
Abstract
Background:
Standardized protocols for laparoscopic surgery of splenic flexure cancer (SFC) have not been established yet. We described a standardized laparoscopic procedure for SFCs and examined its safety and feasibility.
Methods:
Laparoscopic colectomy for SFC was performed as follows. The sigmoid colon was mobilized to the descending mesocolon through the medial approach. After confirming the base of the inferior mesenteric artery, the left colic artery was dissected and resected at the base. Further dissection was carried out between the mesentery of the colon and the renal fascia until it exceeded the upper pole of the left kidney and the splenic flexure. The next dissection reached the white line at the lateral side and the sigmoid–descending colon junction. After making an incision at the greater omentum and gastrocolic ligament from the center of the transverse colon to the splenic flexure, the transverse mesocolon base was dissected from the inside splenic flexure for complete mobilization. This was performed by approaching from four directions toward the splenic flexure. Intestinal resection and anastomosis are performed.
Results:
This procedure was performed in 70 patients with splenic flexure colon cancer (mean age 70 years). The mean operative time was 190 minutes, and the mean blood loss was 2.0 mL. No notable perioperative or postoperative complications were noted.
Conclusions:
Safe mobilization of the splenic flexure can be achieved by approaching from four directions, and standardization of left colectomy can facilitate complete mesenteric excision.
Introduction
Splenic flexure cancer (SFC) is a malignant tumor affecting the distal third of the transverse colon and the proximal side of the descending colon. 1 It accounts for ∼3%–8% of all colon cancers and leads to colonic obstruction and worse prognosis. 2 First report of laparoscopic surgery for colon cancer was in 1991.3,4 Some of the previous studies did not find a difference in the number of harvested lymph nodes, the proximal distance, and distal distance when comparing laparoscopic surgery and open surgery. However, the laparoscopic procedure can lead to lesser postsurgical pain and shorter hospital days.5–7 In previous studies, transverse colon cancer and SFC were excluded because of technical difficulties, anatomical complexities, and low curability estimate of laparoscopic surgery.8–10
The laparoscopic approach for SFC remains to be standardized, and it is difficult and complicated. The primary concerns are the harvesting range of lymph nodes, resected colon length, vessel anastomosis, and the possibility of injury to the spleen. 11
In this study, we standardized the laparoscopic surgical procedure for SFC at the distal transverse colon or proximal descending colon and aimed to examine its safety and feasibility.
Methods
Patients and tumors
SFC was defined as a malignant tumor located between the left third of the transverse colon and 10 cm proximal descending colon. 1
From April 2011 to March 2018, laparoscopic surgeries were performed for patients with locally advanced or totally obstructing SFC. In those patients, a colon cancer diagnosis was confirmed using colonoscopy and tissue biopsy. Colonoscopic tattooing was performed on adjacent cancer. Irrigoscopy was also performed. Tumor staging was identified using computed tomography (CT) scan. Three-dimensional CT was used to identify the precise tumor and vessel locations. Also, vessel imaging was reconstructed in three dimensions. Patient data, including the body mass index (BMI), American Society of Anesthesiologists score, 12 operative time, amount of bleeding, conversion to open procedure, postoperative adverse event, duration of hospital days, pathological results, and clinical outcomes, were analyzed in a retrospective manner. To determine the tumor-node-metastasis (TNM) stage, 13 tumor size, the number of harvested lymph nodes, the length of the resected colon was noted, and pathological inspection was performed. Adjuvant chemotherapy was recommended to pathological stage III cancer patients. Patients were followed up at a 3-month interval for 5 years. They underwent physical examination, blood examination, and tumor marker testing during follow-ups. Furthermore, CT examinations were carried out every 6 months. Total colonoscopy was also performed at 1 year, 3 years, and 5 years after surgery.
This study was approved by the ethical committee of the Kobe City Medical Center General Hospital. Informed consent the surgery was obtained from all patients.
Surgical techniques and procedures
Laparoscopic surgeries were carried out by skilled surgeons at our institute., The surgery was performed under general anesthesia in the lithotomy position. The operator and a scopist stood on the patient's right side, and the first assistant stood on the left side. Five trocars were placed. The first trocar for a scope was placed on the umbilicus using the open method. After inducing 10-mmHg pneumoperitoneum, a second trocar was set in the right lower abdomen, and a third trocar was set in the right upper abdomen. Two trocars were individually set on the left upper and lower abdomen.
The patient was maintained in the Trendelenburg position and moved approximately 10° rightward to keep the operative field clear of the small intestine. The left-sided mesocolon was raised, and the retroperitoneal plane was mobilized from the promontorium using the medial-to-lateral approach. The left colic artery (LCA) and the inferior mesenteric artery were identified and exposed while preserving the left ureter and gonadal artery and vein. The LCA is clipped at its base and then divided (Fig. 1). Then, the inferior mesenteric vein (IMV) was clipped and cut near the divided LCA stump. Next, the patient's position was changed to the reverse Trendelenburg position, and the small intestine was moved. The mesenterium was raised, and the descending mesocolon was dissected from the retroperitoneal plane to the splenic flexure by the medial approach. Dissection was continued until the back of the pancreas was defined, and the inferior pole of the spleen could be viewed (Fig. 1).
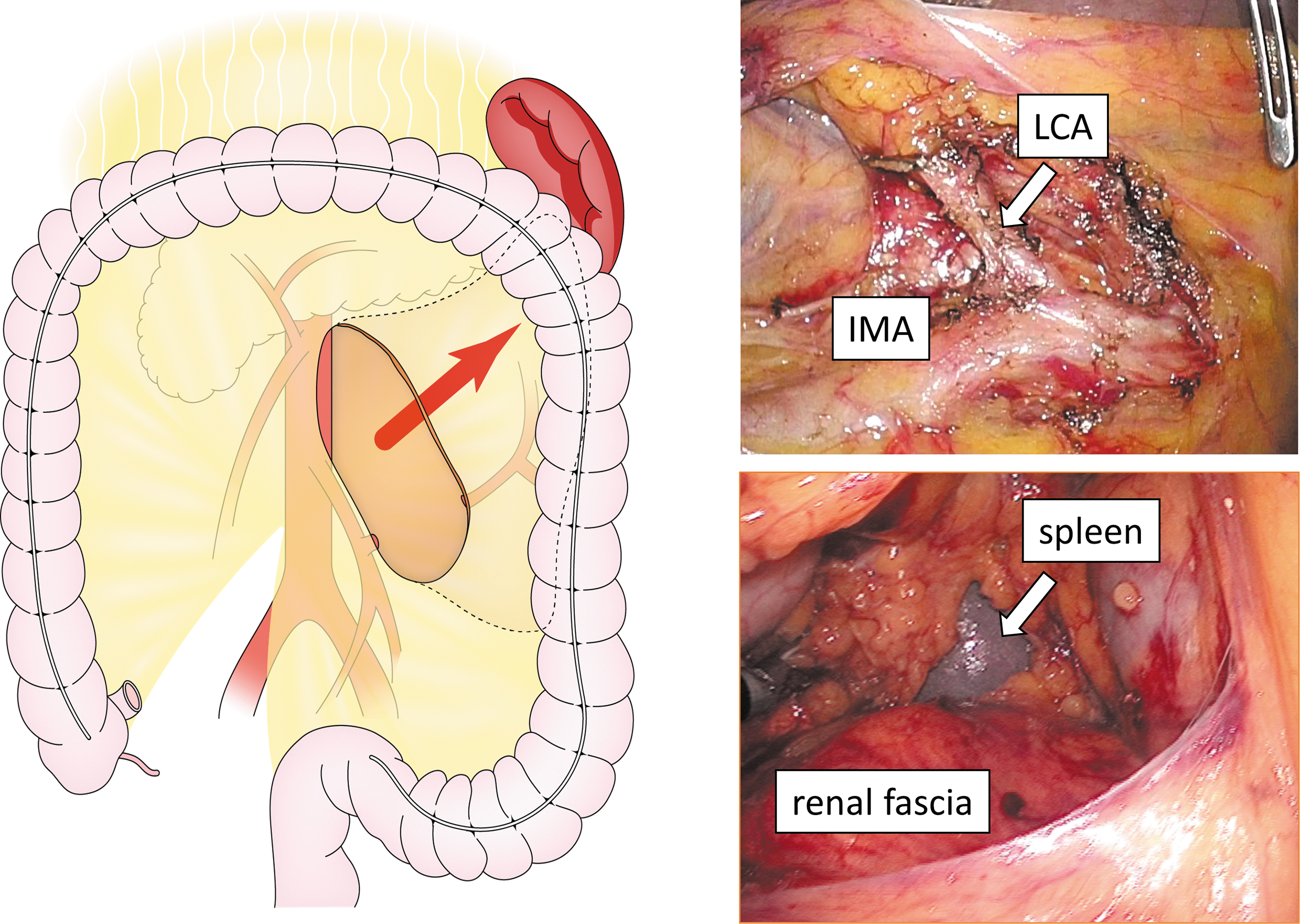
The root of IMA is skeletonized to dissect lymph nodes. Dissection is performed till the inferior pole of the spleen can be viewed. IMA, inferior mesenteric artery.
The descending colon was separated from the lateral abdominal wall toward the flexure of the spleen (Fig. 2).

The descending mesocolon is separated from the retroperitoneal plane to the splenic flexure.
Next, the omental bursa was opened by dissecting the greater omentum from the transverse colon to the splenic flexure without injured the gastroepiploic artery (Fig. 3).
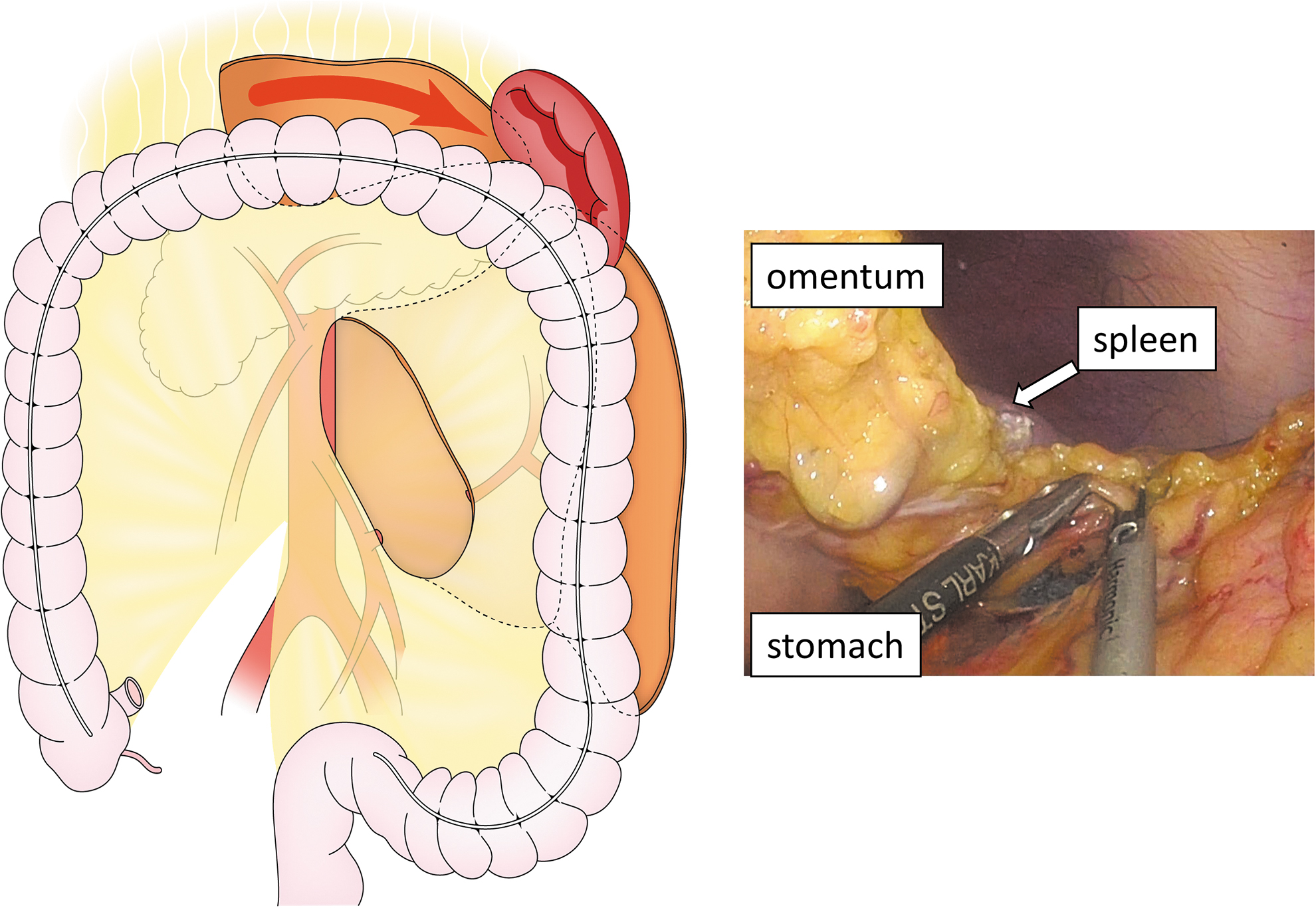
The omental bursa is opened by dissecting the greater omentum from the middle of the transverse colon to the splenic flexure.
The IMV was redivided at the inferior edge of the pancreas, and the left branch of the middle colic artery (MCA) was also divided at its root. If the accessory MCA (AMCA) was found, it was also divided. Then, the transverse mesocolon was divided at the inferior edge of the pancreas toward the splenic flexure (Fig. 4). In brief, splenic flexure mobilization was completed by approaching from four directions toward the splenic flexure.

The transverse mesocolon is divided at the inferior border of the pancreas to the splenic flexure.
The mobilized splenic flexure colon was withdrawn through a small incision of the umbilicus. After transecting the colon, extracorporeal anastomosis was performed by a functional end-to-end anastomosis technique.
Results
Our minimally invasive procedure was performed in 70 patients with SFC from April 2011 to December 2017. The characteristics of these patients are summarized in Table 1. Complete mesocolic excision (CME) and central vascular ligation (CVL) were performed in all cases. Cases included were 40 males and 30 females, with a mean age of 70 years (48–85 years), a mean BMI of 23.3 kg/m2, a mean tumor size of 3.8 cm, and a mean surgery time of 190 minutes (150–295 minutes). The average amount of bleeding was 2.0 mL. Conversion to open procedure was not shown.
Characteristics of Patient and Tumor
BMI, body mass index.
AMCA was found in 12 patients, and it was divided. No intraoperative complications, accidental symptoms, or postoperative complications (Clavien–Dindo classification ≥III) were observed. The 30-day mortality rate was 0%. The mean duration of hospital stay was 8.5 days (range 6–19 days).
A total of 35 patients had metastasis in the lymph nodes. The mean length of the resected colon was 24.3 cm (range 18.9–33.0 cm), and the distance of the proximal margins from the tumor was 10.5 cm, and the distal was 11.5 cm. The mean number of lymph nodes harvested was 18.8 (range 12–29). Two patients had recurrence during follow-up (Table 2).
Outcomes of Surgery
AMCA, accessory middle colic artery; C–D, Clavien–Dindo classification.
Discussion
This study described a standardized laparoscopic surgical procedure for left transverse and descending colon cancers and examined its safety and feasibility. Because of the low frequency of SFC and the anatomical complexity, surgical anatomy considerations are very important for the standardization of the approach. CME with CVL is the optimal surgical procedure for patients with colon cancer. 14 The LCA and left branches of the MCA are the vessels that supply the splenic flexure colon; however, it is technically complex to identify the middle and LCAs and veins. SFCs were previously excluded from randomized controlled trials such as the COST, COLOR, CLASICC, and Barcelona trials.6,15 Interestingly, the anatomical features of splenic flexure were reported through the embryological aspect. 16 Understanding the anatomy of the splenic flexure is essential for CME and CVL. Also, CME is performed to dissect the mesentery, including the left branch of the MCA, the LCA, and the IMV as well as the lymph nodes. As mentioned previously, the lymph node spread in SFC is important, suggesting the oncological efficacy of segmental resection. Segmental resection is effective for early-stage SFC because there are few lymph nodes along the left branch of the MCA and MCA. 8 In our procedure, the lymph nodes dissection was enough to perform CME and CVL. Besides, laparoscopic mobilization for the splenic flexure is carried out without identifying the MCA. 17 Isolation of the middle colic artery and veins laparoscopically requires advanced techniques. Our study participants underwent ligation at the origin of the left branch of the MCA and LCA, as a fine laparoscopic view was supplied. In several cases, the AMCA was identified and safely isolated at its origin. Therefore, no major complications or conversions to open were observed. Another key hurdle that prevents laparoscopic splenic flexure resection from becoming a standardized approach is the resection of the injured spleen as a risk factor. In SFCs, the likelihood of splenectomy is more frequent than in cancers elsewhere in the colon, and mortality and morbidity are also high. 11
Efficient mobilization of the splenic flexure is needed for taking out the mobilized colon for extracorporeal anastomosis. No study has compared extracorporeal and intracorporeal anastomoses in laparoscopic surgery for the splenic flexure, although most series suggests extracorporeal anastomosis. Meanwhile, intracorporeal colon resection and anastomosis may become one of the anastomotic procedures. 18 One of the major complications of this procedure is acute postoperative pancreatitis of the distal pancreas. Separation of the transverse mesocolon and pancreas rarely causes acute pancreatitis. 19 In this four-direction approach, pancreatic damage or pancreatitis is unlikely because the transverse mesocolon and the pancreas are detached with a laparoscopic fine view.
The recurrence rate of SFC in a previous study was 8.5%. 20 In our study, with a mean follow-up period of 33 months, only two liver metastases were observed, comparatively better than that in previous reports.
To determine the oncological effectiveness of this four-directions approach, large-scale studies of laparoscopic resection for SFC are required.
Conclusion
This study concludes that a laparoscopic approach that mobilizes the splenic flexure from four directions may be feasible and safe for SFC. Laparoscopic resection for SFC yields the same result as those elsewhere in the colon.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.