
Abstract
Background:
Giant inguinal hernia (GIH) is a rare disease but it can cause serious complications, such as intestinal obstruction and strangulation. Few studies have explored surgical treatment with respect to the transabdominal preperitoneal (TAPP) approach or measures to reduce the occurrence of postoperative seroma.
Purpose:
To investigate the safety and efficacy of the TAPP approach with negative pressure drainage in GIHs.
Methods:
From January 2017 to December 2019, 32 patients who underwent TAPP procedures with negative pressure drainage for GIHs at our hospital were reviewed. Demographic information, surgical characteristics, and follow-up data were obtained.
Results:
The mean age of the patients was 66, and more than half of them had medical comorbidities. All GIHs were defined as Type 1 and were successfully repaired through the TAPP approach with negative pressure drainage. The mean operative time was 146 minutes (range 122–251). After surgery, the mean drainage time was 7 days (range 5–10 days), and the mean volume of drainage in each patient was 820 mL (range 655–1020 mL). Complications occurred in 3 cases. For 1 case, the inferior epigastric artery was injured during surgery. A seroma was observed in 1 patient, which occurred 2 days after removal of the drainage tube. Finally, 1 patient developed an umbilical puncture site infection, and the wound healed after changing the dressing. The mean follow-up was 13 months (range 1–32), and there was no recurrence or mesh infection during that time.
Conclusion:
TAPP is a safe and effective approach for treating Type 1 GIHs with low operative complications. Negative pressure drainage through the scrotum to the preperitoneal space may reduce the incidence of seroma. Recurrence of hernias was not observed, and chronic pain seldom occurred during the follow-up period in our study.
Introduction
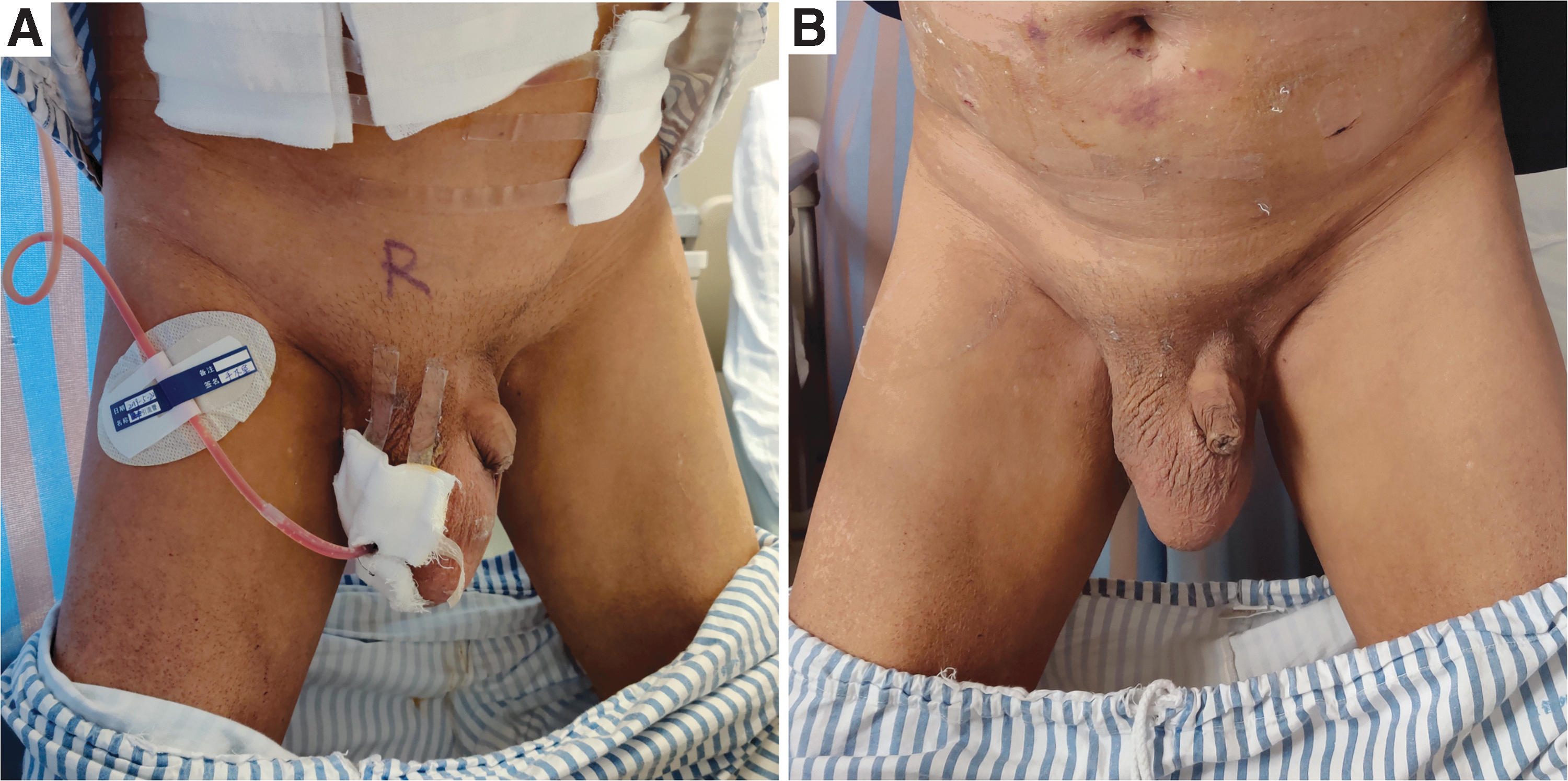
A giant inguinal hernia (GIH) is defined as extending below the midpoint of the inner thigh with the patient in the standing position (Fig. 1).1,2 In developed areas, the incidence of GIH is relatively low because of interventions that occur at an early stage.3,4 However, GIH reduces the quality of life in patients, and in some occasions, it can cause serious complications, such as intestinal obstruction and strangulation.5,6

The hernia sac extends below the midpoint of the inner thigh with the patient in the standing position.
Studies reporting GIH are scant, and most of them are case series. In some cases, the Lichtenstein technique was used and recommended to repair GIH. 7 Meanwhile, resection of abdominal contents and reconstruction of the abdominal wall were implemented in several situations.2,3,8 Nonetheless, few studies have explored the application of laparoscopic techniques, such as a transabdominal preperitoneal (TAPP) approach in these patients. Moreover, surgical treatment of GIHs has a high risk of seroma, especially with the TAPP approach, and few measures have been suggested to reduce the occurrence of postoperative seroma.7,9,10
In this study, the experience of repairing GIH with a TAPP approach and negative pressure drainage in patients referred to a tertiary center is reported. Data concerning complications and follow-up are also described.
Methods
Patients
Hospital records were retrospectively reviewed to identify all patients undergoing TAPP to repair a GIH between January 2017 and December 2019. Eligibility criteria required individuals to have received negative pressure drainage in the preperitoneal space. Recurrent inguinal hernias and irreducible hernias through force were excluded from the study. Demographic information was obtained, and Institutional Review Board approval and informed consent were achieved.
Intervention
All patients received general anesthesia. Prophylactic antibiotics were used before surgery. First, the laparoscope was inserted through a 12 mm umbilical port, and 5 mm ports were placed at the lateral edges of the left and right abdominal rectus muscle. Next, intra-abdominal content in the hernia sac (Fig. 2A) was reduced by pushing the scrotum manually from outside of the body and simultaneously pulling the contents carefully using forceps. If the contents were sticking to the bottom of the hernia sac, scissors or electrocoagulation hooks were used to separate them. Subsequently, the peritoneal flap was carefully dissected, and the edge of the hernia orifice was dissected in a circular manner (Fig. 2B). The hernia sac was left away inside the scrotum and the dissection extended medial to the pubic symphysis, lateral to the anterior superior iliac spine, inferior to the peritoneal reflection, and superior to the conjoined tendon to sufficiently expose the myopectineal orifice. Subsequently, a negative pressure drainage tube was placed in the preperitoneal space through the scrotum (Fig. 2C), and it was connected to a small grenade-type bulb. We used forceps (from the abdominal cavity to the bottom of hernia sac) to grasp the drainage tube and then placed it partially into the peritoneal cavity and the hernia sac. Then, a self-gripping polyester mesh of 15 × 9 cm (ProGrip; COVIDIEN, France) was inserted into the preperitoneal cavity and secured to the myopectineal orifice using absorbable tacks (AbsorbaTack; COVIDIEN, USA) (Fig. 2D). The mesh was fixed over the superior and medial aspects. Finally, the peritoneum was closed with absorbable sutures. The drainage tube was then removed if the drainage volume was <10 mL (Fig. 3). All operative characteristics were collected.
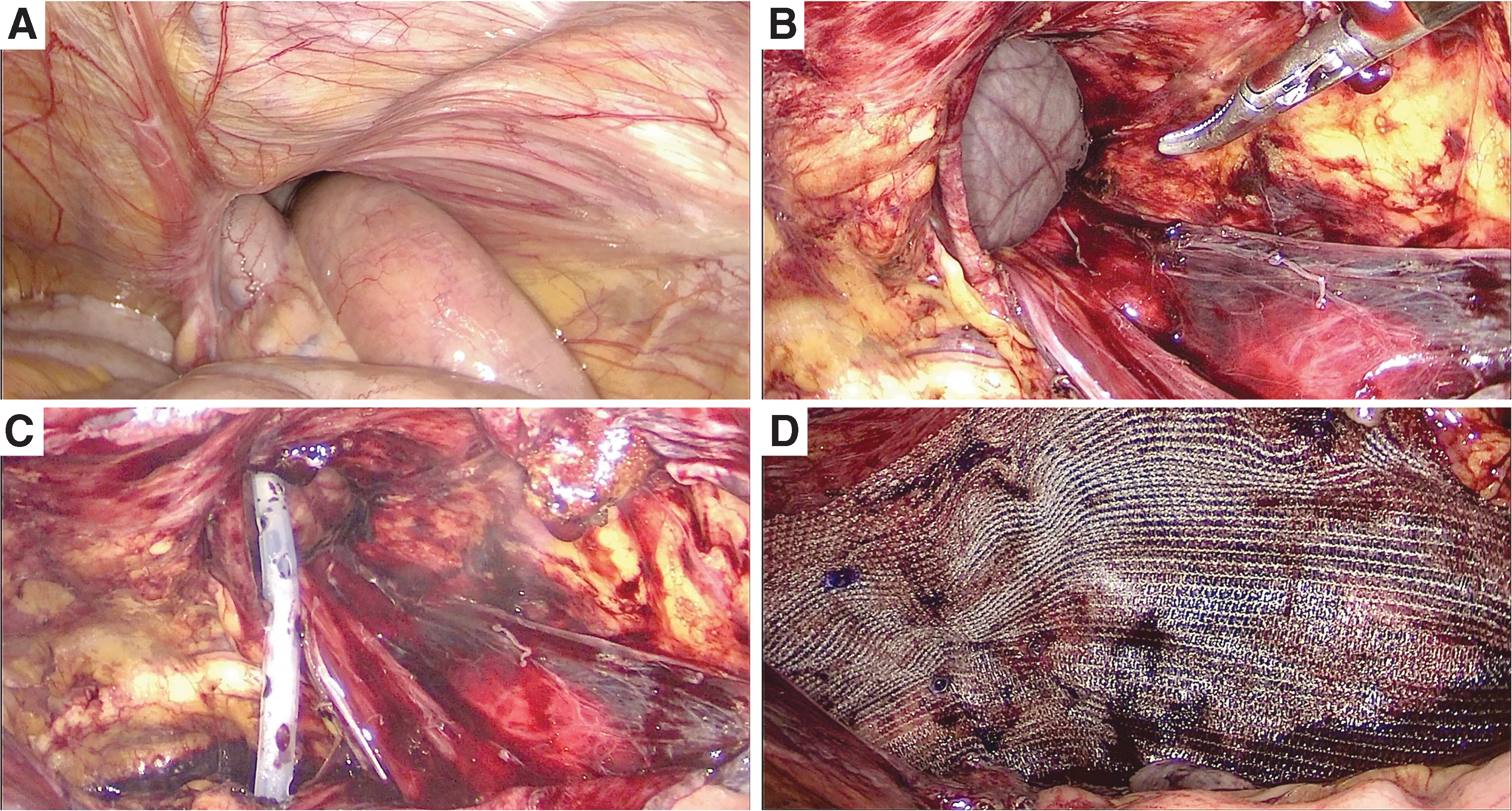
Intraoperative findings of right-sided indirect inguinal hernia.
Complications
Perioperative complications were divided into groups, including subsidiary-injury in the surgery, seroma after surgery, and wound infection. Data were recorded.
Follow-up
Patients returned at 1 and 3 months. After that, telephone follow-up surveys were used every 3 months. If the patient experienced complaints, follow-up was performed at the earliest convenience, usually the same or next day. Chronic pain, recurrence of hernia, and mesh infection were documented.
Statistical analysis
Data were analyzed using SPSS statistical package (Version 18.0, SPSS Inc., Chicago). Continuous variables with normal distribution are presented as the mean ± standard deviation, and otherwise, data are presented as median (range). Categorical variables are presented as number of cases and percentages.
Results
Thirty-two male patients underwent the TAPP approach for GIH repairs. Two patients presented with bilateral hernias, one with a bilateral giant hernia and the other with a giant hernia on one side and a smaller hernia on the other. Median age was 66, and more than half of patients had medical comorbidities. Median body mass index was 25 (range 18–32), including 9% of patients who had a body mass index ≥30. Median American Society of Anesthesiologists classification, as determined by preoperative anesthesia assessment, was 2. Additional preoperative demographics are shown in Table 1.
Patient Demographics (N = 32)
ASA indicates American Society of Anesthesiologists; COPD, chronic obstructive pulmonary disease. Categorical variables are presented as n (%). Continuous variables are presented as median (range).
All GIHs were successfully repaired through the TAPP approach. Eighty-eight percent of them were indirect hernias. Hernia contents included colon, omentum, and small bowel. In all hernia repairs, self-gripping polyester meshes and absorbable fixation devices were used. Median operative time was 146 minutes (range 122–251). In two bilateral hernias, the operative time was 217 and 251 minutes. After surgery, the median drainage time was 7 days (range 5–10), and the mean volume of drainage was 820 mL (range 655–1020). There was usually a small amount of bloody exudate in drainage on the first and second day, and then the content gradually turned transparent and yellowish. Additional surgical data are shown in Table 2 and Figure 4.
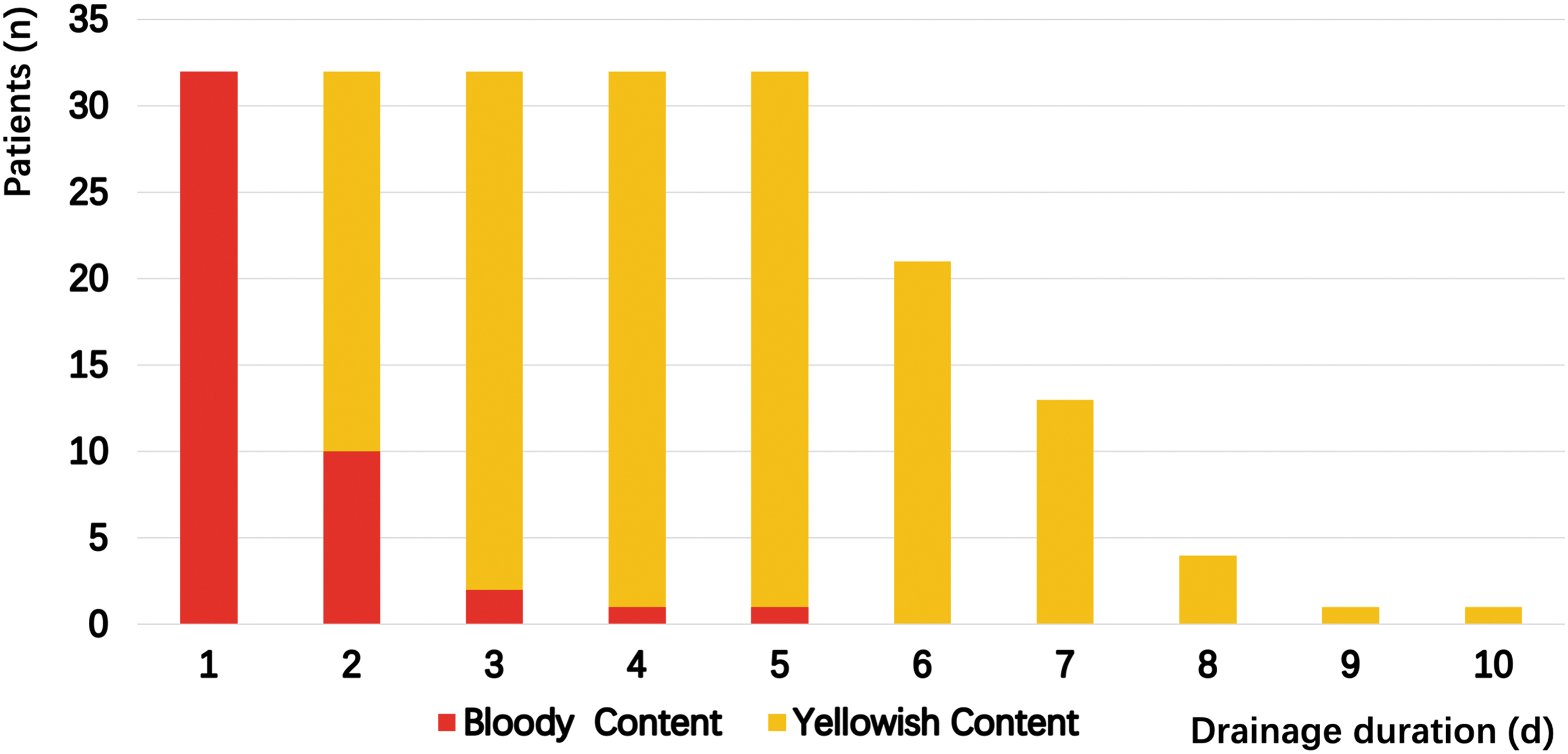
The number of patients with bloody or yellowish content from drainage.
Hernia and Operative Characteristics
Thirty-two patients with 34 inguinal hernias. Categorical variables are presented as n (%). Continuous variables are presented as median (range).
Complications occurred in 3 cases. For 1 case, the inferior epigastric artery was injured during surgery, and ultrasonic scalpel was used for hemostasis. Clinical evident seroma was observed in 1 patient, which occurred 2 days after removal of the drainage tube and was absorbed in 4 weeks without puncture aspiration. One patient developed umbilical puncture site infection, and the wound healed after changing the dressing.
Twenty-nine patients were followed up, and 3 patients were missing. Mean follow-up was 13 months (range 1–32). Two patients (7%) developed chronic pain in the groin region, and symptoms were relieved by medication and local physiotherapy. There was no recurrence or mesh infection during follow-up.
Discussion
In our study, we demonstrated that GIHs were successfully treated through the TAPP approach with negative pressure drainage. Seroma and other complications seldom occurred. Meanwhile, no reoccurrence of hernia was observed during the follow-up period.
Several studies have discussed the repair of inguinoscrotal hernias. The European Hernia Society guideline recommends that Lichtenstein repair is indicated for irreducible or large scrotal inguinal hernias. 11 Guidelines for laparoscopic (TAPP) and endoscopic (totally extraperitoneal [TEP]) treatment of inguinal hernia explained that the TAPP technique could be a therapeutic alternatives in inguinoscrotal hernias. 12 Nevertheless, treatment of GIHs is more challenging and requires more personalized therapy. Trakarnsagna et al. 2 reported that GIHs are categorized into three types based on hernia sac and differential surgical approach. Type 1 GIHs are described as the sac extending below mid-inner thigh but above the middle point of the mid-inner thigh and suprapatellar margin. Forced reduction is feasible in these cases. However, in Type 2 and Type 3 GIHs, forced reduction and simple hernioplasty are impossible, and most cases demand resection of content or increased intraabdominal volume procedure. Generally, open surgery is implemented for GIH repair via abdominal and inguinal incisions,3,8,13 whereas Fujinaka et al. have shown that 4 patients successfully underwent TAPP repair and considered that TAPP might be indicated for Type 1 GIH. 14 In our study, the 32 patients were all diagnosed as Type 1 GIHs, which could be reduced by force, and the TAPP procedure was safe and effective in these cases.
Compared to open surgery, the TAPP approach may be safer and more effective for surgical repair of Type 1 GIHs. 14 First, it reduces wound size because open repair often requires an additional incision to reduce the giant hernia sac.2,8 Furthermore, open surgery with mesh is considered inappropriate in patients with scrotal and inguinal skin infections, but the TAPP approach is possible. Second, it is easier to return hernia contents by pneumoperitoneum and the force from scrotum. The pneumoperitoneum can inflate the intra-abdominal space and possibly reduce the hernia contents. Siow et al. described a similar technique that assists in reduction of incarcerated scrotal hernias. 15 Furthermore, careful manipulation with an appropriate external pressure may reduce the intestines and avoid injury of hernial contents. Finally, separation of the preperitoneal space is sufficient to make the mesh cover the whole defect, potentially decreasing the rate of hernia recurrence.
Although the TAPP procedure has its advantages in some respect, it is not applicable in all cases. For instance, in Type 2 and Type 3 GIHs, forced reduction and simple hernioplasty may not be appropriate because of the loss of domain of the intra-abdominal cavity. Typically, resection of contents or increased intra-abdominal volume procedures, including preoperative progressive pneumoperitoneum, are indicated. 2 On the contrary, TAPP is considered relatively contraindicated in patients with respiratory or cardiac dysfunction. Forced reduction of the massive hernial contents may result in increased pressure in both the abdominal and thoracic cavities, which can lead to abdominal compartment syndrome.
Surgical treatment of GIHs has a high risk of seroma, especially with the TAPP approach. Leibl et al. reported that seroma was the most frequent complication of scrotal hernia with TAPP repair, and 10.5% of these seromas required evacuation via puncture. 9 Misra et al. reported that 21 massive scrotal hernias were repaired via the entirely extraperitoneal approach, and postoperative scrotal seroma occurred in 14 patients (70%), which required needle aspiration. 10 Furthermore, Bierca et al. described the Lichtenstein to repair GIH in 15 patients, and a seroma was found in 3 patients (20%). 7 Our incidence of scrotal seroma was lower than the incidence of the previous study, probably because they placed a drainage tube on the mesh for every patient. Considering the high frequency of postoperative seroma after repair of GIHs, we placed the negative pressure drainage tube in the preperitoneal space through the scrotum in our patients. Meanwhile, Leibl et al. reported that there was no difference in postoperative formation of seroma between complete and incomplete sac dissection. 9 Complete dissection of the GIH sac is challenging in TAPP and may cause hematoma and orchitis due to serious adhesion. Consequently, we did not dissect the sac thoroughly. In our study, seroma occurred in only 1 patient (3%) and was absorbed in 4 weeks without puncture aspiration. We suspect that early removal of the drainage tube is one possible cause of seroma. Thus, we suggest removing the drainage tube if the drainage volume is <10 mL for two consecutive days.
Currently, there is no consensus on the management of scrotal seroma, and the most common intervention is percutaneous aspiration. 16 However, it may increase the risk of introducing infection. Several preventative measures have been advocated to minimize seroma formation, such as obliteration of the dead space by suturing, intraoperative application of fibrin or thrombin, systemic administration of antifibrinolytic agents, delayed postoperative physical activity, pressure dressing, and cauterization of the hernia sac. 17 However, results of these techniques are mostly empirical without evidence-based proof. External compression may help obliterate dead space, prevent shearing of the surgical planes, and promote adherence between the opposite tissues that were used to reduce seroma formation after laparoscopic hernia repairs in our center.
Although retrograde mesh infection did not occur in any of the 32 cases, it remains a controversial issue whether drainage increases the infection rate. A retrospective study, including 321 draining cases and 157 nondraining cases in endoscopic TEP inguinal hernia repair, showed infectious complications were comparable between draining and nondraining groups. 18 A prospective double-blind randomized controlled trial on preperitoneal closed-system suction drainage after TEP hernioplasty also indicated that it was safe and feasible with no infective complications. 19 However, drainage time in the two studies was 23 and 48 hours, respectively, which was less than that in our study. Therefore, more evidence is needed to prove the safety of drainage over a longer duration.
During the follow-up period in our study, 2 patients (7%) suffered moderate chronic pain. Niebuhr et al. analyzed 20,004 patients undergoing the TAPP procedure and reported rates of chronic pain were 4.7%–5.3% for pain at rest and 8.8%–10.1% for pain upon exertion. 20 Wirth et al. stated that 2.4% patients (9/372) complained of chronic pain after TAPP repair with fibrin glue or staple fixation. 21 A prospective study with 146 patients demonstrated that glue fixation decreased the intensity and frequency of pain compared to that experienced preoperatively in patients. 22 The rates for chronic pain in the currently available literature vary between 1.5% and 12%.20,21,23,24 In fact, the genesis of pain is more complex, and more studies are needed to focus on the prevention of postoperative pain. 25 In our report, the rate was similar to the previous studies, and we suspect that chronic pain is related to fixation of the mesh; use of lightweight meshes combined with fibrin glue mesh fixation may decrease the rate of chronic pain. 23
There are some limitations of this study, including its retrospective characteristics and small sample size. The follow-up period was relatively short for investigating the recurrence of hernias, and 3 patients were missing in follow-up. Although we successfully repaired GIHs via the TAPP approach, we still suggest transition to an open anterior approach if the inguinal hernia is irreducible.
Conclusions
TAPP is a safe and effective approach for addressing Type 1 GIHs with low operative complications. Negative pressure drainage through the scrotum to the preperitoneal space may reduce the incidence of seroma. Recurrence of hernias was not observed, and chronic pain seldom occurred during the follow-up period in our study.
Footnotes
Authors' Contributions
Conception and design: H.L., B.T., H.Z., J.S., Y.C., X.Q., and H.W.; Analysis and interpretation: H.L., B.T., H.Z., J.S., Y.C., X.Q., and H.W.; Collection: H.L., B.T., H.Z., J.S., Y.C., X.Q., and H.W.; Writing the article: H.L., H.Z., J.S., Y.C., X.Q., and H.W.; Critical revision of the article: B.T., H.Z., J.S., Y.C., X.Q., and H.W.
Ethical Approval
Institutional Review Board approval and informed consent were achieved.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.