
Abstract
Background:
Radical surgery is recommended for high-risk pathological stage T1 (pT1) or pT2 rectal cancer after transanal endoscopic microsurgery (TEM). However, in clinical practice, many patients may unfit or decline radical surgery. In recent years, adjuvant chemoradiotherapy (CRT) after TEM was considered as an alternative to radical surgery for these patients. This study aimed to assess oncological outcomes of adjuvant CRT after TEM for high-risk early rectal cancer.
Materials and Methods:
We collected retrospectively data of 97 patients who underwent TEM with pT1 and pT2 between January 2008 and December 2018. Of these, 35 patients were excluded. Of the remaining 62 patients, 42 were managed by TEM alone and 20 by TEM plus adjuvant CRT. Demographics, recurrence, and survival were analyzed between the two groups.
Results:
At a median follow-up of 52.5 months, the 3-year local recurrence-free survival and disease-free survival (DFS) in TEM alone group were significantly lower than those in TEM+CRT group (66.6% versus 93.3%, P = .035; 63.7% versus 93.3%, P = .022). Although the 3-year overall survival in TEM+CRT group was higher than TEM alone group (100% versus 83.3%), the difference was not statistically significant (P = .13). The local recurrence rate in TEM alone was 31%, compared with 5% in TEM+CRT group (P = .025). Multivariate analysis showed that adjuvant CRT was an independent prognostic factor for DFS (hazard ratio: 0.094; 95% confidence interval: 0.001–0.764; P = .027).
Conclusions:
Our study suggests that adjuvant CRT after TEM may be an alternative for pT1 high-risk and T2 rectal cancer who are not suitable or unwilling to undergo salvage radical surgery.
Introduction
Radical surgery with total mesorectal excision has long been the standard treatment for rectal cancer 1 ; however, local excision is an appropriate alternative to major surgery in well-selected early rectal carcinoma. 2 Transanal endoscopic microsurgery (TEM) as a surgical method of local excision, first described by Buess in 1983, 3 had proved to be technically superior to conventional transanal local excision with precise resection margin, wide vision, lager operating space, and significant lower local recurrence rates.4–6 At present, TEM has become the gold standard for the excision of large adenomas and selected early rectal cancer.
TEM has many advantages in complication rate, hospital stay, quality of life, morbidity, and mortality in the treatment of early rectal carcinoma compared with radical surgery. 7 However, despite the benefits of TEM are obvious compared with radical surgery, TEM was still controversial in the treatment of early rectal cancer. The high local recurrence rate and the risk of lymph node metastasis of TEM for early rectal cancer were still a question. A Norwegian study 8 compared outcomes after TEM and total mesorectal excision (TME) in the treatment of early rectal cancer reported that the 5-year local recurrence rate after TEM was 14.5% versus 1.4% after TME in patients with T1 rectal cancer, and 5-year local recurrence rate was 11.4% versus 4.4% in T2 lesion.
A diversity of factors was related to high local recurrence after TEM for early rectal cancer. Potential lymph node metastasis in mesorectal was likely to mainly account for local recurrence. Although the preoperative imaging examinations showed no lymph node metastasis, those similar to normal lymph nodes in size are difficult to diagnose. The limitations of clinical imaging may lead to inaccurate preoperative tumor staging. Therefore, it is common that histopathological evaluation of rectal cancer specimens after TEM usually shows that the tumor is more advanced than previously predicted or has unforeseen adverse features, such as poor differentiation, lymphovascular invasion (LVI), perineural invasion, and submucosal invasion ≥1 mm, which all was associated with the relapse.
It is generally believed that TEM alone can provide acceptable oncological and functional outcomes for patients with T1 low-risk rectal cancer, 9 but it is not sufficient when the adverse histopathological features or more advanced tumors are present. According to guidelines of National Comprehensive Cancer Network (NCCN), patients whom pathological findings after TEM showed stage T1 with high-risk features or stage T2 were advised to perform completion radical surgery 10 ; however, many patients in clinical practice may be medically unsuitable or refuse radical surgery because of a diversity of factors, such as a strong desire to preserve the anus, the high mortality and complications associated with radical surgery. A couple of studies have shown that adjuvant (chemo)radiotherapy after local resection has a potential to decrease the risk of local recurrence11–13 by sterilizing occult metastatic lymph nodes in mesorectum and residual cancer cells within the rectal wall at the time of local resection. Therefore, adjuvant chemoradiotherapy (CRT) after TEM might be an alternative to radical surgery for these patients.
However, the role of adjuvant CRT after TEM was still controversial. Our retrospective single-center study was to evaluate oncological outcomes of adjuvant CRT after TEM as an alternative to radical surgery in patients with pathological stage T1 (pT1) high-risk and pT2 rectal cancer.
Materials and Methods
Patients
Date of patients who were operated by TEM with pT1 and pT2 between January 2008 and December 2018 were collected. The data included gender, age, T stage, tumor diameter, distance from the anal verge, tumor differentiation, resection margin, LVI, perineural invasion, serum carcinoembryonic antigen (CEA). All the patients needed to receive preoperative assessment, including clinical imaging (endorectal ultrasound, chest-abdominal computed tomography [CT], and pelvic magnetic resonance imaging [MRI]), colonoscopy with biopsy, and blood tests. Basing on histopathological results of the specimen after TEM, we defined T1 high-risk as resection margin positive, and/or tumor diameter >3 cm, and/or poor differentiation, and/or LVI, and/or perineural invasion. All patients signed informed consent forms and the current study was approved by the Ethics Committee of the Fist Affiliated Hospital of Shandong First Medical University.
Surgery and adjuvant therapy
To select the appropriate surgical position according to the tumor location, the tumor should be placed as far below the visual field as possible after the placement of TEM colonoscopy. Full-thickness resection was operated while securing a horizontal margin of 1 cm from the tumor. Adjuvant CRT as follow-on treatment after TEM started at 6–8 weeks after confirming complete healing of the TEM site endoscopically. The dose and frequency of radiotherapy were determined by the experienced oncologist in our radiotherapy center according to the guidelines. Radiation doses commonly were 45.0–50.4 Gy in 25–28 fractions for 5 weeks, with concurrent oral Capecitabine 825 mg/m2 twice daily 5 days per week. The radiation therapy fields are generally the same as standard fields for rectal cancer, including the TEM site, mesorectum, and lateral pelvic walls.
Follow-up
All the patients followed up on the outpatient clinic regularly. The initial follow-up is required 1 month after TEM to evaluate the TEM site healing by colonoscopy. Patients received examinations, including physical examination, digital rectal examination, colonoscopy, chest-abdominal CT and pelvic CT/MRI, and tumor markers every 3 months for 2 years, every 6 months up to the fifth year postoperatively, and yearly thereafter. Local recurrence was defined as detection of newly developed soft tissue lesion in rectum or lymph node metastasis in pelvic on CT or MRI, and pathological confirmation was eventually required for the diagnosis of local recurrence.
Statistical analyses
Statistical analyses were conducted by using SPSS software, version 24.0. Pearson chi-square test and Fisher exact test were used for categorical data. Kaplan–Meier method was used to calculate the overall survival (OS), local recurrence-free survival (LRFS) and disease-free survival (DFS), and the log-rank test was used to test differences in outcomes. Using the univariate analysis screened the potential prognostic factors and a Cox proportional hazards regression model was used to further identify independent risk factors in multivariate analysis. Baseline variables with a P < .2 in univariate analysis or considered clinically relevant were entered into a multivariate model. P < .05 indicated a statistically significant difference between the two groups. OS was calculated from the date of TEM to the date of death from any causes or the last follow-up. LRFS was calculated from the date of TEM to the date of cases confirmed of local recurrence or last follow-up, or death from any cause. DFS was calculated from the date of TEM to the date of appearance of local recurrence or metastatic disease, or death from any cause, or last follow-up.
Results
Patient and tumor characteristics
A total of 97 patients who underwent TEM with pT1 and pT2 were selected. Of these, 9 patients with a history of malignant tumor, 2 patients with a loss to follow-up, 3 patients who operated salvage radical surgery after TEM, and 21 patients with pT1 low-risk were excluded from analysis, the remaining 62 patients with pT1 high-risk and pT2 were eventually enrolled in this study. Of these 62 patients, 42 (67.7%) were operated by TEM alone and 20 (32.3%) by TEM plus adjuvant CRT. Twelve patients in TEM+CRT group were treated by radiotherapy in combination with capecitabine, 8 patients were only treated by radiotherapy. The flowchart of included patients is shown in Figure 1.
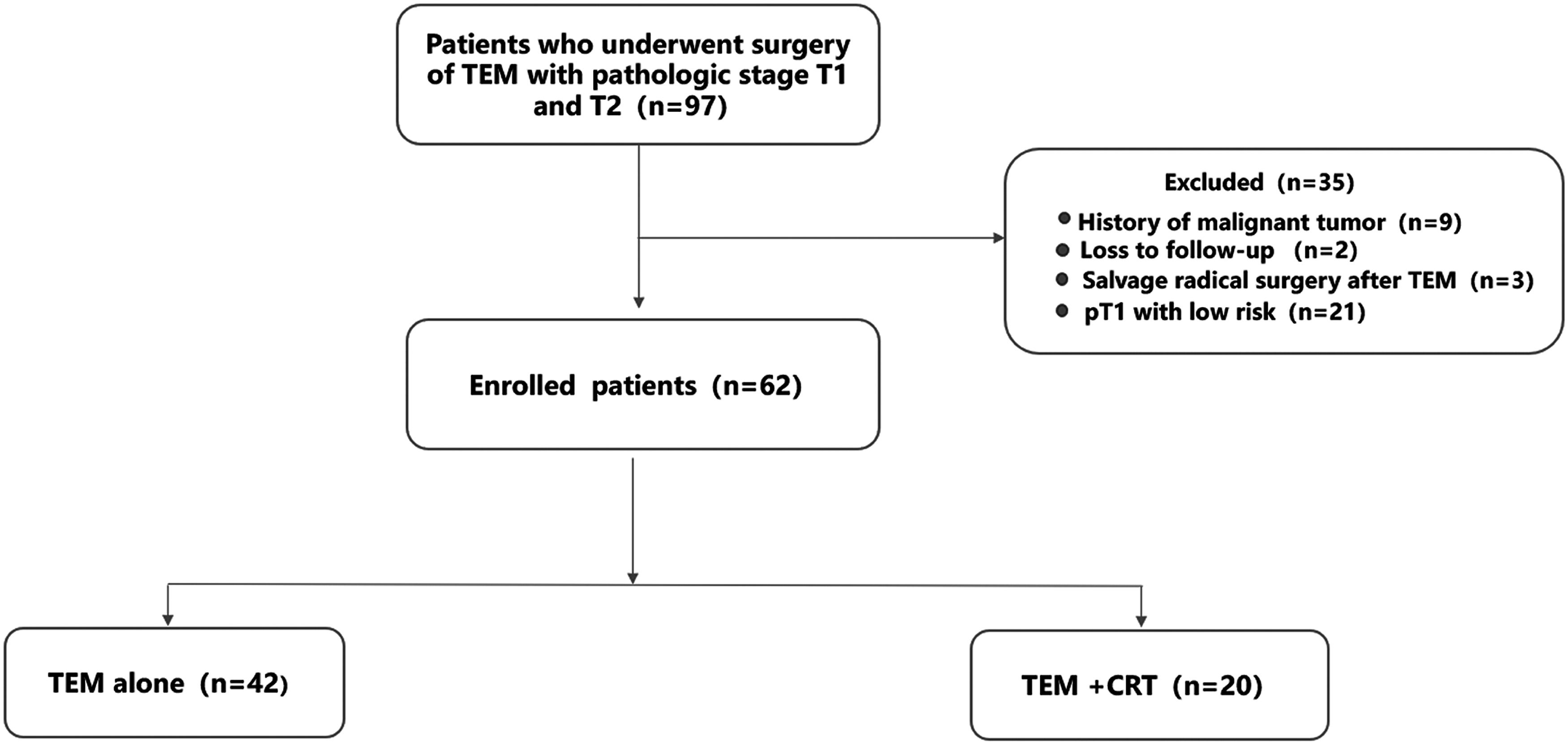
Protocol flowchart. CRT, chemoradiotherapy; pT, pathological stage; TEM, transanal endoscopic microsurgery.
There were 35 males (43.5%) and 27 females (56.5%), the median age of all patients was 62 years (range 25–83). The median age in TEM alone group was older than that in TEM+CRT group and the median age in TEM alone group was 63 years (range 25–83) compared with 56 years (range 39–77) in TEM+CRT group. The proportion of T stage of the two groups was as follows: 31 (73.8%) pT1 high-risk and 11 (26.2%) pT2 in TEM alone group, 5 (75%) pT1 high-risk, and 15 (25%) pT2 in TEM+CRT group. There were no differences between two groups in gender, age, distance from the anal verge, tumor differentiation, resection margin, LVI, perineural invasion, serum CEA, but there were significant differences in T stage (P < .001) and tumor diameter (P = .004), showing that TEM alone group had significantly more T1 high-risk and tumor diameter >3 cm compared with TEM+CRT group. Patient and tumor characteristics are shown in Table 1.
Patient and Tumor Characteristics
CEA, carcinoembryonic antigen; LVI, lymphovascular invasion; pT, pathological stage; TEM, transanal endoscopic microsurgery.
Survival outcomes
Recurrence was observed in 15 patients (24.2%) and 6 patients died. Five of the 6 patients with death were related to recurrent cancer and the other died as a result of coronary heart disease. At a median follow-up of 52.5 months, the 3-year OS, LRFS, and DFS in TEM alone group was 88.8%, 66.6%, and 63.7%, respectively, compared with 100%, 93.3%, 93.3% in TEM+CRT group, respectively. The difference of LRFS (Fig. 2) and DFS (Fig. 3) between the two groups had statistical significance (P = .035; P = .022, respectively). Although the 3-year OS in the TEM+CRT group was higher than the TEM alone group, the difference was not statistically significant (P = .13) (Fig. 4).
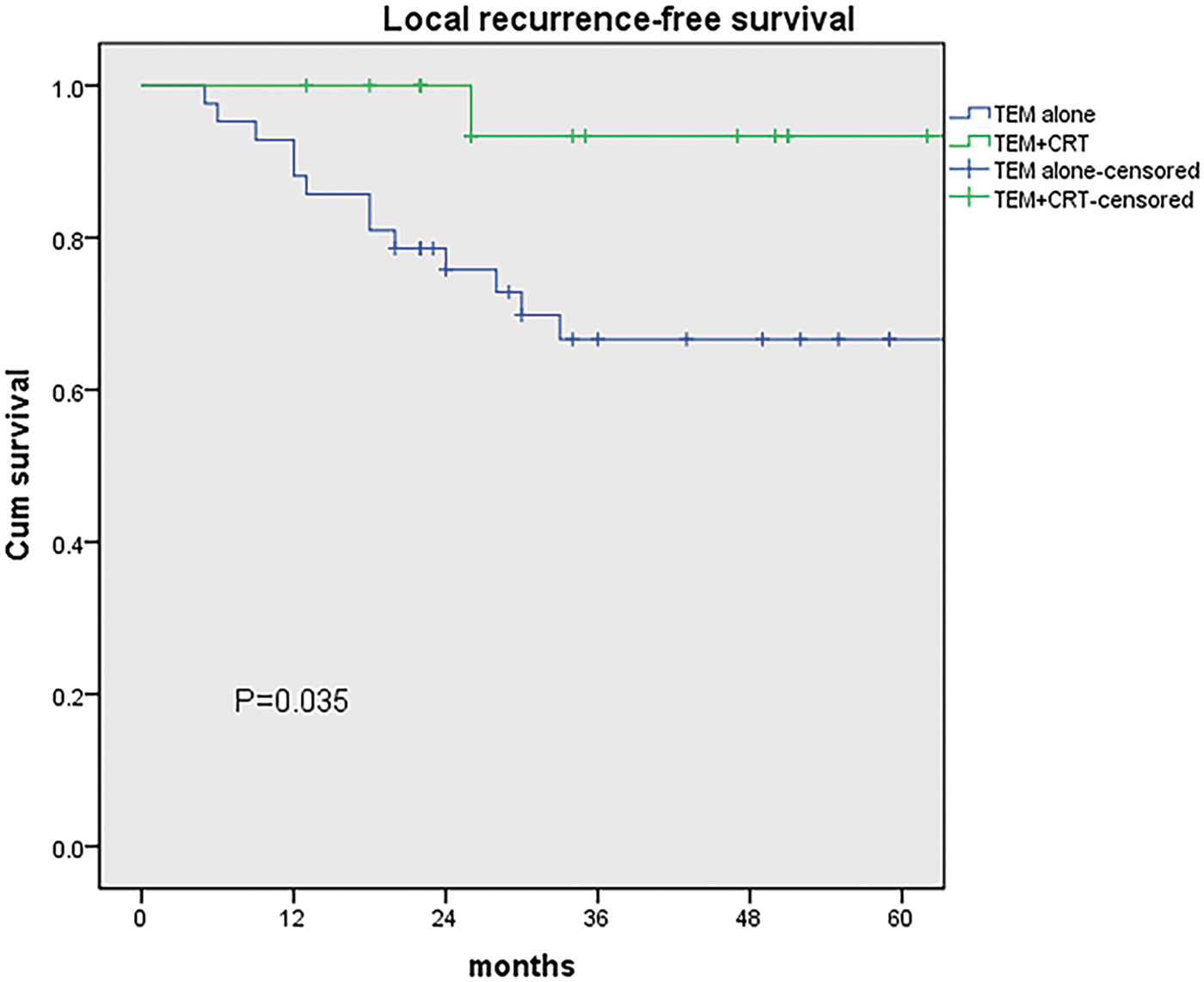
Kaplan–Meier survival curves of local recurrence-free survival. CRT, chemoradiotherapy; TEM, transanal endoscopic microsurgery.
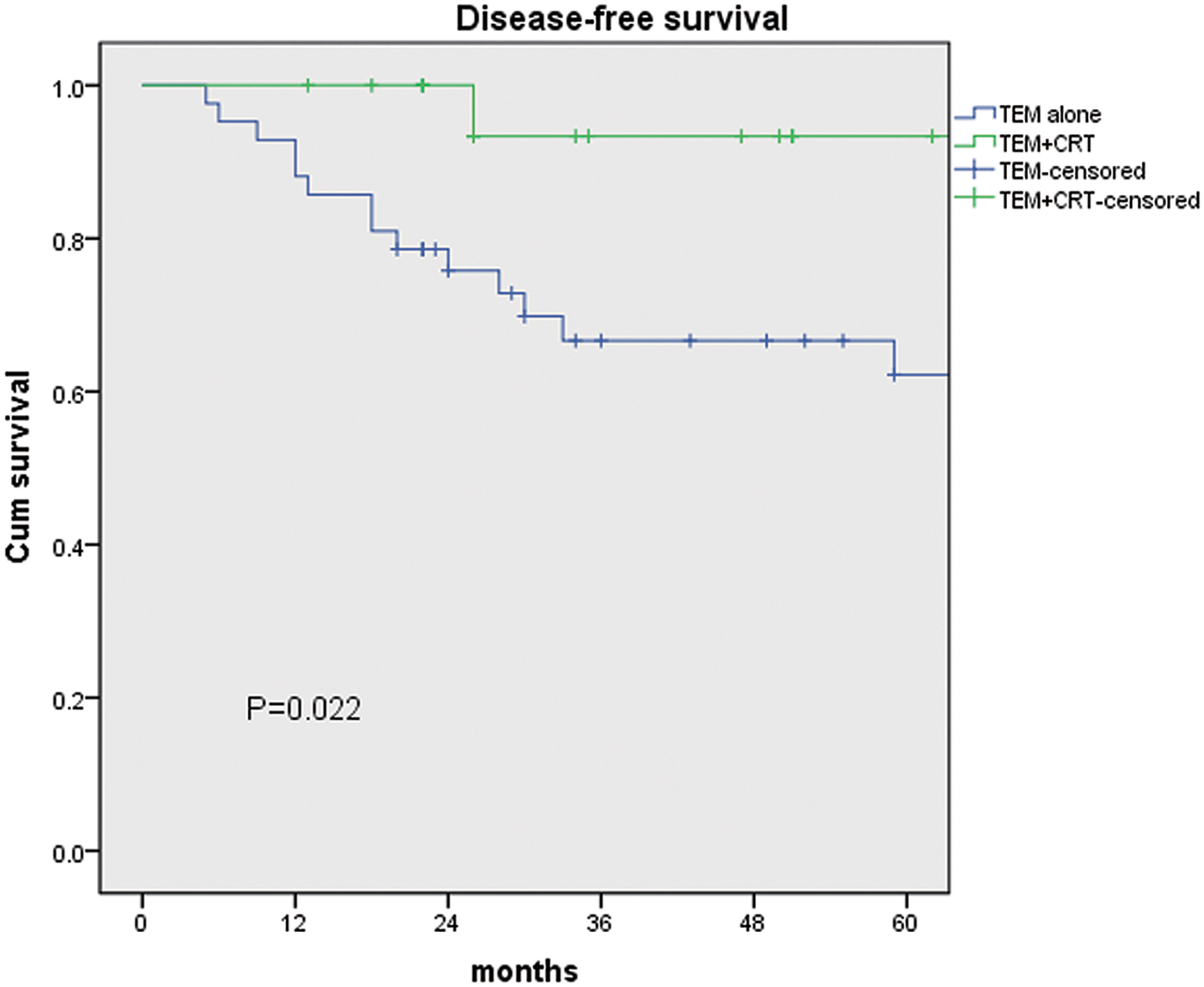
Kaplan–Meier survival curves of disease-free survival. CRT, chemoradiotherapy; TEM, transanal endoscopic microsurgery.
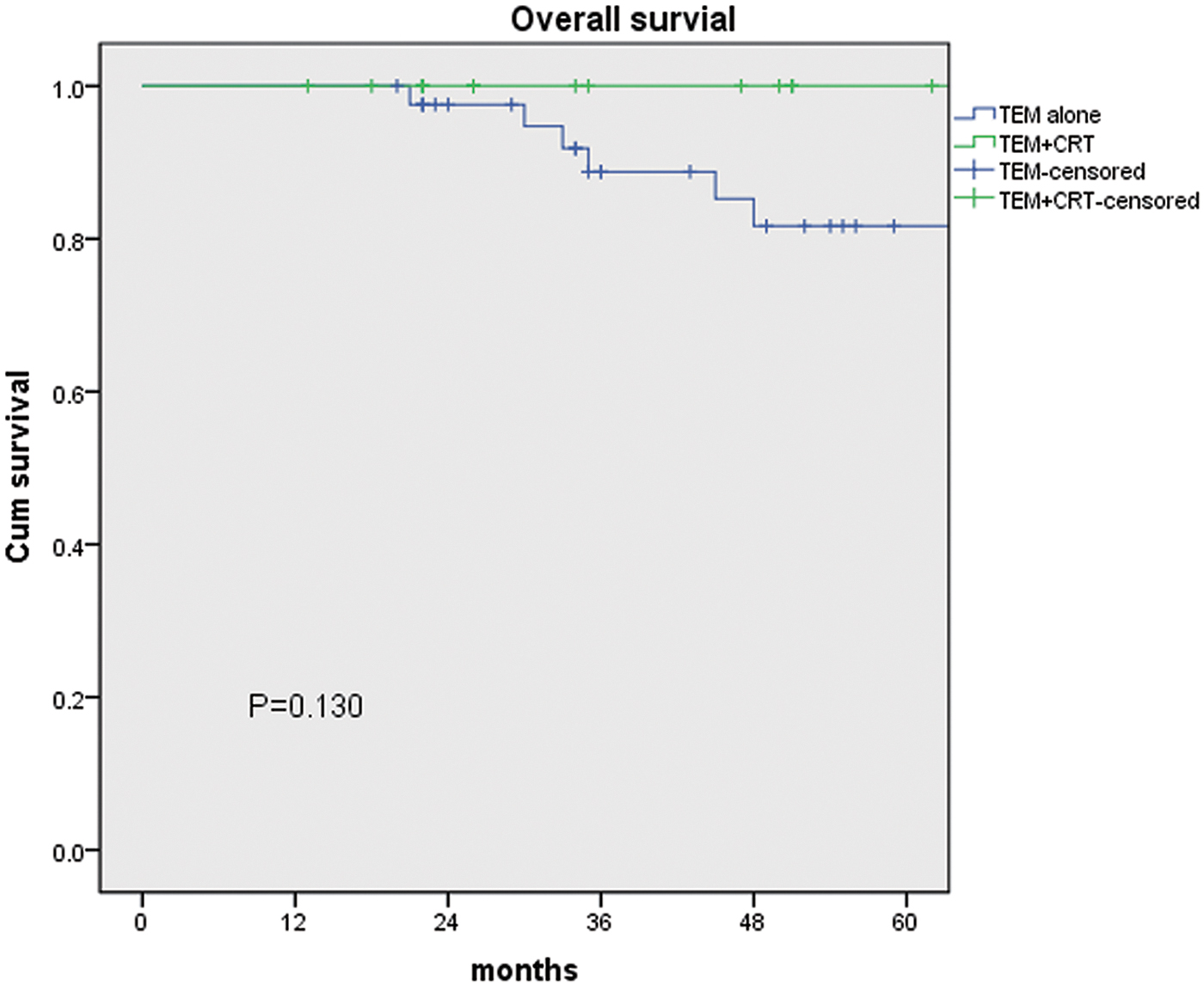
Kaplan–Meier survival curves of overall survival. CRT, chemoradiotherapy; TEM, transanal endoscopic microsurgery.
The variables of gender, age, T stage, tumor diameter, distance from anal verge, tumor differentiation, RM, LVI, perineural invasion, CEA, adjuvant CRT were used for the univariate analysis and multivariate analysis. In univariate analysis, the adjuvant CRT was only potential prognostic factors for LRFS and DFS, the age was only potential prognostic factors for OS. In multivariate analysis, there were no significant factors for OS or LRF, but adjuvant CRT (hazard ratio [HR]: 0.094; 95% confidence interval [CI]: 0.001–0.764; P = .027) was the independent prognostic factors for DFS (Table 2).
Univariate and Multivariate Analyses of Local Recurrence-Free Survival, Overall Survival, and Disease-Free Survival
CEA, carcinoembryonic antigen; CI, confidence interval; CRT, chemoradiotherapy; DFS, disease-free survival; HR, hazard ratio; LRFS, local recurrence-free survival; OS, overall survival; pT, pathological stage.
Details of patients with recurrence
Fifteen cases of recurrence were observed, of which 8 patients had isolated local recurrence, 1 patient had distant metastasis, and 6 patients had both local recurrence and distant metastasis. The mean time of recurrence was 21 (range 5–59) months. There were 10 males and 5 females, the mean age of the patients was 59 years (range 32–82). Among the 15 patients with relapses, tumors were categorized as pT1 high-risk in 9 patients, pT2 in 6. Thirteen patients developed local recurrence in TEM alone group, whereas only 1 had local recurrence in TEM+CRT group. And the rate of local recurrence was 31% and 5%, respectively (P = .025). It is worth noting that all patients with local recurrence occurred within 3 years after TEM. The 1 patient with local recurrence in TEM+CRT group occurred 26 months after TEM. The patient was operated by TEM again because the preoperative assessment was cT1N0M0 and the patient wanted to preserve anal. Of course, postoperative pathology also proved to be T1. The follow-on adjuvant therapy with concurrent CRT was performed and the survival after recurrence was 56 months by the last follow-up date. The basic information and treatment approaches of 15 patients with recurrence are shown in Table 3.
Basic Information and Treatment Approaches of 15 Patients with Recurrence
APR, abdominoperineal resection; CRT, chemoradiotherapy; DM, distant metastasis; LAR, low anterior resection; LH, laparoscopic hepatectomy; LR, local recurrence; pT, pathological stage; TEM, transanal endoscopic microsurgery.
Complications
Two of the 42 patients who received TEM alone had recorded surgery-related complications. One developed delayed healing, whereas the other developed postoperative rectal stenosis and was again treated with TEM. In 20 patients who underwent adjuvant CRT after TEM, 5 patients had CRT-related adverse events, including 4 who developed leukopenia and 1 who developed a dermal mucosal reaction. All patients were treated conservatively.
Discussion
In this study, the oncological outcomes showed a tendency that the TEM+CRT group was significantly better than the TEM alone group. Adjuvant CRT after TEM significantly improved 3-year LRFS and 3-year DFS in patients with pT1 high-risk and pT2 (93.3% versus 66.6%, P = .035; 93.3% versus 63.7%, P = .022). Moreover, the 3-year OS for patients in the TEM+CRT group was higher than that in TEM alone group (100% versus 83.3%), but this difference was not significant (P = .13), which may be related to the small sample size and the small number of deaths. In multivariate analysis, the only independent prognostic factor affecting DFS was the adjuvant CRT (HR: 0.094; 95% CI: 0.001–0.764). In this sense, the results indicated that adjuvant CRT after TEM was promising.
Both radical surgery and local excision can be used as the treatment for early rectal cancer. Local excision, however, has always been controversial in the treatment of early rectal cancer. There are two main reasons for the controversy. On the one hand, TEM only removed the primary tumor without mesorectal lymph nodes compared with radical surgery, and the occult metastatic lymph nodes in the mesorectum may increase the risk of local recurrence. Brodsky 14 showed that there is a known 5%–10% risk of occult lymph node metastases in stage T1 rectal cancer and a 20%–35% risk in those with stage T2 tumors. A recent study even suggests patients who are sensitive to CRT for early rectal cancer after neoadjuvant CRT still have an ∼20% probability of lymph node metastasis. 15 A Korean study 16 reported the 10-year local recurrence rate in patients with pT1 rectal cancer after TEM was 10%, whereas the 10-year local recurrence rate in patients underwent TME was 0% (P < .001). A Norwegian study 8 reported that the 5-year local recurrence rate after TEM was 11.4% versus 4.4% after TME in patients with T2 rectal cancer. On the other hand, precise preoperative staging is still a challenge. MRI and endorectal ultrasound (ERUS) were currently considered as the best available techniques for assessing preoperative staging of rectal cancer, but postoperative pathology often revealed a more advanced tumor than preoperative staging. MRI may miss some small metastatic lymph nodes in assessing lymph node status. Langman et al. 17 found that ∼28% metastatic nodes retrieved in 244 patients with 344 positive nodes were ≤3 mm in diameter. A study 18 found MRI accuracy to predict lymph node status was 84% (95% CI: 70–92) by comparing preoperative high-resolution MRI with a histopathological assessment of TME specimen. Moreover, another study 19 reported that accuracy of ERUS for T staging of rectal cancer according to pathology was 73.7%. In our study, 8 (31%) of the 26 cases with stage pT2 were initially diagnosed as clinical staging T1. The risk of potential lymph node metastases and the lack of accuracy of preoperative staging indicated that TEM alone was not sufficient treatment for some cases.
Adjuvant CRT with radical surgery has long been used for advanced rectal cancer to reduce the local recurrence rate. However, there is growing evidence in recent years to show that CRT combined with local excision for early rectal cancer could also provide favorable outcomes. A Japanese study 20 reported that local recurrence rate was only 2% in patients with T1 rectal cancer who underwent local excision followed by CRT at a median follow-up of 71 months. Chakravarti et al. 21 study indicated that adjuvant CRT can improve 5-year local control rate from 37% in local excision alone to 85% in LE+CRT group for early rectal cancer with high-risk pathological features (P = .03). A phase II clinical trial 22 with 10 institutions of assessing the outcomes of postoperative CRT after local excision reported that the 5-year DFS was 94% in T1 high-risk tumor and 75% in T2 lesions at a median follow-up of 7.3 years, but only 4 patients with T2 were registered. However, in T2 categories of our study, 3-year LRFS was 90.9% in TEM+CRT group and 54.5% in TEM alone group (P = .033).
Generally, TEM is an adequate treatment for T1 tumor with low-risk features, such as a clear resection margin, tumor invasion <30% of the bowel circumference, tumor size <3 cm, well to moderately differentiated and without LVI or perineural invasion. 13 Adjuvant CRT after TEM may best be suitable for patients with a high-risk feature of local recurrence and where completion TME surgery is not favored. At present, the high-risk features of local recurrence were deemed as the poor differentiation, third submucosal layer (SM3), positive resection margin, and LVI. 10 In addition to aforementioned factors, other studies have shown that local recurrence of early rectal cancer after local excision might be related to second or third submucosal layer (SM2-3), tumor diameter, perineural invasion, or residual cancer cells during local resection.23–26 Therefore, we based on the aforementioned possible risk factors to define pT1 high-risk.
Regarding the issue of complications, we observed only a small number of patients with relatively mild complications, all of them were treated conservatively, except for a case of rectal stenosis that was re-treated with TEM. The most common CRT-related complication was leukopenia, probably chemotherapy played a major role in it. Only a few of the previous studies mention serious complications related to adjuvant CRT after local excision. An England study 11 noted significant complications of radiotherapy in 2 patients (6%), including 1 with persistent radiation proctitis and the other who developed small bowel infarction. Besides, a Korean study 12 reported that 9 (10.8%) of 83 patients occurred early proctitis (Grade 2), and no patients had Grade 2 or higher late toxicities. In the Spanish study 13 of 28 patients developed complications of radiotherapy (8 Grade I, 5 Grade II) and all were managed conservatively.
In our study, with a median follow-up of 52.5 months, there were 15 (24.2%) patients of recurrence, 13 (31%) of 42 patients with stage pT1 high-risk and pT2 developed local recurrence in TEM alone group, whereas only 1 (5%) of 20 patients in TEM+CRT group had a local recurrence (P = .025), which was similar to that (4%) in those who underwent TME.12,27 Patients who should have had radical surgery due to their high-risk pathological features but declined to have it could benefit from adjuvant CRT. Therefore, the use of CRT after TEM may offer an attractive oncological result for early rectal cancer when pathological features suggested that TEM may not have been an adequate treatment. There are a few limitations to this study. First of all, the sample was inadequate and only 20 patients received adjuvant CRT after TEM. Moreover, this study is limited by the retrospective nature and the study period spanned 11 years, which resulted in incomplete pathological information of some patients. The aforementioned factors might result in the deviation of our consequences.
Conclusions
In conclusion, when the pathological findings after TEM indicated a high-risk T1 or T2 rectal cancer, adjuvant CRT after TEM could be a safe option for patients who prefer to avoid radical surgery and provide an encouraging oncological outcome. Further prospective studies were needed to evaluate and validate these results.
Footnotes
Acknowledgment
The authors thank postgraduate Haodong Li from University of California, Berkeley, with assistance statistically.
Disclosure Statement
No competing financial interests exist.
Funding Information
The project of Science and Technology Development of Jinan city (No. 201602177) and the project of Medical science and technology development of Shandong Province (No.2017WS368) supported this study.