
Abstract
Background:
Obesity treatment requires surgical procedures included in bariatric surgery. Bleeding complications are reported in 1%–4%. Image-guided surgery (IGS) includes minimally invasive procedures that have the advantage of less aggression to the patient, fewer complications, and a quick recovery. Endovascular therapy by interventional radiology (IR) is a minimally invasive image-guided procedure widely used in central, peripheral, and splanchnic vascular pathology. Treatment of postoperative bleeding in bariatric surgery can be aided by image-guided endovascular procedures.
Objectives:
The aim of this study is to carry out an update on the application of IR in bariatric surgery bleeding complications.
Bleeding Complications:
General rate of postoperative complications in bariatric surgery is 0%–10%. Postoperative bleeding (1%–4%) can be gastrointestinal (endoscopic treatment) or intra-abdominal (surgical treatment/relaparoscopy). In the case of arterial vascular lesions that cannot be resolved either endoscopically or surgically, the option of endovascular treatment with IR should be considered.
Conclusions:
Endovascular approach through IR and IGS in bleeding complications after bariatric surgery is presented as a valid minimally invasive therapy option in this group of patients.
Introduction
Obesity is an epidemic that affects people in all countries of the world. 1 Its multidisciplinary treatment requires surgical procedures included in bariatric surgery. 2 Sleeve gastrectomy (SG) and Roux-en-Y gastric bypass (RYGB) are the two most widely used techniques.3,4 Although they are standardized procedures, they are not exempt from morbidities. 5 General complication rate of 0%–10% is reported. Within this situation, bleeding complications are ∼1%–4%, and can seriously compromise the patient's life. 6
The technological evolution applied to medicine has allowed the large-scale development in recent years of image-guided surgery (IGS).7,8 These minimally invasive procedures can be adapted to different fields as far as surgery is concerned. They have the advantage of allowing less aggression to the patient, great versatility in terms of approach options, fewer associated complications, and quick postoperative recovery.
Taking into account the characteristics of the bariatric patient, the current trend is to try to resolve postoperative complications with a minimally invasive approach. 9 Postoperative bleeding in bariatric surgery is no exception, and may be favored by IGS, especially interventional radiology (IR) in endovascular procedures.
Objectives
The objective of this study is to update on the application of IGS, particularly IR, in endovascular therapy of postbariatric surgery bleeding complications.
Bleeding complications
Bariatric surgery
The overall rate of postoperative complications in bariatric surgery is 0%–10%. 10 For SG it is 1%–3% and for RYGB it is 0.2%–3.6%.11,12 The following can be listed: leak, abdominal collection, anastomotic stenosis, bleeding, intestinal obstruction, and acute gastric dilation. 13
Postoperative bleeding represents 1%–4%. It typically manifests with tachycardia, hypotension, paleness, asthenia, and abdominal pain, confirmed by a decrease in hematocrit on laboratory tests. 14 In the case of intra-abdominal bleeding, blood flow can be observed through the drains. In addition, a patient may have a fever in the case of an infected intra-abdominal hematoma produced by a previous bleeding. When the bleeding is gastrointestinal (endoluminal) to the typical picture, the symptoms of upper gastrointestinal bleeding (UGIB) or lower gastrointestinal bleeding (LGIB) (hematemesis or melena, respectively) are added.
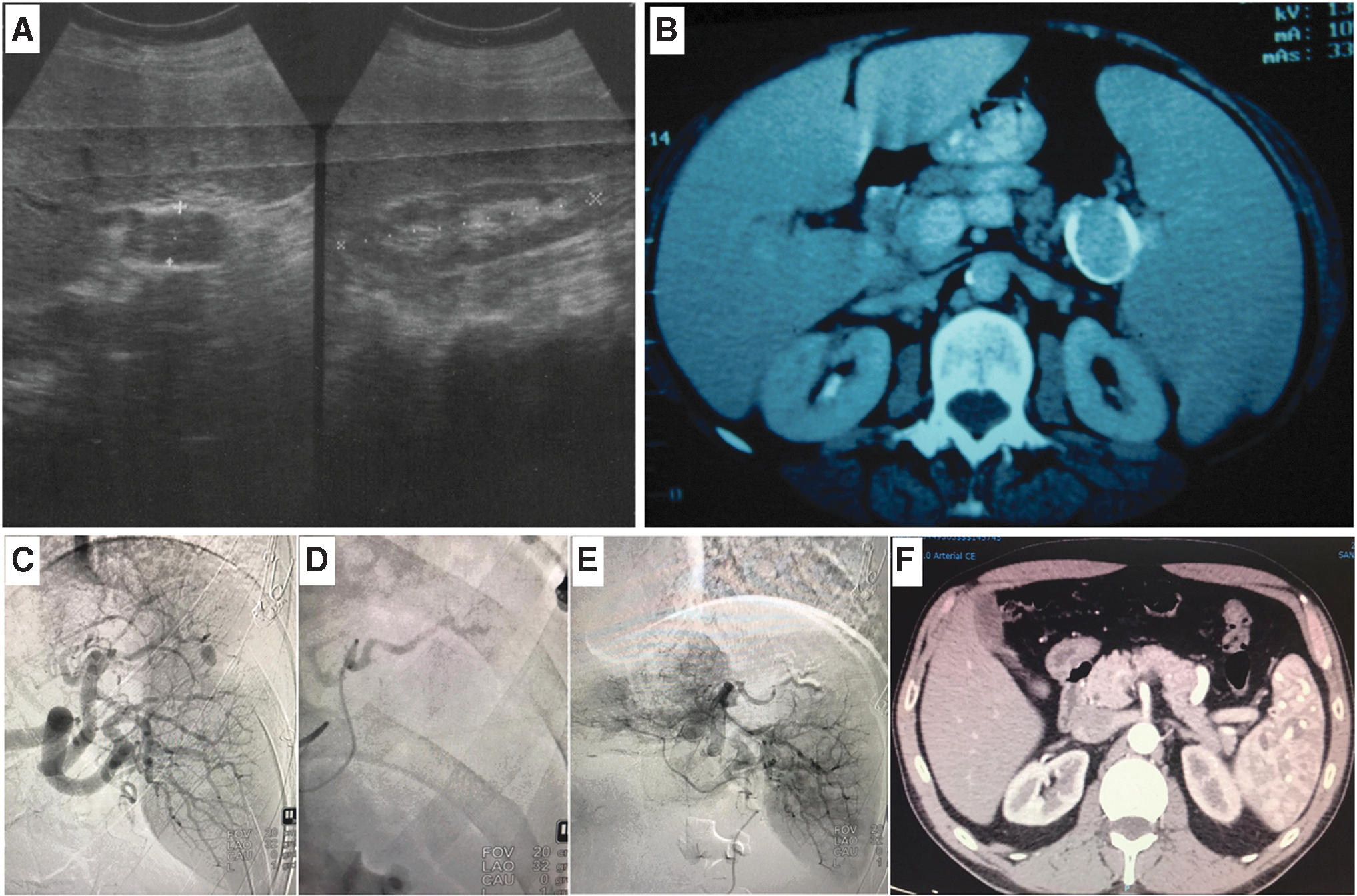
In bariatric surgery, the characteristic sites of bleeding are the staple line of the gastrectomy in SG (Fig. 1A–D), the short gastric vessels, and the gastric suture line and the anastomoses in RYGB.15,16 Less frequently, bleeding originating from the spleen (Fig. 1E) or liver due to iatrogenic lesions is caused by trocars. In contrast, in the presence of abdominal pain without signs of external bleeding, pseudoaneurysm should be considered. 17 It has been described as an infrequent vascular complication that can generate severe bleeding, both in the intraoperative and in the immediate postoperative period. This condition mainly affects the splenic artery, and is usually an imaging finding. When accompanied by UGIB, the presence of a gastrosplenic fistula should be suspected. 18

Bleeding sites in bariatric surgery.
Considering their severity, these situations present a great opportunity for endovascular resolution.
Image-guided surgery
Endovascular therapy by IR is a minimally invasive procedure widely used in central vascular pathology (coronary artery disease) as well as peripheral vascular pathology (carotid, lower limb arteries, etc.). The application in splanchnic (abdominal) vascular pathology is less frequent but no less important. It basically consists of the practices of dilation (stenosis), embolization (hemorrhages), and placement of arterial endovascular stents (stenosis and aneurysms) (Fig. 2) using special devices through a peripheral arterial access, all guided by radiology with intravascular contrast support.

Placement of vascular prosthesis in the celiac trunk due to stenosis.
In digestive surgery, this type of procedure is very useful in the selective embolization of the territory of the gastric arteries (UGIB), in the territory of the inferior mesenteric artery (LGIB), and of the hepatic artery (in the case of chemo or radioembolizations in liver tumors). It is also useful in renal and splenic embolizations due to hemorrhages secondary to thoracoabdominal trauma with great kinematics (Fig. 3).
IGS in postbariatric surgery hemorrhagic complications: Application of IR as endovascular treatment
With regard to bariatric procedures, the vascular territory that can present complications is the upper abdomen. Within this, the potentially affected vessels are the celiac artery, the hepatic artery, the splenic artery, the left gastric artery, and the right gastric artery, less frequently the gastroduodenal artery and the superior mesenteric artery.
Given the suspicion of hemorrhagic complication, there are algorithms that guide its management (Fig. 4). If it is a postoperative bleeding without hemodynamic instability, conservative treatment with fluid management and transfusions should be initiated. 19 In case of severe bleeding, an invasive treatment is chosen. When the bleeding is endoluminal, the first option is endoscopy and local hemostatic treatment. 20 Vasotonic injections or metal clips can be used, among others. In the case of intra-abdominal bleeding, surgical resolution by laparoscopic approach is suggested. A lavage, aspiration, detection of the bleeding site and hemostasis with clip, mechanical suture, or synthetic hemostatic material, and placement of drainage to the bed are performed. For arterial vascular lesions that cannot be resolved either endoscopically or surgically, the option of endovascular IR therapy should be considered. Peripheral access is usually used either radial with introducer or femoral using a 5–7F (French) introducer. When the radial artery is used as access on occasions, the sheathless guide catheter system can be chosen, which does not use sheath. It is inserted directly into the artery, granting a reduction in the radial lumen, allowing an internal lumen close to 6F. This reduces the complications associated with this access, such as spasm and radial occlusion. However, to work on the abdominal vascular territory, the most convenient access is the femoral. Although it should be taken into account that it has a higher rate of complications (hematoma or bleeding at the puncture site). Once inside the vascular system, by manipulating 5–6F catheters, the abdominal arterial territory is accessed, reaching the celiac trunk and its branches. In case of detection of active bleeding, it is embolized with physical means (coils) or chemical means (absorbable hemostatic sponges) 18 (Fig. 3C, E), and if a pseudoaneurysm or an aneurysm is detected, we proceed to the placement of a fully covered stent. 21 Embolizations of the vessels responsible for bleeding must be selective or superselective. This makes it possible to reduce the chances of embolization of a large area and generate undesirable ischemic lesions. This problem can be observed above all in the stomach at the level of the suture line, since it is the site that must bear the greatest stress due to the reduction in blood supply.
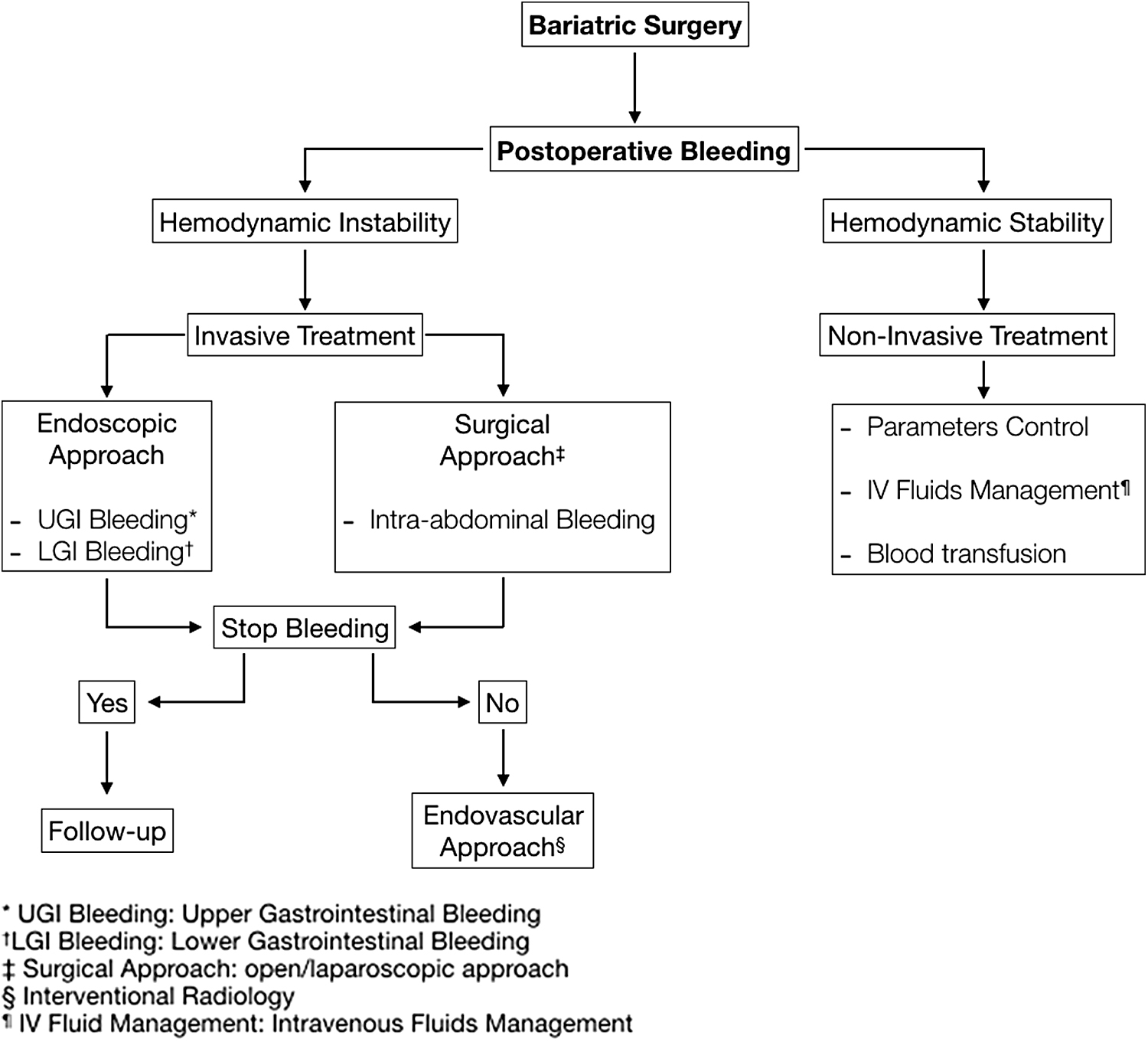
Algorithm for the management of postoperative bleeding in bariatric surgery.
Discussion
As in any procedure, the preparation of both the surgical team and the patient requires reaching certain standards to carry out a safe surgery. 22 This preoperative period is as important as the intraoperative and postoperative period. 23 Although this action does not guarantee a surgical act without complications, at least it tries to reduce them to a minimum, or if they occur, they are as less serious as possible. Regarding bleeding complications, one of the goals of the preoperative stage is to rule out any pathology that affects the patient's coagulation system, and to suspend medications that alter its proper functioning.
During the intraoperative period, several techniques have been described to try to minimize postoperative bleeding. For the gastric section stage, a reinforcement of the staple line with manual suture of resorbable or nonabsorbable material can be used 24 (Fig. 1A–D). In addition, the industry has developed types of mechanical suture with reinforcement of resorbable material. 25 These maneuvers not only prevent bleeding but also stapling line leakage. 26
Despite carrying out all the maneuvers to avoid perioperative bleeding, these are not entirely inevitable. Fortunately, postoperative hemorrhagic complications are not the most common in bariatric surgery. In a meta-analysis by Rausa et al., it was estimated that this type of complications could be associated with the learning curve. 27 When they do occur, most resolve endoscopically or laparoscopically. Depending on their site of origin, they are usually secondary to bleeding from the gastroenteric or enteroenteric anastomosis in the case of RYGB, or from the stapling line, especially in SG (Fig. 1A–D). The latter is less frequent in RYGB. Osland et al. published a meta-analysis wherein bleeding is reported as an early complication in both techniques (SG and RYGB). 28 In cases of gastrointestinal (endoluminal) bleeding, its resolution is endoscopic. 29 If it is intra-abdominal, it is resolved by surgery (relaparoscopy). 30 But if neither approach solves the problem, endovascular treatment should be considered. This is where IGS through IR comes into play. The usefulness of endovascular treatment in abdominal hemorrhagic complications is that it allows treating the responsible vessel when there is active bleeding. The great challenge is to detect the compromised vessel in a highly variable abdominal vascular anatomy.
The literature presents an extensive report on the application of IR in UGIB of gastric origin and in LGIB of colonic origin, especially associated with diverticular disease or vascular dysplasia in the mucosa of the sigmoid colon,31–33 as well as its utility in secondary abdominal bleeding due to trauma (hepatic, renal, and splenic).34–37 But with regard to the treatment of postoperative bleeding complications in bariatric surgery, the literature is short. Only isolated cases of treatment of pseudoaneurysms,21,38,39 gastrosplenic fistulas, 18 or bleeding from the left gastric artery 40 are reported. Endovascular treatment may be useful in bleeding from an anastomosis and from the gastrectomy stapling line, but the truth is that most surgeons do not consider this therapy as a first option. Relaparoscopy is the immediate action in this situation. Naturally, this could be attributable to the surgeon's idiosyncrasy and his attempt to solve a problem secondary to his previous behavior. But we consider that it is necessary to know what the benefits of endovascular treatment would be in this eventuality. It is a minimally invasive procedure and does not require re-entry into the abdominal cavity to perform revision surgery with all that entails. These advantages in the context of a postoperative complication in a morbidly obese patient must be taken into account by the treating surgical team.
Although we consider that IGS together with endovascular treatment applied by IR is highly useful in this group of patients, it is not easy to verify it, since the publications on the subject are scarce, which represents an important limitation in this update work.
Conclusions
IGS approach as endovascular IR treatment in postbariatric surgery bleeding complications is presented as a valid feasible minimally invasive option with good results. It requires that the treating bariatric surgery team be aware of IR and consider it as a treatment option in this group of patients.
Informed Consents
All patients signed an informed consent to participate in research and to allow us to use their data for publication.
Footnotes
Ethical Approval
The approval of our institutional ethics committee was obtained before the start of the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.