
Abstract
Background:
Laparoscopic lymph node biopsy through a multi-port access (MPLB) is a well-established technique for intra-abdominal lymphoma diagnosis. The aim of the current study is to assess the feasibility and the diagnostic accuracy of the single-port laparoscopic lymph node biopsy (SPLB) in intra-abdominal lymphoma.
Materials and Methods:
Between October 2016 and February 2019, 15 patients underwent SPLB to rule out or to follow the progression of a lymphoma. The clinical outcome and the pathology reports were analyzed retrospectively.
Results:
SPLB was completed laparoscopically in all cases. The total number of biopsies performed for each procedure was sometimes multiple (median: 2; range: 1–3). Duration of surgery was 85 ± 32 minutes (range: 75–105 minutes). Length of hospitalization was 1.8 ± 0.7 days (range: 1–3 days). No major postoperative complications occurred. A cutaneous infection managed conservatively was observed in a patient. In 10 patients, SPLB was used to establish a diagnosis whereas in 5 patients it was performed to follow a progression of a lymphoproliferative disease.
In 93.3% of the cases, SPLB achieved the correct diagnosis and subsequent therapeutic decisions.
Conclusion:
SPLB has shown good procedure and postoperative outcomes as well as a high diagnostic yield, comparable to literature data on traditional MPLB. Therefore, our results show that this approach is safe and effective and can be an equally valid option to MPLB to obtain a diagnosis or to follow the progression of a lymphoproliferative disease. Further studies are necessary to support these results before its widespread adoption.
Introduction
Studies have shown over time a superiority of laparoscopic lymph node biopsy (LLB) versus core-needle percutaneous biopsy (PB). In fact, in the suspicion of lymphoproliferative disease and when isolated abdominal lymphadenopathy is poorly accessible to PB, laparoscopy is the key tool for making diagnosis.1–3
In the face of greater invasiveness, the laparoscopic single-port approach has recently appeared. It represents a further evolution in laparoscopic surgery, born with the aim of further reducing surgical trauma by reducing the number of abdominal incisions. Since the advent of the first single-incision laparoscopic cholecystectomy described in 1995 by Navarra et al., 4 various other abdominal interventions have benefited from this approach.5–8 Numerous retrospective series on the single-port approach report improved cosmesis and less pain, even if sometimes results are controversial.9,10 To date, there is no documentation on the use of laparoscopic single-port technique for intra-abdominal lymphoma diagnosis. The main experiences are those described by gynecologists for pelvic lymphadenectomy for surgical staging of early uterine cancer.11,12
The purpose of this work is to verify, in addition to the technical feasibility, whether these proposed advantages are also present in the single-port LLB and especially if the good value of diagnostic yield is preserved.
Materials and Methods
In October 2016, laparoscopic single-port surgery was introduced at our Division. Since then, all the single-port laparoscopic lymph node biopsy (SPLB) procedures (n = 15) performed until February 2019 were collected in a prospective database. Patients' details included sex, age, previous abdominal surgery, and associated comorbidities. All the patients included in the study underwent surgery to establish a diagnosis or to follow the progression of a lymphoma. Intra-abdominal lymphadenopathy was present on a computed tomography scan in all patients. All the procedures were performed by the same senior surgeon (MC).
The operative time, estimated blood loss, associated operations, surgical conversion, trocar addition, abdominal drain positioning, length of hospitalization, and postoperative morbidity were the parameters taken into consideration to assess the outcome of the procedure.
Surgical technique
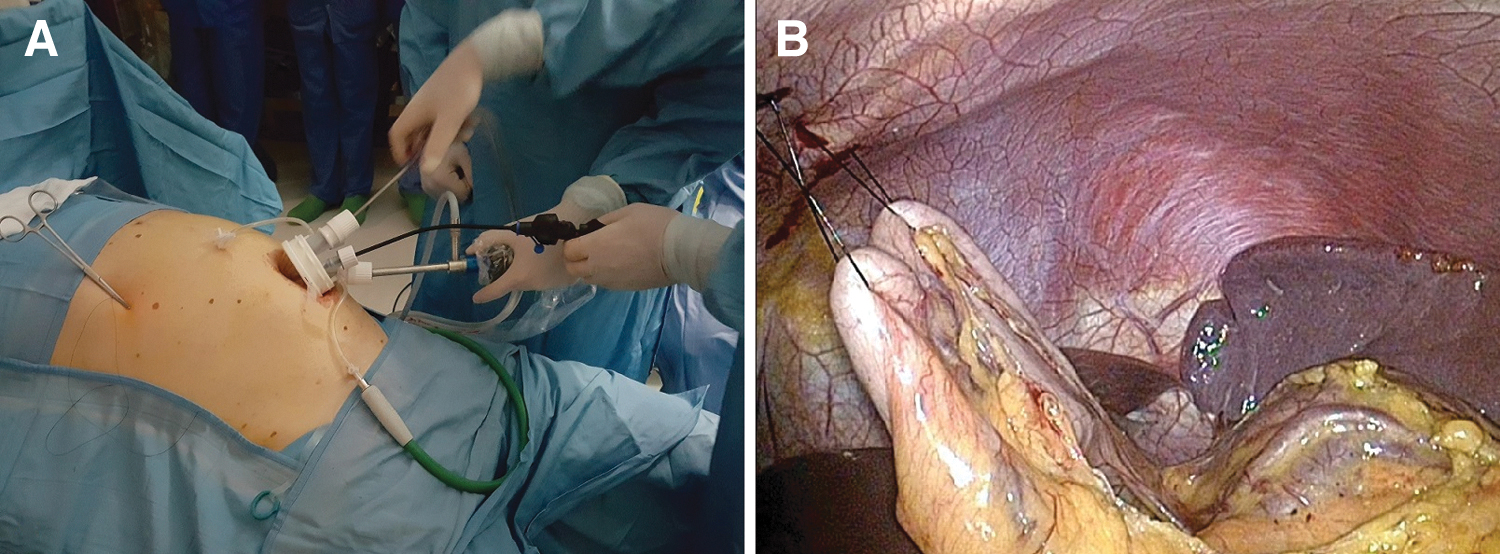
For the SPLB technique, a single port with four channels (Single port, Unimax Medical Systems, Inc., Taipei, Taiwan) is inserted through the umbilicus; a reusable 5-mm hook and a 5-mm reusable prebent grasper (Olympus Medical Systems, Hamburg, Germany) are used for dissection. A radiofrequency device (Ligasure; Covidien Italia, Segrate (Mi), Italy) is often used for dissection as well. The specimen can be extracted with a retrieval bag through the Unimax device once the cap is removed.
According to lymph node location, the technique can be standardized according to two situations: supramesocolic and submesocolic lymphadenopathy. In case of supramesocolic lymphadenopathy (lymph nodes of the celiac axis, hepatic pedicle, splenic hilum, or periaortic position), the patient is placed in reverse Trendelenburg position with the surgeon between the patient's legs. To obtain a better exposition, one percutaneous thread can be passed under the round ligament and used for retraction of the liver. Alternatively, liver retraction can be achieved by using the Versa Lifter™ Band (Surgical Perspective SAS, Strasbourg, France) disposable suspension system, hooked to the right diaphragmatic pillar and to the abdominal wall. If the splenic hilum has to be exposed or in case of difficult access to the celiac axis or to periaortic position, the gastrocolic ligament can be opened and the stomach retracted through sutures passed on its greater curvature (Fig. 1B), according to the “puppeteering technique.” 8
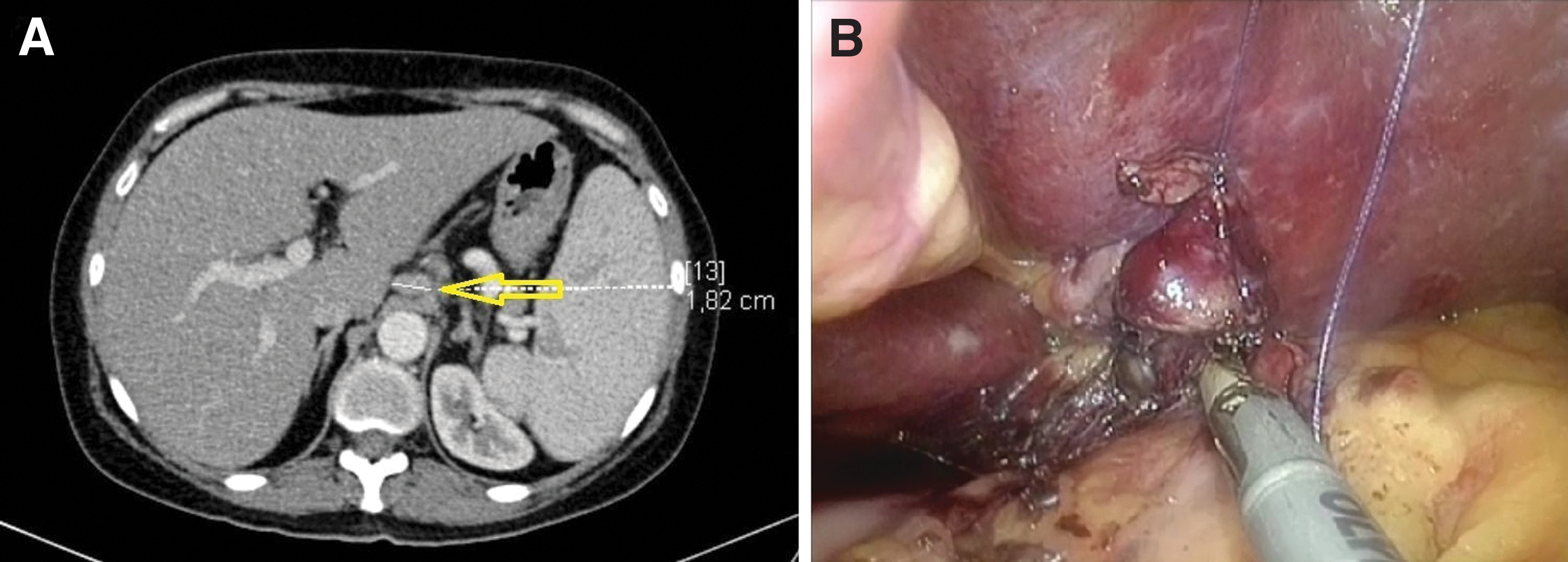
When dissection is made difficult because lymphadenopathy is located deeply or in the vicinity of important vascular structures such as the hepatic pedicle, a suture can be passed on the lymph node to lift it, thus obtaining a better visualization (Fig. 2B). In case of submesocolic lymphadenopathy (lymph nodes of the mesentery, periaortic and periiliac), the surgeon and the camera holder stand on the right side of the patient. A right tilt and mild Trendelemburg position of the table allow to obtain a correct exposure of the root of the mesentery; periaortic lymphadenopathy can be reached as well through an incision of the peritoneum laterally to Treitz ligament (Fig. 3B).

Results
The gender ratio was 9 males for 6 females. The median age of patients was 55.8 years (range: 38–68 years). Previous abdominal surgery was absent. SPLB was completed laparoscopically in all cases. One SPLB patient needed the addition of a trocar due to insufficient exposure of the gastrohepatic ligament, despite lifting the liver by means of a trans-abdominal stay suture passed under the round ligament. An abdominal drain was not necessary in all cases.
Estimated blood loss was <50 mL in 4 patients, and it was absent in the remnant. Abdominal lymph node locations interested in sampling were: periaortic in 6 cases, mesenteric in 4, gastrohepatic ligament in 3, and periiliac in 2.
The total number of biopsies and lymph node stations where biopsy was done during the laparoscopic procedure were sometimes multiple (median: 2; range: 1–3). A liver biopsy was associated in 1 case. Median duration of surgery was 85 ± 32 minutes (range: 75–105 minutes). Length of hospitalization was 1.8 ± 0.7 days (range: 1–3 days). During the postoperative course, one cutaneous infection managed conservatively was observed. In 10 patients, SPLB was used to establish a diagnosis whereas in 5 patients it was performed to follow the progression of a lymphoproliferative disease.
The histopathological diagnosis was non-Hodgkin lymphoma in 8 patients, Hodgkin lymphoma in 4, and sarcoidosis, benign lymphadenopathy, and aspecific inflammatory reaction in 1 patient, respectively.
In 93.3% of the SPLB cases, LLB achieved the correct diagnosis and subsequent therapeutic decisions. One case of false negative was observed in a patient in whom a specific inflammatory reaction was proven at histologic analysis. Due to a suspect past medical history, the laparoscopic biopsy was repeated and led to the diagnosis of large cell anaplastic lymphoma.
Discussion
Surgical excision biopsies of lymph nodes for the diagnosis of lymphoma are recommended whenever possible. 1 In fact, needle biopsies appear inferior to surgical biopsies at providing a correct diagnosis and at identifying lymphoma differentiations. 13 That said, over the years, the minimally invasive surgical approach to the diagnosis of abdominal lymphadenopathy has been imposed on traditional surgery. In fact, conventional laparoscopic lymph node biopsy through a multi-port access (MPLB) has spread thanks to the known advantages of laparoscopy such as pain reduction, shorter hospitalization, earlier resumption of work activity, and, in the case of lymphoproliferative disorders, an earlier onset of chemotherapy.
Although in the gynecological field the use of a single port for pelvic lymphadenectomy for surgical staging of early uterine cancer is established,11,12 there are still no reports on the use of the laparoscopic single-port approach to make a diagnosis or to follow the progression of a lymphoproliferative disease. This is the reason why we wanted to investigate the feasibility and effectiveness of this approach in giving a valid diagnostic response when compared with traditional laparoscopy. The single-port laparoscopic approach has demonstrated its feasibility and efficacy in numerous procedures even if its diffusion has not been widespread due to the limited advantages for the patient in the face of greater technical difficulty.9,10,14
In our study, no surgical conversions and 1 case (6.6%) of trocar addition were reported. Moreover, a drain was never necessary and blood loss was absent in 11 (73.3%) patients. These results testify to the possibility of managing the difficulties connected to the technique. The reason for the reported longer surgical times in single-port surgery are due to the use of instruments that are not appropriate to the technique and to the loss of ergonomics mainly due to the loss of triangulation of the instruments. Notwithstanding, operative times of the SPLB remain acceptable, thus corroborating the validity of the single-port approach. Also, the length of hospital stay showed good results, aligned with the results of other studies where the single-port approach was used.15,16 Morbidity was practically absent in both groups. The only complication that occurred was negligible and did not affect the length of stay. Our data on SPLB surgical outcome are consistent with the conventional MPLB experience reported by the literature. Most studies report a diagnostic accuracy in the 90.4%–95.5% range for LLB, a 5.94%–17.0% conversion rate, and a complication rate in the 1.0%–7.9% range, with no reported mortality.17,18 In our study, a high diagnostic yield was achieved since the correct information for diagnosis and classification was achieved in 93.3% of the patients.
Regarding the surgical technique, some positive considerations must be made on the SPLB approach. The “puppeteering technique” and the round ligament suspension are extremely useful in case of supramesocolic lymphadenopathy, as they allow excellent exposure of the operating field and avoid the use of other forceps and, consequently, the clashing of instruments. Moreover, in case of difficulty, the conversion of an SPLB procedure requires only the addition of one or more trocars, thus avoiding a laparotomy and preserving the mini-invasivity of the procedure itself. Finally, SPLB has the advantage of a single site for the positioning of the device, regardless of the location of the lymph node stations involved in the biopsy. This opportunity avoids the problem of finding the correct positioning of the trocars, especially when multiple biopsies in different abdominal quadrants are planned. This report has also some drawbacks. First, the small number of cases does not allow us to draw strong conclusions. Second, also because only 1 surgeon performed all the procedures, the outcomes reported may not necessarily be repeatable for all surgeons. Unfortunately, the lack of data in literature regarding the single-port approach for LLB prevents us from today expressing a judgment on the potential advantages of this method. Further studies are necessary to support these results before its widespread adoption.
In conclusion, SPLB has shown good procedure and postoperative outcomes as well as a high diagnostic yield, comparable to traditional multi-port LLB. Therefore, our results indicate that this approach is safe and effective in experienced hands and it may represent a valid alternative to MPLB to diagnose or to restage a lymphoma.
Footnotes
Disclosure Statement
Prof. Marco Casaccia, Prof. Roberto Massimo Lemoli, Dr. Emanuele Angelucci, Dr. Stefania Bregante, Dr. Filippo Ballerini, Dr. Adalberto Ibatici, Dr. Chiara Ghiggi, and Prof. Franco De Cian have no conflicts of interest or financial ties to disclose.
Funding Information
No funding was received for this article.