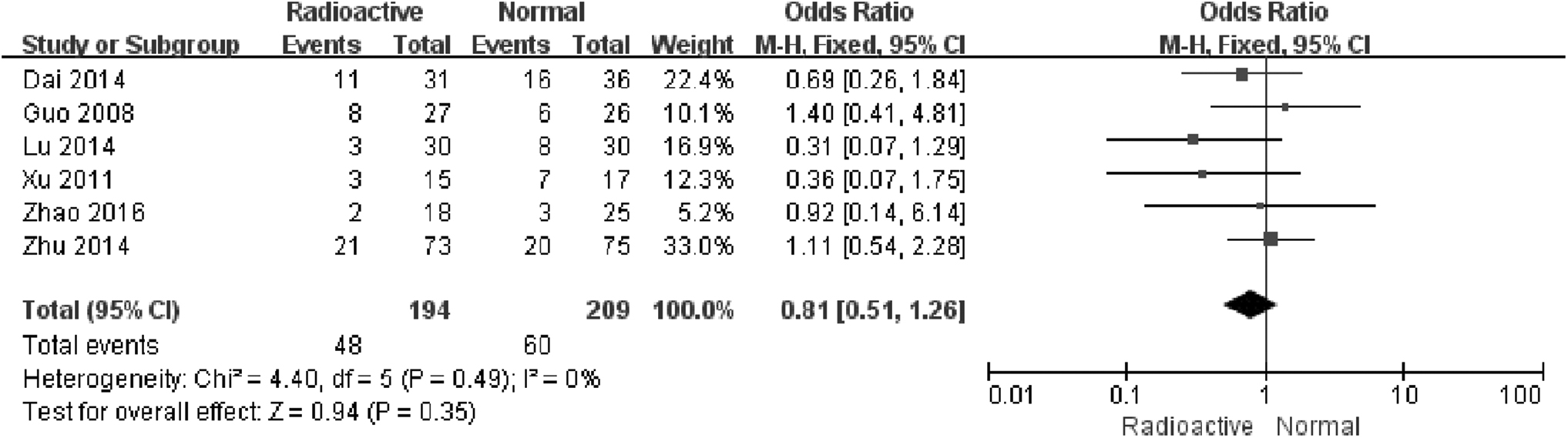
The pooled stent restenosis rates were comparable between the two groups.
Time to restenosis
We were able to extract data for the time to stent restenosis from two reports,12,14 and the pooled time to stent restenosis was significantly longer in the radioactive stent group (MD: 2.53; 95% CI: 1.95–3.11, P < .00001, Fig. 4). We found no significant heterogeneity among these studies (I 2 = 0%; P = .76).

The pooled time to stent restenosis was significant longer in radioactive stent group.
Stent migration
The data for the stent migration rates were available in three of the study reports,12,14,15 and there were comparable pooled stent migration rates between the two stent groups (3.3% versus 4.4%, OR: 0.61; 95% CI: 0.09–4.01; P = .61, Table 3). Two of the studies14,15 found that both the radioactive and normal groups had 0% stent migration rates; therefore, the evaluation of heterogeneity was not applicable.
Survival
We were able to calculate the HR for survival using the data in four articles.11,12,15,16 The survival time was significantly longer in the radioactive stent group (HR: 1.70; 95% CI: 1.47–1.97, P < .00001, Fig. 5), and no significant heterogeneity among the four studies was observed (I 2 = 0%; P = .77).

The pooled survival was significant longer in radioactive stent group.
Severe chest pain
The data for severe chest pain rate were extracted from four studies.12–14,16 We discovered that the comparable pooled severe chest pain rates were comparable between the two groups (22.8% versus 20.3%, OR: 1.16; 95% CI: 0.66, 2.03; P = .61, Table 3). Again, there was no significant heterogeneity found among the four studies (I 2 = 0%; P = .98).
Hemorrhage
Five studies provided data on the hemorrhage rates.12–16 When the hemorrhage rates were pooled for each of the two groups, our analysis found them to be comparable (11.0% versus 9.8%, OR: 1.10; 95% CI: 0.53–2.29; P = .80, Table 3). Furthermore, there was no significant heterogeneity found among the five studies (I 2 = 0%; P = .88).
Fistula formation
The fistula formation rate data could be extracted from three studies,12,14,16 and comparable pooled fistula formation rates were seen between the two groups (6.1% versus 4.2%, OR: 1.42; 95% CI: 0.45–4.45; P = .55, Table 3). No significant heterogeneity studies were observed between these studies (I 2 = 0%; P = .62).
Publication bias
We did not detect any evidence of publication bias pertaining to the selected study endpoints from our funnel plot analyses.
Discussion
In this meta-analysis, we assessed the reported clinical efficacies of the radioactive and normal stent insertion methods for treating patients with MEO. The clinical efficacies were primarily evaluated by comparing the instant effectiveness, long-term effectiveness, and stent-related complications.
Initially, we found similar Δdysphagia scores between two groups (P = .40), which indicate that both normal and radioactive stents can be used to provide rapid symptom relief to MEO patients.
Although various stent types can be used to provide short-term clinical benefits, stent restenosis remains a major problem because it limits long-term outcomes in patients with malignant esophageal, biliary, airway, or superior vena cava obstruction.18–22 The major reasons for stent restenosis are tumor in-growth and overgrowth, followed by fibroepithelial hyperplasia and obstruction by food debris. 18 However, a number of therapeutic strategies, including chemotherapy, external beam radiotherapy, and brachytherapy, have been employed in various efforts to prolong stent patency. 5 Compared with traditional external beam radiation, radioactive seed brachytherapy has been shown to more effectively protect the surrounding tissues by precisely delivering radiation directly to the interior of the tumor. 23
Within the studies, the assessments of stent patency typically included two points: (i) the stent restenosis rate and (ii) time to stent restenosis. It was clear from our meta-analysis that, although the stent restenosis rates were comparable between the two groups (P = .35), the time to stent restenosis was significantly longer in the radioactive stent group (P < .00001). Furthermore, these results are consistent with findings from other studies on radioactive stent insertion in malignant biliary obstruction patients,24,25 which suggests that radioactive seed brachytherapy cannot prevent tumor growth because not all patients were sensitive to this treatment. Nonetheless, radioactive seed brachytherapy was able to inhibit tumor growth and, thereby, prolong stent patency in treated patients.
Another problem with stent dysfunction is the phenomenon of migration. Stent migration usually results from tumor shrinkage after anticancer treatment. However, the stent migration rates were only observed as 3.3% and 4.4% in radioactive and normal groups, respectively (P = .61), which may be attributed to the antimigration design of the esophageal stents. The esophageal stents used are typically designed as a tubular configuration with a drum structure at both ends, 2 and the bilateral drum structure can help in fixing the stent to esophageal wall.
Our analysis of the pooled HR values indicated that radioactive stents significantly improve patient survival, and this finding is consistent with the results of other studies regarding radioactive stent insertion in malignant biliary obstruction patients.24,25 However, a retrospective study into the use of radioactive stents for esophageal squamous cell carcinomas indicated that radioactive stents do not increase survival time, 26 as in that study, many patients died from massive hemorrhage. 26 However, there was a substantial imbalance between the patient numbers in the radioactive (n = 40) and normal (n = 91) groups. 26
The major complications associated with esophageal stents included severe chest pain, hemorrhage, and fistula formation,11–16 and our meta-analysis indicated that radioactive stents do not increase the prevalence of these complications compared with normal stents. These results suggest that radioactive stent insertion is safe for the palliative management of patients with MEO.
This meta-analysis had some limitations. First, although we only included reports of RCTs, the quality of some of the RCTs was deemed low. We subsequently aim to identify higher quality RCTs and to perform further meta-analyses using those reports. Second, none of the included RCTs were double-blind studies; however, unlike in clinical drugs trials, it is almost impossible to use a double-blind study design for the surgical insertion of medical devices. Third, these studies enrolled MEO patients who had several different types of esophageal cancer, and thus, potentially constrained the applicability of our findings. Fourth, all the RCTs were conducted in China; the radioactive stent was developed by Guo et al.'s 12 and, currently, this type of stent is mainly used in China. A more general worldwide study may be possible in the future when the use of the stent has been adopted by more countries.
In conclusion, our meta-analysis demonstrated that radioactive stent insertion can prolong stent patency and the survival of patients with MEO in comparison with normal stent insertion.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.