
Abstract
Background:
Recently, in pursuit of minimal invasion, needlescopic surgery (NS) using forceps thinner than the previous standard has garnered attention as a surgical approach to various diseases.
Objective:
We compared the outcomes of NS for gastroesophageal reflux disease (GERD)-related diseases with the conventional method using propensity score-matched analysis.
Subjects and Methods:
Among 205 of 328 cases who underwent laparoscopic fundoplication for the first time from June 2008 to December 2019, excluding 115 cases using mesh and 8 cases undergoing reduced port surgery, 25 subjects in the NS group and 25 subjects in the conventional group were extracted upon propensity score matching for six factors: age, gender, body mass index, degree of esophageal hiatal hernia, duration of intraesophageal acid reflux, and severity of reflux esophagitis.
Results:
The NS group used the Toupet method, whereas the conventional group used the Nissen method for 2 cases and the Toupet method for 23 cases. There were no significant differences between them (P = .490). Although the operative time (143 versus 112 minutes, P = .038) was longer in the NS group, there were no differences in the bleeding volume (nearly equal at 0 mL in both groups), laparotomy conversion rate, intraoperative complications, and postoperative complications (P = .588, P = 1.000, P = 1.000, P = 1.000, respectively). There was also no significant difference in recurrence: 2 cases in the conventional group (8%) and 1 case in the NS group (4%) (P = 1.000). Moreover, the degree of esophageal hiatal hernia, the severity of reflux esophagitis, and the duration of intraesophageal acid reflux all improved after the surgery in both groups (NS group: P = .001, P < .001, P = .002; conventional group: P = .007, P < .001, P = .003).
Conclusions:
The short-term outcomes of NS for GERD-related diseases were good, with a longer operative time but no difference in terms of safety or outcomes compared with the conventional method. This study was approved by the Institutional Review Board of the Jikei University School of Medicine [30-238 (9259)].
Introduction
The standard treatment for diseases related to gastroesophageal reflux disease (GERD) is laparoscopic surgery in Japan as well. Laparoscopic surgery has strived to achieve less invasiveness in recent years. With technological advancements and device development, there have been reports on reduced port surgery (RPS) that reduces the size of wounds compared with standard laparoscopic surgery. RPS includes single-incision laparoscopic surgery (SILS) using only one port, natural orifice translumenal endoscopic surgery (NOTES) using transvaginal and transgastrical laparoscopy, and needlescopic surgery (NS) using forceps with thin diameters, aiming for less invasiveness and improved aesthetic outcomes.1,2
Compared with conventional laparotomy, laparoscopic surgery generally has better aesthetic outcomes and it is a minimally invasive procedure with advantages such as reduced intraoperative bleeding volume, faster recovery of intestinal peristalsis, and shorter postoperative hospital stays.3,4 Compared with conventional laparoscopic procedures, SILS and NOTES have difficulties in terms of operative field deployment and surgical operations due to interference between the forceps. It is also difficult to master these procedures. In contrast, it is assumed that NS can be performed in a similar way as the conventional method by using the same trocar placement. In this study, we compared the outcomes of needlescopic fundoplication (NF) for diseases related to GERD with the conventional fundoplication (CF) using propensity score-matched analysis.
Materials and Methods
Study population
Among 205 of 328 cases who underwent laparoscopic fundoplication for the first time from June 2008 to December 2019, excluding 115 cases using mesh and 8 cases undergoing RPS, 50 subjects (25 subjects in each group) were extracted upon propensity score matching for six factors: age, gender, body mass index (BMI), degree of esophageal hiatal hernia, duration of intraesophageal acid reflux, and severity of reflux esophagitis (Fig. 1).
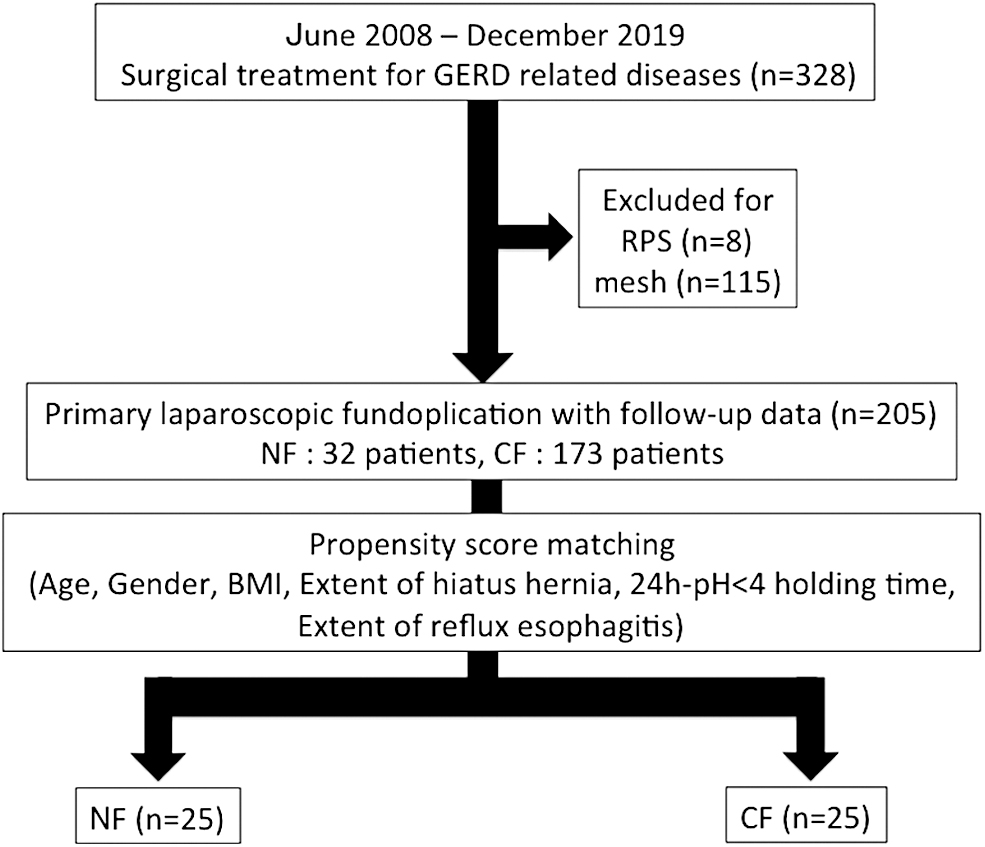
Among 205 of 328 cases who underwent surgical fundoplication for the first time from June 2008 to December 2019, excluding 115 cases using mesh and 8 cases undergoing RPS, 50 subjects (NF: 25 subjects, CF: 25 subjects) were extracted as a result of a matching for six factors: age, gender, BMI, extent of hiatus hernia, 24 hours-pH4HT, and extent of reflux esophagitis. BMI, body mass index; CF, conventional fundoplication; GERD, gastroesophageal reflux disease; NF, needlescopic fundoplication; pH4HT, pH <4 holding time; RPS, reduced port surgery.
Pre- and postoperative assessment
The conditions were evaluated based on the anatomy-function pathology (AFP) classification. 5 In other words, the degree and type of esophageal hiatal hernia were determined using the A factor of the AFP classification (4-scale evaluation from 0 to 3), the duration of intraesophageal acid reflux was determined using the F factor (4-scale evaluation from 0 to 3), and the degree of reflux esophagitis was determined using the P factor (4-scale evaluation from 0 to 3). Postoperative recurrence was defined as hernia recurrence above A1 upon contrast radiography of the upper gastrointestinal tract or upper gastrointestinal endoscopy, or erosive esophagitis at Los Angeles classification grade A or higher upon upper gastrointestinal endoscopy. 6 The evaluation of postoperative esophagitis used the latest results, whereas the duration of acid reflux was evaluated 3 months after surgery.
Twenty-four hours esophageal pH monitoring
Multichannel intraluminal impedance pH monitoring was used for evaluation. Sleuth and a catheter made by Sandhill were used. The catheter was nasally inserted under X-ray fluoroscopy, with the distal end thereof (distal sensor) placed in the stomach and the proximal sensor placed 5 cm superior to the top end of lower esophageal sphincter (LES). During the examination, food intake included only three meals of hospital food, with food prohibited between meals and only drinking water permitted under 24-hour continuous monitoring. Software was used to conduct automatic analysis for data analysis. 7 As a parameter, esophageal pH <4 holding time (pH4HT) was calculated as the duration of esophageal acid reflux. The duration of acid reflux after surgery was evaluated 3 months after surgery.
Surgical method and trocar used
In CF, two 12 mm ports were used for the umbilical region and upper left abdomen, whereas two 5 mm ports were used for the upper right abdomen and left abdomen. To elevate the liver lateral region, Nathanson liver retractors (Iron Intern®) were inserted directly from the fossa; alternatively, 5 mm ports were inserted and a snake retractor (Diamond-Flex®) was used. For the NF, a 12 mm port was indwelled in the umbilical region, a 5 mm port was indwelled in the left upper abdomen, and one 3 mm port was indwelled in each of the right upper abdomen and left abdomen, respectively. The procedure of laparoscopic fundoplication is detailed in the previous report. 8 Both procedures were conducted as follows: exposing and reserving the abdominal esophagus, resection of the short gastric artery/vein and crural repair, and prevention of gastroesophageal regurgitation using the Nissen method or Toupet method.
Assessment of surgical findings
Regarding the surgery, we examined operative time, estimated blood loss, intraoperative complications, laparotomy conversion rate, postoperative hospital stay, and postoperative complications.
Statistical analysis
A statistical examination was carried out using the SPSS program (version 23.0; SPSS Inc., Chicago, IL). All data were described as the median and interquartile range, with P < .05 defined as a statistically significant difference according to the Wilcoxon signed-rank test and chi-squared test. One-to-one propensity score matching was adopted to overcome any potential bias arising from a lack of randomization as a consequence of the different covariable distribution among patients. Matching was performed by calculating the propensity scores using the following predictors: age, gender, BMI, extent of hiatus hernia, pH4HT, and extent of reflux esophagitis.
Results
Demographic data
As patient characteristics (Table 1), we performed matching for six factors: age, gender, BMI, extent of hiatus hernia, pH4HT, and extent of reflux esophagitis. No significant differences were found in the duration of illness, factor F, and factor P for which matching was not performed (P = .806, P = .670, P = .585, in the same order).
Demographic Data Between the Two Groups
Anatomy–Function–Pathology classification.
BMI, body mass index; CF, conventional fundoplication; NF, needlescopic fundoplication; NS, no significant; pH4HT, pH<4 holding time.
Surgical findings
Although operative time was longer in the NF group (143 versus 112 minutes, P = .038), there was no difference between the two groups in terms of the procedure, estimated blood loss, laparotomy conversion rate, intraoperative complications, postoperative hospital stay, postoperative complications, follow-up period, and recurrence rate (P = .490, P = .588, P = 1.000, P = 1.000, P = .180, P = 1.000, P = .170, P = 1.000, respectively) (Table 2).
Surgical Findings Between the Two Groups
CF, conventional fundoplication; NF: needlescopic fundoplication.
Postoperative outcomes
In both the NF group and CF group, there was significant improvement after surgery in terms of factors A, F, and P; Los Angeles classification; and pH4HT (Table 3).
Postoperative Outcomes Between the Two Groups
Anatomy–Function–Pathology classification.
CF, conventional fundoplication; NF, needlescopic fundoplication; pH4HT, pH <4 holding time.
Discussion
NS is defined as a laparoscopic surgery using forceps with a fine diameter of ≤3 mm for fine-diameter trockers. 2 In general, thinner trockers enable smaller cutaneous incisions of the wound, reducing wound pain and improving aesthetic outcomes after surgery. However, because thinner forceps are used, the difficulty of surgery is thought to be higher in terms of maneuvers such as grasping, traction, and suturing of the organs.2–4 Although reports do exist on NS for other diseases, there are only few overseas reports on the outcomes of NS for diseases related to GERD and none in Japan.
In this study, as a result of examination after removing the bias as much as possible using propensity scoring matching, although only the duration of surgery was significantly longer in the NF group, there was no difference in the relapse rate between the two groups and significant improvement was observed after surgery for both groups. The surgical time was extended possibly because the 3 mm forceps had inferior organ gripping/traction power than 5 mm forceps and the view field development took more time, increasing the difficulty of surgery. In contrast, it was revealed that CF and NF had comparable safety and therapeutic effects. Pace et al. 9 performed matching for age, gender, weight, and history of abdominal surgery and compared the NF and CF. As a result, both groups included 38 subjects, with no significant differences in the duration of surgery (143 versus 127 minutes), bleeding volume (54 versus 48 mL), intraoperative complication (2.6% versus 2.6%), and postoperative hospital stay (1.8 versus 1.5 days). However, no matching of pathology was performed in this study. Abbas et al. 10 carried out a randomized clinical trial (RCT) of Laparoscopic Nissen fundoplication using fine-diameter forceps. As a result, there were 7 cases in NF and 6 cases in CF, with no difference in the duration of surgery. This report on RCT includes very few cases. There are no articles comparing the pathology before and after surgery with objective parameters. Therefore, there have been no reports on NF with a high level of evidence. In our report on this retrospective study, we conducted a comparison involving the matching of patient characteristics and pathology, which is thought to be meaningful.
This study includes several limitations: (1) Short observation period, (2) no postoperative pain assessment, and (3) no questionnaire on aesthetic outcomes. Although the invasiveness could not be evaluated from the perspectives of (2) and (3), we were able to prove the equivalence of the safety and curative effects. Going forward, we believe the accumulation of subjects, an extended follow-up period, and an evaluation of the postoperative pain and aesthetic outcomes are necessary.
Conclusions
The short-term outcomes of NF for diseases related to GERD were good, with a longer operative time but no difference in the safety or outcomes compared with the CF.
Footnotes
Ethical Statement
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. Informed consent or substitute for it was obtained from all patients for being included in the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.